The MacArthur Foundation has announced its new class of Fellows, the recipients of what are commonly called the “Genius Awards.” Among the recipients is Dorothy Roberts, the self-styled popularizer of the term “racial disproportionality” and creator of the term “the family policing system.” According to the Director of the Program, “The 2024 MacArthur Fellows pursue rigorous inquiry with aspiration and purpose. They expose biases built into emerging technologies and social systems….” It’s hard to understand how this term can be applied to an author who wrote that the “family-policing system terrorizes Black families because that’s what it is designed to do ” despite also stating that child welfare systems excluded Black children from their inception until the second half of the twentieth century. The choice of Roberts only exposes the bias and lack of rigor–or alternatively the sheer ignorance– of the MacArthur Foundation. As an illustration, I am reposting my 2022 review of Roberts’ most recent book, Torn Apart: How the Child Welfare System Destroys Black Families–and How Abolition Can Build a Safer World.
In her 2009 book, Shattered Bonds: The Color of Child Welfare, Dorothy Roberts drew attention to the disproportional representation of Black children in foster care and child welfare in general and helped make “racial disproportionality” a buzzword in the child welfare world. In her new book, Torn Apart: How the Child Welfare System Destroys Black Families–And How Abolition Can Build a Safer World, Roberts revisits the issues addressed in Shattered Bonds and creates a new buzzword, renaming child welfare as the “family policing system.” Those who liked Shattered Bonds will likely love Torn Apart. But those who value accuracy in history or in data will find it to be sadly misguided, although it does make some valid points about flaws in the U.S. child welfare system.
Roberts starts with a horrific anecdote about a mother, Vanessa Peoples, who was doing everything right–she was married, going to nursing school, about to rent a townhouse and was even a cancer patient. But Peoples attracted the attention of both the police and child welfare and ended up hogtied and carted off to jail by police, placed on the child abuse registry, and subjected to months of monitoring by CPS after she lost sight of her toddler at a family picnic when a cousin was supposed to be watching him. But citing these extreme anecdotes as typical is very misleading. This particular story has been covered in numerous media outlets since it occurred in 2017 and continues to be cited regularly. One can counter every one of these horrific anecdotes with a story of a Black child who would have been saved if social workers had not believed and deferred to the parents. (See my commentary on the abuse homicides of Rashid Bryant and Julissia Batties, for example).
Roberts’ book restates many of the old myths that have been plaguing child welfare discussions as of late and that seem to have a life of their own, impervious to the facts. Perhaps the most common and pernicious is the myth that poverty is synonymous with neglect. Roberts embraces this misconception, suggesting that most neglect findings reflect parents who are too poor to provide adequate housing, clothing and food to their children. But parents who are found to have neglected their children typically have serious, chronic mental illness or substance use disorders that severely affect their parenting, and have refused or are unable to comply with a treatment plan. Many are chronically neglectful, resulting in children with cognitive and social deficits, attachment disorders, and emotional regulation problems. Commentator Dee Wilson argues based on his decades of experience in child welfare that “a large percentage of neglect cases which receive post-investigation services, or which result in foster placement, involve a combination of economic deprivation and psychological affliction…., which often lead to substance abuse as a method of self-medication.” Perhaps the strongest argument against the myth that poverty and neglect are one and the same is that most poor parents do not neglect their children. They find a way to provide safe and consistent care, even without the resources they desperately need and deserve.
Roberts endorses another common myth–that children are worse off in foster care than they would be if they remained in their original homes. She argues that foster care is a “toxic state intervention that inflicts immediate and long-lasting damage on children, producing adverse outcomes for their health, education, income, housing, and relationships.” It is certainly true that foster youth tend to have bad outcomes in multiple domains, including education, health, mental health, education, housing and incarceration. But we also know that child abuse and neglect are associated with similar poor outcomes. Unfortunately, the research is not very helpful for resolving the question of whether these outcomes are caused by the original child maltreatment or by placement in foster care. We cannot, of course, ethically perform a controlled study in which we remove some children and leave a similar set of children at home. We must rely on studies that use various methodologies to disentangle these influences, but all of them have flaws. Roberts cites the study published in 2007 by Joseph Doyle, which compared children who were placed in foster care with children in similar situations who were not. Doyle found that children placed in foster care fared worse on every outcome than children who remained at home. [Update added October 2024: A newer study, reflecting current foster care policy and the more typical state of Michigan, found the opposite result.] But focusing on marginal cases* leaves out the children suffering the most severe and obvious maltreatment. In a recent paper, Doyle, along with Anthony Bald and other co-authors, states that both positive and negative effects have been found for different contexts, subgroups, and study designs.
There is one myth that Roberts does not endorse: the myth that disproportional representation of Black children in child welfare is due to racial bias in the child welfare system, rather than different levels of maltreatment in the two populations. After an extensive review of the debate on this issue, Roberts concludes that it focused on the wrong question. In her current opinion, it doesn’t matter if Black children are more likely to be taken into foster care because they are more often maltreated. “It isn’t enough,” she states, “to argue that Black children are in greater need of help. We should be asking why the government addresses their needs in such a violent way, (referring to the child removal). Roberts was clever to abandon the side that believes in bias rather than different need as the source of disparities. The evidence has become quite clear that Black-White disparities in maltreatment are sufficient to explain the disparity of their involvement in child welfare; for example Black children are three times as likely to die from abuse or neglect as White children. As Roberts suggests and as commentators widely agree, these disparities in abuse and neglect can be explained by the disparities in the rates of poverty and other maltreatment risk factors stemming from our country’s history of slavery and racism. Unfortunately, Roberts’ continued focus on these disparities in child welfare involvement will continue to be used by the many professionals who are working inside and outside child welfare systems all over the country to implement various bias reduction strategies, from implicit bias training to “blind removals.”
In Part III, entitled “Design,” Roberts attempts to trace the current child welfare system to the sale of enslaved children and a system of forced “apprenticeship” of formerly enslaved Black children under Jim Crow, whereby white planters seized custody of Black children from their parents as a source of forced labor.** As she puts it, “[t]hroughout its history US family policy has revolved around the racist belief that Black parents are unfit to raise their children. Beginning with chattel slavery and continuing through the Jim Crow, civil rights, and neoliberal eras, the white power structure has wielded this lie as a rationale to control Black communities, exploit Black labor, and quell Black rebellion by assaulting Black families.” In other passages she adds other groups to the list of victims, adding “Indigenous, immigrant and poor people to the list of communities that are being controlled by the “family policing system.” But most of her statements refer to Black victims only.
Roberts’ attempt to connect slavery and Jim Crow practices with child welfare systems highlights a major flaw of the book. She herself explains that due to racism the child welfare system served only White children when it emerged in the nineteenth century with the creation of child protection charities and the passage of state laws allowing maltreated children to be removed from their homes and placed in orphanages. Foster care was established in the middle of the century and also excluded Black children. The system did not begin serving Black children until after World War II, so it is difficult to understand how it could stem from slavery and Jim Crow practices. It seems much more plausible that the child welfare system arose from basically benevolent concerns about children being maltreated, and that with the rise of the civil rights movement, these concerns were eventually extended to Black children as well.
While Black children’s representation as a share of foster care and child welfare caseloads rose rapidly starting in the 1960’s, and Black children are much more likely to be touched by the system than White children, the system still involves more White than Black children. According to the latest figures, there were 175,870 White non-Hispanic children in foster care (or 44 percent of children in foster care) and 92,237 Black (non-Hispanic) children in foster care, or 23 percent of children in foster care. Moreover, the disparity between Black and White participation in child welfare and foster care as a percentage of the population seems to be decreasing.*** So the idea that this whole system exists to oppress the Black community and maintain white supremacy seems farfetched.
Roberts’ attempt to make Black children the focus of the book results in some awkward juxtapositions, like when she admits that though the Senate investigation of abuses by a for-profit foster care agency called MENTOR “highlighted cases involving white children, we should remember that Black children are more likely to experience these horrors in foster care—not only because Black children are thrown in foster care at higher rates, but also because government officials have historically cared less about their well-being.” A page later she states that the “child welfare system’s treatment of children in its custody is appalling but should come as no surprise. It is the predictable consequence of a system aimed at oppressing Black communities, not protecting Black children.” It is hard to understand how White children being maltreated in bad placements supports this narrative.
Fundamental to Roberts’ critique is her system is “not broken.” “Those in power have no interest in fundamentally changing a system that is benefiting them financially and politically, one that continues to serve their interests in disempowering Black communities, reinforcing a white supremacist power structure, and stifling calls for radical social change.” Even if one believes there is a white supremacist power structure, it is hard to see the direct connection between the abuses Roberts is highlighting and the disempowerment of Black communities; it seems more likely that the more abusive the system, the more protests it would generate. And at a time when the federal government and some of the wealthiest foundations and nongovernmental organizations are echoing much of Robert’s rhetoric, her reasoning seems particularly off-target.
Roberts makes some valid criticisms of the child welfare system. Her outrage at the terrible inadequacies of our foster care system is well-deserved. She is right that “The government should be able to show that foster care puts Black children [I’d say “all children”] on a different trajectory away from poverty, homelessness, juvenile detention, and prison and toward a brighter future.” Any society that removes children from their parents needs to be responsible for providing a nurturing environment that is much, much better than what they are removed from. And we are not doing that. As Roberts states, “The state forces children suffering from painful separations from their families into the hands of substitute caretakers…..who often have unstable connections, lack oversight and may be motivated strictly by the monetary rewards reaped from the arrangement.” As a foster care social worker in the District of Columbia, I was driven to despair at my inability to get my superiors to revoke the licenses of such foster parents; the need for “beds” was too great to exclude anyone was not actually guilty of abuse or severe neglect. Roberts is also right to be concerned the outsourcing of foster care to private for-profit organizations that may be more concerned with making money than protecting children, sometimes resulting in scandals like the one involving MENTOR Inc., which was found to hire unqualified foster parents and fail to remove them even after egregious violations like sexual assault.
Roberts also raises valid concerns about children being sent to residential facilities, often out of state, that resemble prisons rather than therapeutic facilities. But she ignores the need for more high-quality congregate care options for those children who have been so damaged by years of maltreatment that they cannot function in a foster home, no matter how nurturing. Instead, she repeats the usual litany of scandals involving deaths, injuries, fights and restraints, without noting the undersupply of truly therapeutic residential settings, resulting in children sleeping in office, cars, and hotels or remaining in hospital wards after they are ready for discharge. Ironically, she supports defunding the system, even if that would mean even worse situations for these children.
Roberts decries the fact that parents sometimes relinquish custody of their children in order to get needed residential care, arguing that “rather than providing mental health care directly to families, child welfare authorities require families to relinquish custody of children so they can be locked in residential treatment centers run by state and business partnerships.” That statement is completely backwards. The child welfare system does not provide mental health services but, like parents, it often struggles to secure them for its clients. Some parents are forced to turn to the child welfare system because their insurance will not pay for residential care for their children. That is not the fault of child welfare systems, which clearly do not want to take custody of these children. The underlying problem is the lack of adequate mental health care (including both outpatient and residential programs), which has destructive consequences for the foster care system. This is exacerbated by the lack of parity for mental health in health insurance programs. It’s hard to believe Robert is unaware of these well-known facts.
Roberts is correct that parents as well as children are shortchanged by inadequacies in our child welfare program, such as the “cookie cutter” service plans which often contain conflicting obligations that are difficult for struggling parents to meet. But she is wrong when she says that parents need only material support, not therapeutic services. But this error flows logically from her concept of neglect as simply a reflection of poverty. In fact, many of these parents need high-quality behavioral health services and drug treatment, which are often not available because of our nation’s mental health crisis, as well as the unwillingness of taxpayers and governments at all levels to adequately fund these services.
In her final chapter, Roberts concludes that, like the prison system, the child welfare system cannot be repaired because it exists to oppress Black people. “The only way to end the destruction caused by the child welfare system is to dismantle it while at the same time building a safer and more caring society that has no need to tear families apart.” In place of family policing, Roberts favors policies that improve children’s well-being, such as “a living wage and income support for parents, high-quality housing, nutrition, education, child care, health care; freedom from state and private violence; and a clean environment.” I agree with Roberts that aid to children must be expanded. The US is benighted when compared to many other Western countries that invest much more heavily in their children through income support, early childhood and K-12 education, healthcare, and housing. But family dysfunction occurs even if a family’s material needs are met. That is why every other developed nation has a child welfare system with the authority to investigate maltreatment allegations and assume custody of children when there are no other options. Moreover, some of the countries with the strongest safety nets for children also have higher percentages of children living in foster care than the United States.****
Torn Apart is a skewed portrait of the child welfare system. In it Roberts restates the common but easily discredited myths that poverty is synonymous with neglect and that foster care makes children worse off than they would have been if left at home. The underlying flaw in her account is the idea that this system exists to repress the Black community, even though it was established solely for the protection of White children. Roberts makes some valid criticisms of child welfare systems and how they shortchange the children and families they are supposed to help. But when she talks of dismantling child protection, she is proposing the abandonment of abused and neglected Black children in homes that are toxic to them, an abandonment that will perpetuate an intergenerational cycle of abuse and neglect. These children are our future; abandoning their well-being to prioritize that of their parents is a bad bargain with history.
*Doyle’s study included only those cases that would have resulted in foster placement by some investigators and not by others, leaving out the cases in which children were in such danger that all investigative social workers would agree that they should be placed.
**In various places, she also attributes it to different combinations of slavery and apprenticeship of Black children with the transfer of Native American children to boarding schools, the exclusion of Black children from charitable aid and the servitude of impoverished White children.
***A recent paper reports that disparities between Black and White children began to decrease in the twenty-first century in nearly every state, closing entirely in several Southern states.
****Unicef’s report, Children in Alternative Care, shows that Denmark has 982 children in “alternative care” per 100,000 and Sweden has 872 per 100,000, compared to 500 per 100,000 for the United States.
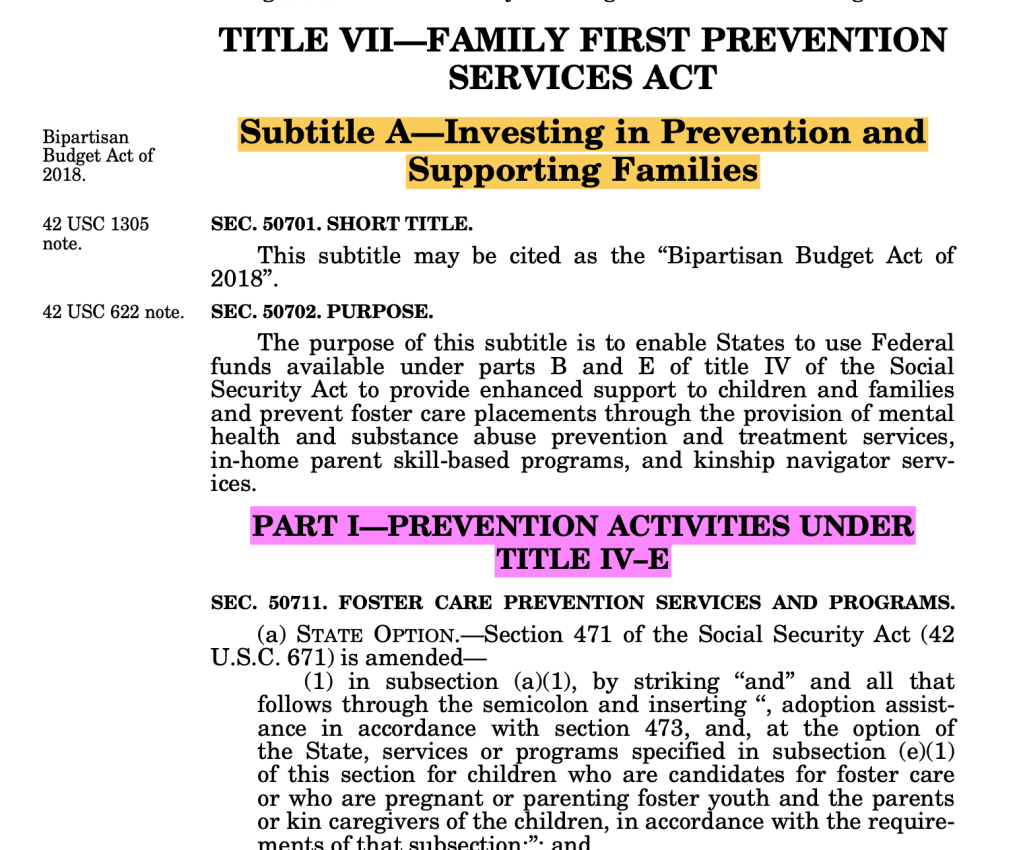
On May 22, 2024, the Senate Finance Committee (SFC) held a hearing entitled “The Family First Prevention Services Act [FFPSA]: Successes, Roadblocks, and Opportunities for Improvement.” The hearing focused on Part I of FFPSA, which is titled “Prevention Activities Under Title IV-E.” In his opening statement, Senator Ron Wyden, the prime author of the Act along with the late Orrin Hatch, recognized that FFPSA has so far not had the anticipated effect. “Six years on,” he acknowledged, “many states are still not taking advantage of the funding available to them.” He suggested that the problems were due to foot-dragging by the feds and states. But Wyden was wrong. The problem is not with the implementation of FFPSA but in the content of the bill itself. States have been hard-put to devise plans for implementing the new services because the bill was designed to fix a problem that did not exist–the alleged absence of child welfare services designed to help families stay together.
Sometime in the early years of the current century, a group of powerful advocates who thought that too many children were being placed in foster care came up with a proposal for change that they called “child welfare finance reform.” They thought the existence of a dedicated funding source for foster care and not for services to families that might keep children out of care impeded the provision of these services and might even provided an incentive to place children in foster care. A Google search for the earliest use of the term “child welfare finance reform” produced a 2010 report by the influential Casey Family Programs, entitled The Need for Federal Finance Reform. In that paper, Casey stated:
the major federal funding source for foster care, Title IV-E, primarily pays for maintaining eligible children in licensed foster care, rather than providing services for families before and after contact with the child welfare system. The fact that no IV-E funding can be used for prevention or post-reunification services has created a significant challenge to achieving better safety and permanency outcomes for children.
The idea of allowing Title IV-E to fund “prevention” or post-reunification services took hold. It was initially tested using waivers authorized between 2012 and 2014 to allow selected states to use Title IV-E funds to implement “evidence based practices” to prevent foster care placement. Despite the underwhelming results of these demonstration programs,1 FFPSA was introduced in 2016 in the House and Senate by the leadership of the House Ways and Means and Senate Finance Committees. The law was enacted in February 2018 as part of the federal Bipartisan Budget Act of 2018 (P.L. 115-123). It expanded the allowable uses of Title IV-E funding, formerly used to pay only for foster care, to include what the Act called “Prevention Services,” meaning services to prevent foster care.2 These services were defined to include mental health services, substance abuse treatment, and “in-home parenting skills training.”
In the recent hearing, Senator Wyden explained his view of the need for FFPSA and what it actually did.
Sometimes, in order to prevent the need for foster care, mom and dad might need a little help. Maybe a parent needs mental health care or substance use disorder treatment, or parenting training and support, or maybe the family needs to do family therapy. … So under Family First, we created new federal funding for those services.
Wyden’s formulation of the issue suggests that these mental health and parenting services and drug treatment were not available before FFPSA. But is simply not true. Mental health care, substance abuse treatment, and parenting training and support were all being provided with the help of federal funds — but just not through Title IV-E. States had other sources of federal reimbursement for these programs, such as Title IV-B, the Social Services Block Grant, and TANF. But above all, these services were funded by Medicaid, a federal entitlement program that receives the same federal match as Title IV-E. Because most parents involved with child welfare are covered by either Medicaid or (more rarely) private insurance, they could be referred to these services. These referrals were part of a set of child welfare services often called “in-home services,” “family preservation services,” “intact family services,” or “family maintenance services.” As the Child Welfare Information Gateway, an information clearinghouse of the U.S. Children’s Bureau, put it in a 2021 Issue Brief:
Most children involved with the child welfare system are not separated from their families but instead receive services while living at home. These child welfare “in-home services” are designed to strengthen and stabilize families that come to the attention of child protective services (CPS).
While FFPSA had taken effect when the issue brief was published, few states had implemented it and almost no money had been spent, so it is a testament to the prevalence of in-home services before any effects of FFPSA. In-home services were and are generally provided to families after an investigation found that the children are “at risk,” but not in immediate danger, which would require removal. A key element of in-home practice is safety assessment and management, which was given short shrift by the writers of FFPSA. Another key element was interventions for specific problems, like drug treatment, mental health services and age-specific parenting skills training–interventions which were mostly provided through referrals to other agencies.
I’m not saying that all families were getting all the services they needed. There is a longstanding undersupply of drug treatment and mental health services, as well as domestic violence services, which were inexplicably left out of FFPSA. Equally problematic is the poor quality of many of the services available, as many high-quality providers choose not to accept Medicaid due to low reimbursement rates and excessive paperwork. Federal reviews have found that child welfare agencies across the country have problems in accessing the services provided by other agencies, including long waiting lists, lack of quality providers, and lack of specialized services in rural areas. Perhaps the drafters of FFPSA assumed that it would allow state child welfare agencies to create their own supply of drug treatment, mental health and parenting programs strictly for child welfare clients.
But the use of Title IV-E funds authorized by FFPSA to add to the supply of services covered by Medicaid and other funders was soon blocked when Congress itself (with the involvement of the House Ways and Means Committee, which had also advanced FFPSA) decided that Title IV-E to be the “payer of last resort” for “Title IV-E prevention services.” This means that Title IV-E cannot be used to pay for any service that would have been paid for by another provider (like Medicaid) before FFPSA was passed. This change to Title IV-E of the Social Security Act was added on to a bill to address the opioid crisis that passed on October 24, 2018, apparently after members of Congress realized that FFPSA was unclear on what program paid first. It is hard to believe that the drafters of the bill did not anticipate this issue. since most of the other funding sources (like Medicaid and Title IV-B) are also under the jurisdiction of Senate Finance and House Ways and Means Committees. In any case, it is unclear why they did not move to amend FFPSA as soon as they recognized the problem.
Making matters worse, FFPSA required that all funded programs be “promising,” “supported,” or “well supported” as defined by a list of criteria set forth in the law, and that half of the funds be spent on programs that meet the more stringent criteria for being “supported” or “well supported.” This meant that some of the poorer and more rural states states as well as Indian tribes, were hard-put to find programs that existed in their states, were culturally appropriate and also met the criteria for being funded. Ironically, while FFPSA’s criteria for methodology are strict enough to rule out many programs, the bar for being considered “promising,” “supported” or “well-supported” is actually very low for any program that meet evaluation criteria. Many of the programs selected have few and small impacts, and common evidence-based services like Cognitive Behavioral Therapy and buphenorphine therapy for Opioid Use Disorder are not included in the list of practices that have been approved by the Title IV-E Prevention Services Clearinghouse. But that is a subject for another post.
The result of all this confusion and red tape was that the bill that was supposed to have a momentous impact, giving rise to an explosion of services for children at risk of being taken into foster care and their parents, has arrived with a whimper rather than a bang. ACF estimated that only 18,400 children in the entire country were served by Title IV-E prevention services programs in FY 2023, five years after it took effect, at a cost of $167 million. That’s hardly the massive impact that Wyden was expecting. It’s not hard to understand why the effect of FFPSA has been so underwhelming. States have been hard-put to find programs that meet the Act’s evidence requirements and are not already paid for by Medicaid.
What could Congress have done instead? They could have made changes to Medicaid to improve options for parents at risk of losing their children to foster care. Even if they preferred to change Title IV-E, they could have extended funding to case management, which the core service provided by child welfare and the backbone for all the other services that child welfare provides–case management. Case management is the only service that the child welfare system usually provides directly rather than through referrals and for which it actually pays. Child welfare social workers are above all case managers. It is the case manager who refers the parent to the other providers, motivates them to continue to participate, monitors their participation by communicating with the service provider, and most importantly, monitors the safety of the children in the home. One could say that in-home services is the main program that clients receive and encompasses other programs to which they may be referred.
The funding of case management through Title IV-E might have helped address an ominous development that is occurring in some large states–the simultaneous decline in both foster care and in-home cases. While, FFPSA was supposed to encourage states to substitute in-home services for foster care, there is evidence from some large states that endangered children are being left at home with no services or monitoring at all. (The evidence is limited because FFPSA does not require states to report on the number of cases that are opened for in-home services and how many children and adults are receiving such services.) The abandonment of these at-risk children may be due in part to the workforce crisis afflicting child welfare and other human services, which results in unmanageable caseloads and possibly pressure not to open cases. But the provision of matching funds for case management would help states provide higher salaries and better conditions, which might help increase the workforce.
It appears that Chairman Wyden still does not recognize the fundamental fallacy behind FFPSA’s “prevention services” and the problems it caused. In his opening statement at the hearing, he lamented that “last year, the federal government spent just $182 million on prevention services, while we spent over $4 billion on traditional foster care. Clearly, priorities are out of whack. The government can and must do better to get this funding out the door to states that ask for it.” But the bill’s drafters should look to their own responsibility before he blames “the government” for its implementation. It’s time to fix the flaws in FFPSA which stem from the fundamental misconception at its heart,
Notes
An evaluation that incorporated the final state reports found that 80 percent of the interventions studied has mixed positive and “unexpected” findings. About one-fifth had statistically significant positive effects across all major outcomes on which they were evaluated…” ↩︎
This title is somewhat deceptive as what is being prevented is placement in foster care, which is an intervention rather than a behavior. It is kind of strange to direct one intervention at another intervention provided by the same agency. If they want to prevent foster care, they can just not place kids in it! What they should have targeted for prevention is child abuse and neglect. ↩︎
A new report by the Senate Finance Committee concludes that children in residential treatment facilities routinely suffer harms like sexual and physical abuse, unsafe and unsanitary conditions, and lack of needed therapy. Further, it concludes that these harms are endemic to residential care itself. While the fact that some residential care facilities are substandard and cause harm to children is undisputed, the SFC’s study is poorly designed and should not be used as the basis of policy. It is based on facilities run by only four companies and cannot be used to make generalizations about residential care as a whole. Both the study design and the findings of the SFC report appear to stem from a preconceived conclusion and not on a desire to describe the actual landscape of residential care for America’s youth who need intensive behavioral health care.
On June 12, 2024, the Senate Finance Committee (SFC) released a report called Warehouses of Neglect: How Taxpayers are Funding Systemic Abuse in Youth Residential Treatment Centers. The report was based on an investigation of what it calls residential treatment facilities (RTF’s) operated by four large companies, “each owning facilities with a history of public abuse and neglect allegations and a substantial facility footprint.” It does not define RTF’s, but the term clearly refers to facilities that provide behavioral health services in a residential context to children with funding from programs under SFC jurisdiction, mainly Medicaid and foster care funds under Title IV-E of the Social Security Act. The four companies include three profit making corporations (United Health Services, Acadia Healthcare, and Vivant Behavioral Healthcare), and one nonprofit, Devereux Advanced Behavioral Health.
The report describes a pattern of poor conditions and abusive practices that the SFC staff observed by reviewing media articles and company documents, supplemented by interviews with senior leaders in the four companies and visits to several facilities not operated by these companies.1 These conditions and practices include sexual and physical abuse by staff; the inappropriate and often abusive use of restraints and seclusion; staff who are unqualified and inadequately trained staff or who routinely fail to discharge their duties, leading sometimes to tragic results; “non-homelike,” unsanitary and unsafe conditions; failure to provide the treatment that children need and that states are paying for; failure to maintain connections between children and their communities and to make adequate discharge plans; use of technology to monitor children that is more appropriate to detention facilities than therapeutic settings; and the absence of adequate oversight by state and federal authorities.
The report raises valid concerns about private businesses being involved in services to the most fragile young people. Several details stand out, all of them involving the company called Vivant and its CEO, John “Jay” Ripley. Ripley is the former CEO of Precision Tune Auto Care and and cofounder of BGR the Burger Joint. Ripley previously founded Sequel Youth and Family Services, which became known for the death of 16-year-old Cornelius Frederick while being restrained at a Michigan facility in 2020 and allegations of abuse and neglect at other Sequel facilities. In 2021, according to the report, Sequel closed half of its facilities and sold the other half, including 13 facilities that it sold to Vivant, Ripley’s new company. VIvant in turn hired many former Sequel executives and staff. In a video made by the University of Baltimore’s Merrick School of Business, Ripley explained that “you can make money in this business if you control staffing.” Ripley does not seem like the kind of person who should be running facilities dedicated to healing the most vulnerable young people.
The SFC report might have been a valuable document had it not tried to apply its findings to residential care in general. “Children suffer routine harm inside RTF’s,” the authors write. “These harms include sexual, physical, and emotional abuse, unsafe and unsanitary conditions, and inadequate provision of behavioral health treatment.” Leaving aside the ambiguity of the word “routine” (does that mean every resident or the majority of residents are harmed in such a way?), such a conclusion cannot be drawn from an investigation of treatment centers operated by four large companies. We have no idea what proportion of young people receiving publicly funded RTF care are in facilities operated by these four companies. Around the country, there are residential treatment facilities operated by many providers, including many freestanding facilities that are not part of large chains. Even within the companies reviewed, the report provides no data to document whether the problems exist only at certain facilities or throughout the chains. A facility’s functioning to a large extent reflects its leadership, and there may be well-run facilities among those operated by these companies.
Going even further, the SFC concludes that “the risk of harm to children in RTF’s is endemic to the operating model. The harms children in RTFs experienced are the direct, causal result of an operating model that incentivizes providers to optimize revenues and operating and profit margin. RTF providers offer minimal therapeutic treatment in deficient physical settings with lean staff composed of non-professionals, which maximizes per diem margins…” The report goes on to say that “[a]t its core, the RTF model typically optimizes profit over the wellbeing and safety of children.” But there is no “RTF operating model.” The understaffing and lack of professionals that are common among publicly funded residential providers more likely stem from the low reimbursement rates that that these programs receive, which in turn means that staff receive low pay as well, forcing the facilities to rely on poorly educated and trained staff.
Even more extremely, the report states that “In the best of circumstances, children at RTFs receive care from under-trained and overburdened staff, are given infrequent therapy, sometimes by non-professionals, and are exposed to unsanitary, unsafe, and non-homelike environments.” It is hard to understand how the SFC is capable of describing the best residential programs when its entire methodology consisted of seeking abuses in an extremely limited universe of residential programs.
In suggesting that residential treatment is a flawed model that should not exist, the SFC report ignores the important role of residential treatment facilities in the continuum of care for young people with mental illness. The Committee’s own invited witness, Elizabeth Manley of the University of Connecticut School of Social Work, testified about the need for these programs.
Residential treatment facilities have an important role in the provision of care for young people with complex behavioral health care needs when they have a clinical or behavioral health treatment need that cannot be met in a family and community setting due to the intensity of their treatment and supervision needs. In those instances, we need the care to be delivered in trauma-responsive environments that embrace parent and caregiver engagement throughout the treatment intervention and continually focus on best practice. These residential treatment facilities can have a significant benefit to the young person and their family.
The Child Welfare League (CWLA), in written testimony submitted to the SFC, added that residential services are “a small but important part of the full array of services” that must be available to meet children’s mental health needs.” CWLA went on to explain that there “are many providers and programs providing or striving to provide trauma-responsive, time-limited, effective residential care. They are informed by the emerging literature highlighting promising practices in residential interventions..” CWLA cited the Building Bridges Initiative, which is a national initiative working to identify and promote best practice and policy in residential interventions for youth. The initiative has produced a guide called Building Effective Short-Term Residential Interventions. According to this report, a new literature has developed in the last ten years or so which documents promising practices in residential intervention which are associated with positive benefits. These include “actively engaging youth and families, ensuring active school and community connection, and keeping residential intervention as short as possible.” The authors explain that “[c]utting-edge effective residential intervention now means providers are creatively working with youth and families in the home, in the community, and as briefly as possible – often for three months or less.” The guide was developed to help organizations make the transition to the new approach, with case histories of 12 programs that are making or have made this transition.
Ignoring this new literature, the SFC claims that “studies show that home and community-based approaches produce better treatment outcomes than placing children in RTFs, and are more cost-effective than RTF placements.” In the footnote to that sentence, the writers list only one study, which concerns only one type of facility, Psychiatric Residential Treatment Facilities, a particular model the provides the equivalent of in-patient psychiatric services outside a hospital setting to young people under 21 through an agreement with a State Medicaid agency. Moreover, that study does not conclude that community-based approaches produce better treatment programs. Instead, it concludes that “evidence is insufficient to assess which interventions are effective.” It is almost impossible to conduct a meaningful study comparing residential treatment to community-based approaches, since the children who are sent to RTF’s are generally much more troubled or impaired than the children who are not, and it would be hard to control for such differences without doing a randomized controlled trial. That’s why there are few if any studies that shed light on this issue.
It is hard to avoid the conclusion that both the study design and the findings of the SFC reflect the Committee’s desire to show that residential care is harmful to young people. The SFC’s anti-residential bias is displayed in numerous passages throughout the report. One particularly inaccurate statement claims that “In some cases….., child welfare agencies place children in state custody without diagnoses in RTFs because they have nowhere else to place them.” As evidence, the report cites a 2013 report that showed 28.8 percent of children in “congregate care” had no clinical diagnoses. But congregate care (a term used to designate any placement that is not a foster home) is a more general term than RTF’s. The earlier report included many other types of facilities including cottage-style homes (often on the site of former orphanages and often providing high-quality family-style care) that are not intended for children with serious behavioral health needs, as well as emergency shelters that some states operate to house children before they are placed in a foster home. Given the relatively high cost of RTF’s, it would be very strange if states placed children in them for lack of another option.
Much more common is the opposite scenario: agencies placing children in foster homes unprepared to care for them, resulting in placement instability, or even letting them sleep in hotels or offices, for lack of residential treatment facilities. Articles about this problem appear frequently, including a recent report from the Midwest Newsroom (a collaboration between NPR and Midwest member stations) on the insufficient capacity of residential care for girls in Missouri and Iowa. The article starts with the story of a young woman who was placed in a residential treatment program called Missouri Girls Town after a traumatic childhood, placement in foster care and a disrupted adoption by a parent who could not handle her rebellious adolescence. This young woman credits Missouri Girls Town with completely changing the trajectory of her life. Sadly, this nonprofit program, which relies on private donations to supplement what it gets from government agencies, was designed to accommodate up to 50 girls but can only take 12 because of “staffing and funding challenges.” Stories like this have been appearing from around the country for years. There is not enough residential treatment for the young people in foster care who need it. Facilities have been shutting down due to failure of state reimbursement rates to keep up with operating costs, as well as the increasing unpopularity of residential care among state officials and legislators.
Despite the major flaws in the SFC’s analysis, there is little to object to in its recommendations. It’s hard to argue against recommendations that Congress act to improve conditions in congregate care facilities, that the companies reviewed raise their standards, and that states invest in community-based services for children with behavioral health needs and improve oversight over RTF’s. The need to invest in community-based services is particularly important because it might enable some children to be helped before their problems become so severe that they need residential care. It might even prevent some placements in foster care that occur when parents can no longer care for behaviorally challenging their children at home. But the findings of the report remain dangerous even if the recommendations are benign; they can be used to support attempts to defund residential care entirely, which would be disastrous for our most vulnerable young people and their families.
The SFC report confounds a group of residential treatment facilities poorly run by four large corporations with the entire field of residential treatment for youth with serious behavioral health care needs. The report presents a distorted picture of a field that already contains excellent, life-changing programs and where passionate and dedicated leaders are already providing or working toward trauma-informed, short-term, and effective residential services for these most vulnerable young people.
Visits to five facilities that were not operated by the four providers being investigated were used to document physical conditions in the facilities, as well as their efforts to provide education to the residents. The finding of “non-homelike,” unsanitary and unsafe conditions was based on the visited facilities rather than on the four companies that were investigated. ↩︎
Year after year, states and the federal government continue to release annual data showing a decline in the number of children in foster care, congratulating themselves on keeping families together. They seem to have forgotten that reductions in foster care were supposed to be accompanied by increased services so that children could be safely maintained at home. Unfortunately, there seems to be little to no interest on the part of the federal Children’s Bureau, Members of Congress, advocates, or the media in whether such services are actually being provided.
The newest report from the Adoption and Foster Care Analysis and Reporting System (AFCARS) showed that the number of children in foster care dropped to 368,530 on September in 2022–a drop of 5.8 percent over the previous year 15.6 percent since 2018. “We are encouraged by the continued decrease in the number of children entering foster care and staying in foster care and we will continue working with our state, tribal and territorial partners to ensure an emphasis on family well-being and safe family reunification,” said Jeff Hild, the Principal Deputy Assistant Secretary of the Administration on Children and Families (ACF) in a press release heralding the new numbers. ACF gave credit to the Family First Prevention Services Act (FFPSA), which “helped change the conversation to be about prevention of foster care placements and preservation of families.”
It seems premature to celebrate the shrinkage of the foster care rolls as a triumph without knowing what is happening to the children remaining at home who would have been removed in a different year. How many of these children are living with abuse or neglect that will leave lasting scars or impair their development, if not endanger their lives? Supporters of the Family First Prevention Services Act (FFPSA), which passed in 2018, said that declining foster care counts would result from providing support to parents who needed help to address the problems (like substance abuse, mental illness and poor parenting skills) that led to their maltreatment of their children.
After an allegation of abuse or neglect is substantiated, an agency can place a child in foster care or open a case for in-home services, among other options.1 FFPSA made it possible to use the same federal funds for foster care and in-home services, allowing children to stay at home safely while their parents addressed the issues that put them at risk. A major purpose of FFPSA was to enable states to use federal funds that were formerly available only for foster care to pay for parenting support, mental health, and drug treatment that would enable children to stay safely with their families. The rationale for this change was that allowing foster care funds to be used for such services was necessary to enable states to keep kids out of foster care.
However, FFPSA has not made massive federal resources available for such services. ACF estimates that only 18,400 children in the entire country were served by Title IV-E prevention services programs in FY 2023, at a cost of $167 million. But perhaps states are using their own funds to pay for these services? After all, foster care is more expensive than services provided to families in their homes. Both require case management, but instead of the cost of room and board for foster youth, providing in-home services usually involve referring parents to mental health and drug treatment services often funded by Medicaid or paying for parenting support programs that cost less than foster care. (Of course the supporters of FFPSA ignored this basic fact and claimed the legislation would revolutionize child welfare!). States were already providing these services before FFPSA and they could have increased them without the promised federal funding.
But believe it or not, nobody knows if more children and their families are receiving in-home services as the foster care rolls decline, since the federal government doesn’t ask states for this information. While states were already required to report the number of children entering foster care, leaving it, and in care at a point in time, FFPSA did not add a requirement to provide the same data on services provided to children and families in their homes, now that they were also covered by federal Title IV-E funds.2 Hoping some states might track this data of their own accord, I searched the data publications and dashboards on the websites of the ten states with the largest number of children in foster care according to the most recent AFCARS report,3 but I was able to obtain this data for only California and Texas.
California has by far more children in foster care than any other state, 45,924 children at the end of September, 2022, which was 12.4 percent of the national total. Fortunately, there is extraordinarily good data from the California Child Welfare Indicators Project (CCWIP), a collaboration between University of California at Berkeley and the California Department of Social Services. The CCWIP dashboards include data on the number of entries into foster care and the opening of Family Maintenance cases, as in-home cases are called in California. Entries into foster care declined precipitously from April 2019 to March 2020 and continued declining, though more slowly, through March 2024. Family Maintenance case openings also declined continuously throughout the period. Thus, there was no increase in Family Maintenance case openings to compensate for the decline in removals. Or put in a different way, the total number of cases opened for child welfare services dropped from 46,264 at the beginning of the period to 29,969 at the end–a drop of 35 percent. Rather than a shift from foster care to in-home services, there has been a shrinkage of children reached by child welfare services overall.
Texas has the third largest state foster care caseload, after Florida. The Texas data are a bit more confusing. The number of children entering foster care dropped from 16,028 in 2021 to 9,623 in 2022, an incredible 40 percent, while the number of children entering in-home services declined steeply as well, resulting in a 35.7 percent drop in all case openings. Both drops may well have been related to a new Texas law that took effect on September 1, 2021 and changed the definition of neglect to an action or lack of action that puts a child in “immediate danger” of harm, rather than “substantial risk” of harm as the previous language read. The bill also put restrictions on child removals, requiring that children can be removed only from parents who display “blatant disregard” for their actions, or whose inaction “results in harm to the child or creates an immediate danger to the child’s physical health or safety.” Interestingly, in 2022, foster care entries actually rose slightly in Texas, while family preservation entries sprung back to where they were in FY2021, resulting a substantial increase in total case openings that year. Nevertheless, the overall trend over time was a decrease in foster care entries, family preservation case openings and the total number of children receiving help through open in-home or out-of home cases. That total dropped from 72,181 to 48,619 over five years–a drop of 32.6 percent–almost the same as the drop in California’s child welfare case openings.
Florida, the state with the second largest number of children in foster care, reports on the numbers of children entering foster care but not on the number entering in-home cases. One can, however, compare the number of children in foster care at a point in time with the number of children and young adults receiving in-home services. Both numbers have been decreasing and the number of children receiving in-home services has been consistently about half of the number of children in foster care. But these numbers don’t tell us whether declining entries to foster care have been offset by increasing entries to in-home services. In general, foster care cases last longer than in-home cases. Not knowing the average length of stays in foster care and in-home cases, and how they have changed over time, one cannot tell whether in-home case openings have made up for the reduced number of entries into foster care.
The Florida data show why point-in-time data cannot be used to answer the question of whether the decline in foster care entries has been accompanied by a rise in in-home case openings. Unfortunately, none of the other eight states with the highest caseloads provide this data on their websites. Illinois and Indiana provide point-in-time data on foster care and in-home participants. The other five states with the largest caseloads–Ohio, New York, Pennsylvania, Arizona, and North Carolina–display no data on in-home case participants at all.
If California and Texas are typical, states have not been increasing their provision of in-home services to make up for declines in foster care. Instead, the total number of abused and neglected children being helped by in-home or out-of-home services (or foster care) has declined by as much as a third in five years. But we cannot assume that California and Texas represent the entire nation. It is unfortunate that the writers of FFPSA did not requiring states to include data on in-home case openings and total caseloads, given that the legislation allowed federal funds to be used for this purpose. States have not begun tracking and reporting on this data on their own, and are triumphantly proclaiming the drop in foster care without even reporting on whether in-home services are being provided instead. When Congress considers desperately-needed fixes to FFPSA, a requirement that states report in-home case data analogous to the foster care data in the AFCARS system should be included in the new legislation.
Notes
Other options include referring a family to a community provider or even doing nothing nothing if the abuse or neglect was assumed to be a one-time event unlikely to occur. The family may also refuse in-home services, and the agency would then have to decide whether to file a court petition to require such services ↩︎
States must provide to National Child Abuse and Neglect Data System (NCANDS) information on how many children receive “postresponse services,” meaning services after a child protection investigation. But unfortunately, “postresponse services” includes foster care and provides a duplicated count, counting children every time they are the subject of an investigation, so it is not useful in telling us how many children receive in-home services. ↩︎
State foster care data can be accessed from https://www.acf.hhs.gov/cb/report/trends-foster-care-adoption. According to the latest information, the ten states with the largest number of children in foster care on September 30, 2022 were California, Florida, Texas, Illinois, Ohio, New York, Missouri, Pennsyhlvania, Arizona, and Indiana. ↩︎
Officials of New Jersey’s Department of Children and Families (DCF) are congratulating themselves on what they call the decline of child abuse and neglect in their state and attributing this ostensible decline to their department’s preventive services. The number of reports of child child maltreatment has actually increased over this period. DCF’s claims are based on a decline in the number of children with substantiated reports–a number which reflects DCF policy and practice much more than it reflects actual abuse and neglect. Whether agency officials are ignorant or attempting to manipulate the data for naive readers, this is no way to keep the public informed about how well New Jersey is protecting its children.
Two DCF officials, Laura Jamey, Director of the Division of Child Protection and Permanencyand Sanford Starr, Director of the Division of Family and Community Partnerships, say they have some good news for New Jerseyans. They announce it in an op-ed titled “Maltreatment of NJ kids is decreasing. Here’s wow [sic] we’re preventing it,” which was published in the Asbury Park Press. “By using evidenced-based [sic] prevention strategies and practically addressing families’ needs, we’re happy to report that over the past decade, there has been a steady decline in the number of confirmed cases of child abuse and neglect in our state. In 2016, there were more than 8,000 substantiated and established cases of Child Abuse and Neglect in New Jersey. Last year, that number was only 2,641.”
Wow! sounds impressive, right? But it turns out the authors took as much care with the substance of their commentary as with their capitalization and spelling. That much is clear to anyone who bothers to look at the data that New Jersey shares with the federal government through the National Child Abuse and Neglect Data System (NCANDS) and which the federal Children’s Bureau shares through its annual Child Maltreatment reports. The data for 2023 have not yet been published by the Bureau, but the figures below represent what New Jersey reported for Federal Fiscal Years (FFY) 2016 to 2022, which ended on September 30, 2022.
Federal Fiscal Year
Referrals
Children Receiving an Investigation or Alternative response
Children receiving a “substantiated” disposition/percent of referrals
Jamey and Starr cited only the number of substantiated cases of maltreatment. But that figure has meaning only in the context of two figures that represent earlier steps in the process, which are always discussed first in the Child Maltreatment reports. “Referrals” is the child welfare system’s term for reports to the state child protective services hotline. As you can see, those reports increased slightly in New Jersey from 56,014 in FFY2016 to 60,934 in FFY2019. There was a significant drop in referrals during the COVID pandemic in FFY2020 and FFY2021, and then a rebound to 57,068 in FFY 2022, just slightly higher than the number in 2016.
The number of children who were the subject of an investigation also dipped during COVID (in response to the drop in referrals) and bounced back up to a level that was slightly higher than that of 2016. But the number of cases that received a disposition of “substantiated” (which means an investigation concluded that a preponderance of the evidence indicated that abuse and neglect occurred) fell every year, with especially large drops in 2017 and during the COVID pandemic. And according to Jamey and Staff, that number fell even further to 2,641 in 2023, which means the number of children with substantiated referrals had dropped by 68 percent since FFY2016. And the number of children receiving a substantiated disposition as a percent of all referrals fell by half–from 11.2 percent to 5.5 percent, in that period.
So what explains this large drop in children with substantiated dispositions during a period of nine years? In its commentary in Child Maltreatment 2017 (CM2017), New Jersey attributed the one-year drop in children with substantiated dispositions from FFY 2016 to FFY2017 to a revised disposition model it adopted in April 2013.1 But after FFY2017, DCF provided no explanations other than regularly repeating its statement in 2018 that “the decrease in the number of substantiated victims “remains consistent with prior years and shows a continued trend in the decrease of victimization rates.” In CM2022, DCF simply acknowledged without explaining that “[d]espite the number of CPS referrals increasing from FFY 2021 to FFY 2022, the number of child victims continues to decrease. The rate in which New Jersey substantiated reports also decreased from FFY 2021 to FFY 2022.”
Research suggests that substantiation decisions are not very accurate and that a report to the hotline predicts future maltreatment reports and developmental outcomes almost as well as a substantiated report.2 So it just does not seem plausible that child maltreatment could have dropped by over half while the number of reports increased. There is one possible explanation for this decline, which I raised in a 2021 blog. New Jersey is one of many states that is increasingly using a practice called “kinship diversion.” Kinship diversion occurs when social workers determine that a child cannot remain safely with the parents or guardians. Instead of taking custody of a child, the agency facilitates placing the child with a relative or family friend. If this occurs in the context of an investigation, kinship diversion may result in a finding of “unsubstantiated” (or in New Jersey, “unfounded” or “not established”) even when abuse or neglect has occurred, on the grounds that the child is now safe with the relative. We have no idea how widespread kinship diversion is in New Jersey or how often it results in an “unfounded” or “not established” finding. However, the system of informal kinship care created by kinship diversion has been called America’s hidden foster care system and nationwide it appears to dwarf the provision of kinship care within the foster care system.
There is no way of knowing how much, if any, of the drop in child maltreatment substantiations is accounted for by kinship diversion. If diversion accounts for a substantial portion of the drop, that points to serious problems with the practice. It means not only that DCF is undercounting incidents of child abuse or neglect but also that a parent who committed serious maltreatment would not show up as having a substantiated report, possibly affecting decisions on future allegations against that parent. I described some of the other problems with kinship diversion, such as the lack of support for the child and relatives, the possibility that the caregiver will return the child to the an unsafe home, the possible placement of children with inadequately-vetted relatives, and the lack of due process and services for the parents, in another post.
Despite their lack of explanation in their annual commentaries designed for federal employees and child welfare specialists to read, DCF officials have offered the public an optimistic explanation for the drop in maltreatment substantiations. “We’ve worked to transform New Jersey’s child welfare system to support and strengthen families who are struggling to meet their basic needs rather than separating them. A family unable to provide clean clothes may need a supportive neighbor who can offer a ride to the local laundromat. A family struggling to put food on the table may need to be connected with a local food bank.” We have already shown that this decline does not indicate a decline in actual maltreatment, but this attempt to tie it to simple casework like finding a family a ride to a laundromat is simply not believable.
The problem is not just an op-ed that few will read. As quoted in NJ Spotlight News, the Commissioner of DCF told a legislative committee that “Working together, we have achieved so much for New Jersey’s families, including the lowest rate of family separations in the country, one of the lowest rates of child maltreatment and repeat maltreatment in the country.” This was quoted as part of a congratulatory article about how New Jersey has become a “national leader in child welfare.” it is unfortunate that this public media outlet simply echoed the Department’s rosy view, making no attempt to verify their claims by consulting the data.
The misuse of data by high officials of New Jersey’s child welfare agency raises an uncomfortable question. Is it really possible that these leaders believe that child maltreatment has declined by 68 percent since 2016? All I can say is that their statement reflects either ignorance or a cynical disregard for the truth. Neither of these options reflects well on the leadership’s moral or intellectual capacity to serve their state’s most vulnerable children and families.
Notes
Before the new framework, New Jersey had only two investigation dispositions: unfounded and substantiated. The new model added two new dispositions: established and not established, which fall on a continuum between “substantiated” and “unfounded.” DCF explains that the cases that receive the “established” disposition are coded as “substantiated” in NCANDS, so it is possible that finding some children who would have been substantiated as “not established” instead contributed to the drop in substantiations. ↩︎
Theodore Cross and Cecilia Casanueva, “Caseworker Judgments and Substantiation,” Child Maltreatment, 14, 1 (2009): 38-52; Desmond K. Runyan et al, “Describing Maltreatment: Do child protective services reports and research definitions agree?” Child Abuse and Neglect 29 (2005): 461-477; Brett Drake, “Unraveling ‘Unsubstantiated,’” Child Maltreatment, August 1996; and Amy M. Smith Slep and Richard E. Heyman, “Creating and Field-Testing Child Maltreatment Definitions: Improving the Reliability of Substantiation Determinations,” Child Maltreatment, 11, 3 (August 2006): 217-236. Brett Drake, Melissa Jonson-Reid, Ineke Wy and Silke Chung, “Substantiation and Recidivism,” Child Maltreatment 8,4 (2003): 248-260; Jon M. Hussey et al., “Defining maltreatment according to substantiation: Distinction without a difference?” Child Abuse and Neglect 29 (2005): 479-492; Patricia L. Kohl, Melissa Jonson-Reid, and Brett Drake, “Time to Leave Substantiation Behind: Findings from a National Probability Study,” Child Maltreatment, 14 (2009), 17-26; Jeffrey Leiter, Kristen A. Myers, and Matthew T. Zingraff, “Substantiated and unsubstantiated cases of child maltreatment: do their consequences differ?” Social Work Research 18 (1994): 67-82; and Diana J. English et al, “Causes and Consequences of the Substantiation Decision in Washington State Child Protective Services,” Children and Youth Services Review, 24, 11 (2002): 817-851. ↩︎
The annual Child Maltreatment reports, produced by the Children’s Bureau of the U.S. Administration for Children and Families, are based on data that states submit to the National Child Abuse and Neglect (NCANDS) data system. These reports are eagerly anticipated in the child welfare policy community because they provide much of the data commonly used to quantify child maltreatment and the operations of child protective services around the country. The latest report, Child Maltreatment 2022 (CM2022), provides data for Federal Fiscal Year (FFY) 2022, which ended on September 30, 2022. This post discusses the findings on child maltreatment fatalities specifically. A more general discussion of the report is provided in a previous post. In general, this analysis shows the extent to which child maltreatment fatality numbers and rates reported by states reflect how they define and determine child maltreatment fatalities. This diversity makes it impossible to use these data to estimate the total number of fatalities, differences between state maltreatment fatality rates, and differences over time. More specifically, several key points emerge from the analysis.
States reported a total of approximately 1,990 fatalities to the federal government for Federal Fiscal Year 2022. Yet it is widely recognized that states’ reports to the federal government greatly underestimate the number of child fatalities due to maltreatment by most common definitions. States may use restrictive definitions, fail to consult all available sources, or decide not to investigate or substantiate some maltreatment related deaths. Information from the states’ commentaries to Child Maltreatment 2022 reveals great diversity in how they determine child maltreatment fatalities. In states where child death review (CDR) teams estimate the number of maltreatment deaths, their estimates are always higher than the NCANDS estimates, with some CDR estimates as much as twice, three times, or even ten times higher.
CM2022 shows child fatalities increasing every year between FFY 2018 and FFY2022. But year-to-year changes should be approached with caution. Most states report for each fiscal year the number of maltreatment fatalities identified during that year, not the number that occurred during that year. However, at least two states, including the state with the largest number of children (California), report fatalities based on the year of occurrence and report additional deaths in subsequent years as they are identified. For this reason, even five-year trends shown in CM2022 may change over time. Adjusting for the changes in reports for these two states, reported child maltreatment fatalities have indeed been increasing since 2013. Several states report improvements over time in their ability to capture child maltreatment fatalities for NCANDS reporting. Thus, we do not know the extent to which this increase reflects improved reporting as opposed to increasing deaths from abuse or neglect.
The data reported in CM2022 show that child maltreatment fatalities are concentrated in the youngest children and become less frequent as age increases. Boys are somewhat more likely to die of maltreatment than girls. Black children are much more likely to die of maltreatment than White or Hispanic children—two to three times as likely as White children, depending on the year. The broad category of “neglect,” defined as defined as “neglect or deprivation of necessities” was involved in 76 percent of child maltreatment fatalities while abuse was Involved in 42 percent. Another 8.3 percent of child maltreatment fatalities involved medical neglect.
The Number of Child Fatalities
There is no standard mandated reporting system for child abuse or neglect deaths in this country. Definitions, investigative procedures, and reporting requirements vary from state to state. Attributing a child’s death to abuse rather than to an accident or natural cause is often extremely difficult. The death of a toddler who drowns in a bathtub, for example, may be classified as an accident in one jurisdiction or as a child neglect death in another.
Child Maltreatment 2022 (CM2022) reports an estimated total of 1,990 child maltreatment fatalities for FFY2022.1 But there is widespread agreement among experts that the annual estimates of child fatalities from NCANDS undercount the true number of deaths that are due to child maltreatment by a factor of two to three.2 The National Center on Child Fatality Review and Prevention lists several reasons why this occurs in a given jurisdiction. Jurisdictions may count only deaths substantiated as abuse or neglect using definitions from child welfare civil or criminal law, which may not be comprehensive. Some jurisdictions count only deaths for which the death certificate lists homicide or child maltreatment. Multiple data sources may not be used to identify possible maltreatment deaths. Accidental deaths that were made possible by egregious neglect are often not included,
To get states to use more data sources, the Child and Family Services Improvement and Innovation Act (P.L. 112-34) requires states to describe in their state plans all the sources used to compile information on child maltreatment deaths. To the extent that information from state vital statistics departments, child death review teams, law enforcement agencies and medical examiners or coroners is not included, states must explain the reason for the exclusion and how they plan to include this information in the future. However, this law is clearly not being enforced, and most states do not report using data from all these sources.
In the commentaries that almost all states provided with their NCANDS submissions (included at the end of CM2022), most report drawing on at least some sources external to the child welfare agency, but usually this information is accepted only as a report to the child protection hotline with an allegation of maltreatment. Only if investigated and substantiated by child protective services (CPS) are these deaths included in the counts provided to NCANDS. A few states report taking special measures to ensure that suspected child fatalities are reported to child welfare agencies. In Missouri, coroners and medical examiners are required by law to report all child fatalities to the child abuse hotline. In its commentary, Missouri suggests that it may appear to have a higher child fatality rate than other states because of this law, and indeed its child fatality rate is higher than that of most states. Indiana requires county coroners to report any “suspicious, unexpected, or unexplained” deaths to the Department of Child Services (DCS). Idaho’s Division of Vital Statistics refers to CPS all child death cases for which the cause of death is homicide. (Except when a link or reference Is provided, information in this post is drawn from CM2022.)
Some state child welfare agencies have an internal fatality review unit that may add maltreatment fatalities to the state’s counts. Minnesota’s child welfare agency has a Critical Incident Review Team that reviews death certificates and directs local agencies to add fatalities that they find were due to abuse and neglect to the cases that they already substantiated. New Jersey’s Department of Children and Families’ Office of Quality maintains a critical incident review process that may add to NCANDS some deaths that were not substantiated as maltreatment by CPS.
A few states explain that they report to NCANDS fatalities that are determined to be maltreatment-related by agencies other than child welfare:3
California reports fatalities determined by medical examiners or coroners, and by law enforcement agencies, in addition to county child welfare agencies, to NCANDS.
Washingtonand New Mexico report to NCANDS child fatalities that were determined to be the result of abuse or neglect by a medical examiner that were not already known to CPS.
Alabama, Nebraska, and North Dakota add cases from child fatality review teams that were not already in their databases to their NCANDS reports.
South Carolina incorporates into its NCANDS submission additional cases received from the State Law Enforcement Division (SLED), which receives reports of all child deaths that were not the result of natural causes. SLED investigates all “preventable” cases and refers its findings to the Department of Social Services.
Since most states’ child welfare agencies report only fatalities substantiated as maltreatment by CPS to NCANDS, the number that are reported will depend in part on the state’s definition of a child maltreatment fatality. NCANDS defines a child maltreatment death as “the death of a child as a result of abuse or neglect, because either: (a) an injury resulting from the abuse or neglect was the cause of death; or (b) abuse and/or neglect were contributing factors to the cause of death.”4 But not all states use this definition. At least one state, Arizona, includes only fatalities where abuse or neglect was the sole cause of death, as described in more detail below. (Iowa indicated that it did not include fatalities where child maltreatment was only a contributing factor until FFY2015 and there may be other states that do the same.)
A state’s maltreatment fatality numbers will also depend on its tendency to accept child fatality referrals for investigation and to substantiate them. Hotline screening methods and tools differ by state, and states report little about their screening practices around child maltreatment fatalities. Ohio, which has a county-run system, reports that some county agencies will not investigate child fatality reports if there are no other children in the home or the other children are not deemed to be at risk of maltreatment. The likelihood of substantiation of a report once accepted for investigation will depend on a state’s standard of proof and other investigation policies, messages transmitted by agency leadership, and staffing issues. My commentary about CM 2022 shows how much screening and substantiation rates for maltreatment reports differ by state, and there is no reason to think that fatality reports would be any different from other maltreatment reports. Variations in these rates, as well as the sources states draw from and the definitions they use, ensure that states’ child maltreatment fatality counts reflect much more than the actual number of maltreatment fatalities according to a given definition.
It is instructive to compare states’ maltreatment fatality rates displayed in CM2022 with their rankings on an index of child well-being such as the one used in the Annie E. Casey Foundation’s latest Kids Count Data Book. The 12 states with the highest rates of reported child maltreatment fatalities in CM2022 are Mississippi, South Dakota, Arkansas, Maryland, Alaska, Ohio, Missouri, New Mexico, North Carolina, Illinois, Indiana and South Carolina. Only four of these states are among the 12 states with the lowest rankings for overall child well-being, according to Kids Count. The 12 states with the lowest rankings on child maltreatment fatalities in CM2022 are Vermont, Montana, Nebraska, New Hampshire, Arizona, New Jersey, Rhode Island, Kansas, Kentucky, Utah, Maine, Utah and Hawaii. Five of these states are also among the 12 states with the best child well-being outcomes, and another seven are not. Clearly a state’s rank on child well-being is not an accurate predictor of its rank in reported child maltreatment fatalities. This suggests that the fatality data may reflect more than actual child maltreatment deaths that meet the state’s definition. Particularly striking are the two states—Arizona and Kentucky—that are among those with the lowest reported child maltreatment rates and worst child outcomes. But it is worth noting that there are no states with top-tier child well-being outcomes that have bottom-tier reported child maltreatment fatality rates. Therefore, this exercise suggests that the state fatality rates may reflect in part the “true” incidence of maltreatment fatalities as defined by the states and in part how maltreatment fatalities are identified.
Arizona is one of the states with the lowest reported maltreatment fatality rates despite its low child well-being ranking. Serendipitously, it turns out that Arizona has another estimate of child maltreatment fatalities, thanks to its exceptional Child Maltreatment Fatality Team (CFRT), which is housed in the state’s health department. Arizona’s CFRT analyzes every child death, classifies it by cause and manner, and determines whether the death was caused by abuse or neglect. All child death certificates issued in the state are reviewed, first by the local team in the area where the child lived, and then by the statewide team. For Calendar Year 2022, the team calculated that there were 146 neglect or abuse deaths, or 17 percent of all child fatalities that year. Yet, the Arizona Department of Child Safety (DCS) reported only 14 fatalities to NCANDS for FFY 2022, resulting in its low reported maltreatment fatality rate of 0.88 per 100,000 children.
In its current Child and Family Services Plan, DCS reported that it receives information on all unreported child fatalities from local CFRT’s. But the agency explained that CFRT identifies many more fatalities than it does because CFRT includes deaths where maltreatment was believed to have “contributed” to the death rather than “caused it,” a distinction discussed above, But, as we have seen, the NCANDS Codebook defines a maltreatment death to include cases where abuse and/or neglect were contributing factors to the cause of death.” By not reporting such deaths, DCFS is failing to report all maltreatment fatalities as defined by NCANDS.5
Arizona’s CFRT clearly has an expansive definition of maltreatment fatalities and probably errs on the side of finding maltreatment. Forty-four of the 146 maltreatment deaths it found (30 percent) were due to suffocation—apparently mainly unsafe sleep deaths. Another 15 (10 percent) were due to drowning. Most of these suffocation and drowning deaths were likely accidental. And as the quote at the top of this post indicates, one jurisdiction (or agency within a jurisdiction) may classify such a death as neglect and another may not. Another ten percent of the CFRT-identified maltreatment deaths were due to prematurity caused by the mother’s substance abuse or other factors. Fifteen states (including Arizona) and the District of Columbia defined prenatal exposure to harm due to the mother’s abuse of an illegal drug or other substance as neglect as of May 2022. But DCS may not in practice investigate or substantiate such cases.6
The comparison with CFRT provides some insight on why Arizona reports such a low rate of maltreatment fatalities. Leaving out fatalities where maltreatment was a contributing factor and being less likely to find that accidents or premature births involve maltreatment, may help explain the difference between the two estimates. It is also worth noting that Arizona reported a steep drop in maltreatment fatalities from 48 in FFY 2018 to 33 in FFY2019 to 18 in FFY 2020 (followed by no fatalities reported in FFY2021 and 14 in FFY2022). Arizona provided no explanation for these reductions in its commentaries for FFY’s 2019, 2020, and 2022 and did not provide commentary for FFY2021. One cannot help but wonder whether DCS changed its methods or criteria or simply stopped investigating some allegations of child maltreatment fatalities.
In its publication mentioned above, the National Center for Child Fatality Review and Prevention notes that child death review (CDR) teams often identify more maltreatment deaths than states report to NCANDS. Among the reasons are the records from multiple disciplines and agencies are shared, additional information comes to light in the review process, CDR leads to improved investigations, and teams often use broader definitions for maltreatment, as we have seen for Arizona. CDR teams in most states do not review all child fatalities for a given year or identify those that were due to maltreatment, as Arizona does. But a review of the most recent state CDR reports in all states that published statewide reports yielded eight state CDR teams (including Arizona’s) that do such an analysis. Table 1 shows the differences between the number of maltreatment fatalities identified and reported to NCANDS by child welfare agencies and the number identified by the CDR teams in these eight states in their most recent reports. All the CDR estimates are higher than the NCANDS reports, ranging from 50 percent higher in North Dakota to almost ten times as high in Arizona.
Table 1: Number of Child Maltreatment Fatalities Reported by NCANDS and by CDR
In contrast to Arizona, Mississippi’s position in the ranking of child maltreatment fatalities is not a surprise. Being 48th in child well-being, the state also has the highest child maltreatment fatality rate—by far—at 10.62 per 100,000 children. But there is an anomaly. Mississippi’s maltreatment fatality rate is almost twice that of the state with the next highest rate. And it almost doubled between 2020 and 2022. Even assuming that Mississippi’s “real” maltreatment fatality rate is closer to the 5.48 per 100,000 it reported in FFY2020 still puts it second from the top of all states. It seems unlikely that Mississippi’s child maltreatment deaths doubled in two years; it is more plausible that something about the way the deaths were defined, identified, or reported changed.
This discussion has illustrated the impossibility of knowing the extent to which state maltreatment fatality numbers reflect real differences in child maltreatment fatalities versus differences in definition or measurement. But if states were consistent over time in their definitions and measures, the difference in fatality numbers over time could still be meaningful. Whether that is the case is discussed below.
Have child fatalities increased?
As mentioned above, CM2022 provides a national estimate of 1,990 children who died of abuse or neglect in FFY 2022 at a rate of 2.73 per 100,000 children in the population. Exhibit 4A from CM2022 shows an increase in reported child maltreatment every year between FFY2018 and FFY2022.7
There are many reasons to be cautious about year-to-year comparisons of child fatalities. Those deaths reported in the 2022 report did not mainly occur in 2022. As CM2022 puts it, the “child fatality count in this report reflects the federal fiscal year (FFY) in which the deaths are determined as due to maltreatment,” rather than the year of death.8 It may take more than a year to find out about a fatality, gather the evidence (such as autopsy results and police investigations) to determine whether it was due to maltreatment, and then make the determination. States explain in their commentaries that the deaths they reported may have occurred as long as seven years before 2022. Because child fatalities are rare, a year-to-year increase, even in a larger state, may reflect a large fatality event that occurred in one year or a delay in determining several fatalities. For example, Illinois reported that an increase from 70 fatalities in FFY2018 to 106 in FFY 2019 resulted from the delayed completion of 15 death investigations and an incident that claimed the lives of ten children.
However, not all states report fatalities in the way described by CM2022. California, as it describes in its annual commentaries, reports for each federal fiscal year the deaths that occurred in the prior calendar year and were known to the state by December of the calendar year following the death. Because counties will continue to investigate fatalities that occurred in previous years, the state submits revised counts if additional fatalities from that calendar year are later determined to be caused by abuse or neglect. For example, California originally reported 135 fatalities in FFY2021, but that number had increased to 159 by FFY2022. Second-year changes were not as large for fatalities first reported in FFY2020 and FFY2021.
Knowing that at least one state changes its fatality data in the next year’s submission raises an intriguing question. Even accepting that each state’s fatality count has its own meaning, can we even rely on Exhibit 4A in any given year to at least illustrate the trend in reported fatalities? It does not take long to answer that question. Exhibit 4A of CM2021 does not show maltreatment fatality rates increasing each year between FFY2018 and FFY2022, as does the same table in FFY2022. Instead, it shows a decrease in FFY2020 followed by an increase in FFY2021 to just slightly below the level of FFY2019.
Since each CM report shows five years of data, each year’s figures will eventually be shown in five different reports, starting as the most recent year displayed and ending as the earliest year. Table 2 shows the numbers of fatalities reported for FFY 2018 to FFY2022 in the CM report for each year. The figures for FFY2018 and FFY2019 changed two or three times in the succeeding years, but never by more than 10 deaths. Oddly, the number of deaths reported sometimes decreased from year to year. But the original numbers for FFY2020 and FFY2021 increased considerably in succeeding years. The total number of deaths reported for FFY2020 increased from 1,750 in that year to 1770 in FFY2021 and 1,850 in FFY2022. The total for FFY2021 increased from 1820 in that year to 1930 in FFY2022. Clearly, the 24 fatalities that California added in FFY2022 for the previous year are part of that increase, and presumably one or more other states did the same. Inserting the new numbers into the table from CM 2021 now shows an increase every year between FFY2018 and FFY2021.
Table 2: Deaths Reported by Year Reported
Deaths in:
Reported In:
2018
2019
2020
2021
2022
2018
1770
1780
1770
1765
1765
2019
1840
1830
1825
1825
2020
1750
1770
1850
2021
1820
1930
2022
1990
Source: Author’s compilation from Children’s Bureau child maltreatment reports. US Department of Health and Human Services, Administration for Children and Families, Children’s Bureau, “Child Maltreatment,” June 27, 2023, https://www.acf.hhs.gov/cb/data-research/ child-maltreatment.
A plot of the number of child fatalities reported between FFY2013 and FFY2022, using the most recent versions of each number, is shown below as Figure 1. Assuming the numbers for years before FFY2021 will change little if at all, we can see that reported child maltreatment fatalities have increased annually since FFY2013, aside from a slight decrease in FFY2017. And if the numbers from FFY2021 and FFY2022 will increase, as seems likely, the rise in fatalities in FFY2021 and FFY2022 will get steeper.
Source: Source: Author’s calculations using US Department of Health and Human Services, Administration for Children and Families, Children’s Bureau, “Child Maltreatment,” June 27, 2023, https://www.acf.hhs.gov/cb/data-research/child-maltreatment
The critical question is whether this increase in reported child maltreatment fatalities reflects increasing maltreatment deaths, better measurement, or even changing definitions. Some states attribute increases in reported fatalities to improvements in the accuracy of their reporting.9
Through 2018, North Carolina reported only child fatalities determined by the Chief Medical Examiner as homicide by a parent or caregiver. According to a Senior Media Relations Manager at the North Carolina Department of Health and Human Services, “Since 2018, Child Welfare has: developed closer working relationships with counterparts at OCME, utilized vital statistics data, and enhanced processes to include more law enforcement information. This work has increased our ability to identify maltreatment deaths, as defined in statute…[W]e have also continued to enhance our ability to track the information – resulting in more robust reporting and accounts for the change in numbers.” The Children’s Bureau noted in CM2022 that North Carolina “resubmitted data from multiple prior years to include additional fatalities.” North Carolina’s reported child fatalities increased from 64 in FFY2018 to 111 in FFY2019, 99 in FFY 2020, 121 in FFY2021, and 93 in FFY2022.10
Mississippi reported that the creation of a special investigation unit for child fatalities in FFY 2014 resulted in an increase in reported child maltreatment fatalities in FFY2013, FFY2014, and FFY2015. The state also reported that public awareness campaigns about deaths caused by unsafe sleep and deaths from heat stroke of children left in hot cars led to more reporting of such deaths as possible maltreatment starting in 2014.
West Virginia reported 20 fatalities in FFY 2016 compared to 9 in FFY2015 and attributed the increase to the fact that the state had begun investigating child fatalities in cases where there were no other children in the home.
Virginia attributed its increase from 37 maltreatment fatalities in FFY2014 to 54 in FFY 2015 to a change in the law regarding the timing of investigations. The time spent waiting to obtain documents from outside agencies, like autopsies, would no longer count toward the 45-day deadline for completing an investigation. (It is not clear whether child death investigations previously were terminated before these documents arrived, and therefore the deaths were not reported.)
Ohio reported in FFY2022 that it required mandated reporters participating on child fatality review boards to report suspected maltreatment fatalities to the local child welfare agency. Reported child maltreatment fatalities increased from 98 in FFY2021 to 115 in FFY 2022. But the state also attributed the fatality increase to the fact that the overall death rate from violence had been on the rise for the past several years, showing the difficulty of disentangling causes for any increase in maltreatment fatalities.
Iowa began reporting child fatalities where maltreatment was a contributing factor rather than the sole cause of the fatality in FFY 2015. Reported fatalities increased from 8 to 12 but those are small numbers, and Iowa attributes the increase to the growing under-18 population.
The increase in reported maltreatment fatalities clearly reflects at least in part improved reporting, as documented by some states. But it may also reflect an underlying increase in actual maltreatment fatalities as defined by the states. Such an increase could be due to several factors. Washington’s commentary in the FFY2022 report suggests that the opioid crisis has contributed to its increase in fatalities from 19 in FFY 2021 to 31 in FFY 2022.11 West Virginia also reported an increase in illegal drug use in its commentary to CM2016, probably referring to opioid abuse as well.12 Ohio mentioned increasing violence in recent years as a possible reason for the increase in reported child maltreatment fatalities.
Demographics, type of maltreatment, and perpetrators
We have already discussed the reasons that the child maltreatment fatality numbers may not be accurate, even given different definitions in different states. These problems affect our ability to draw conclusions about demographics and child maltreatment fatalities. If some of the definition and measurement issues affect different groups differently, it is possible that findings on demographics would be less meaningful.
The data presented in CM2022 shows that Infants under a year old are more than three times more likely to die of maltreatment than one-year-olds, and the fatality rate generally decreases with age. Younger children are more fragile, and there are many reasons to believe that the relationship between age and maltreatment fatality rates is correct, despite problems with the data. The age graph has a similar shape every year, with the percentage of child fatalities dropping as age increases.13 The percentage of victims who are under one year old varied between 22.8 percent and 25.3 percent between FFY2018 and FFY2022. There are bigger differences by year in the older age groups, where smaller numbers make the data less reliable.
Boys were between 57 percent and 60 percent of the fatalities in every year between FFY2018 and FFY2022. In contrast, victims of child maltreatment in general, are slightly more likely to be girls. It is hard to imagine a reason why data problems would affect boys and girls differently, so it is likely that boys are more likely than girls to die from maltreatment.
Reported child maltreatment fatality rates varied greatly by race and ethnicity, and the differences among the larger groups were fairly stable over the five years since FFY2018. Black children had by far the highest maltreatment fatality rate of all the groups for whom information was available. The fatality maltreatment rate for Black children ranged from 5.06 to 6.37 per 100,000 children over the five-year period. Reported maltreatment fatality rates ranged from 3.27 to 4.40 for children of two or more races. White children reportedly died from maltreatment at a rate between 1.90 and 2.18 per 100,000 children, Hispanic children at a rate from 1.44 to 1.89. (The numbers of Native American, Native Hawaiian, and Asian children were too small to be reliable). The reported maltreatment fatality rate for Black children was two to three times as high as the rate for White children, which was always somewhat higher than the rate for Hispanic children. The rates from CM2022 are shown in Exhibit 4-D, reproduced below.
The question of bias must be addressed in evaluating racial and ethnic differences in reported child fatality rates. We have seen that fatality numbers reported by states generally reflect the results of a CPS investigation or a determination by a coroner, medical examiner, or fatality review team. It is possible that racial bias could play a role in whether a fatality is substantiated as due to maltreatment. But Drake et al. found that indicators of risk and harm for Black children were usually between two and three times greater than those for White children in 2019, while the Black-White homicide disparity was four times as great as that for White children.14 While we cannot rule out any role for bias, it is unlikely to be the main cause of the Black-White disparities in child maltreatment fatalities. As Drake et al suggest, they are more likely to stem from the legacy of slavery, Jim Crow, and segregation, which includes intergenerational poverty and the relegation of poor Black families to disadvantaged and often dangerous neighborhoods.
For each fatality, NCANDS collects the types of maltreatment that were substantiated. The authors note that “while these maltreatment types likely contributed to the cause of death, NCANDS does not have a field for collecting the official cause of death.” One child can be found to have suffered more than one type of maltreatment. Over three quarters (76.4 percent) of the children who died were found to have suffered from “neglect” (defined as “neglect or deprivation of necessities” in the Codebook), 42.1 percent were found to have endured physical abuse, 8.3 percent were found to have suffered from medical neglect, and 2.4 percent from sexual abuse.
Most of the perpetrators of reported child maltreatment fatalities were parents, according to NCANDS data submitted by 43 states. A total of 81.8 percent of the maltreatment fatalities involved “one or more parents acting alone, together, or with other individuals. That includes mothers alone in 13.2 percent of the death, fathers alone in 14.5 percent, “two parents of known sex” in 23.2 percent of the fatalities, and mothers with nonparents (such as boyfriends) in 10.3 percent of the cases. Another 13.2 percent of the fatalities involved nonparents only, including relatives (4.7 percent), “child daycare providers” (1.3 percent), unmarried partners of the parent (1.1 percent), and “other” (3.4 percent). A final 4.9 percent of the fatalities involved unknown perpetrators only. (See Table 4-4 of CM 2022 for all the categories, numbers and percentages).
CM 2022 was originally published on the Children’s Bureau website early in January 2024 without a press release; it then disappeared from the website for about three weeks. It is hard to avoid speculating about the reasons for its removal and the gap before it was finally replaced. One might wonder if officials were trying to figure out how to spin the five years of increase in reported fatalities. Strangely, the press release, when it did come out, reported the increase in child maltreatment fatalities without raising the possibility that changes in how fatalities were defined and measured could have contributed to this increase, which might have supported their optimistic narrative.
In summary, this analysis shows how difficult it is to make any conclusions based on the child maltreatment fatality data contained in the Children’s Bureau’s annual Child Maltreatment reports. Single-year numbers cannot be fairly compared between states because they reflect different ways of defining child maltreatment fatalities, learning of fatalities that may involve maltreatment, and determining whether maltreatment was a contributing factor. Trends over time are difficult to assess because states often change these definitions and practices, and because new data from previous years may be entered after each year’s report is published. There is evidence that improved reporting has contributed significantly to the increase in reported fatalities. But until the federal government imposes a uniform set of standards for counting child abuse and neglect fatalities as recommended by the Committee to Eliminate Child Abuse and Neglect Fatalities, it will be impossible to get a handle on actual levels and trends.
Notes
This estimate is based on the reports of 51 jurisdictions including the District of Columbia, Puerto Rico, and all states but Massachusetts. The maltreatment fatality rate for the reporting jurisdictions was multiplied by the population of all 50 states, the District of Columbia, and Puerto Rico, to obtain the estimate of 1,990.
US Government Accounting Office (2011). Child Maltreatment: Strengthening National Data on Child Fatalities Could Aid in Prevention. Washington, DC; Schnitzer P, Covington T, Wirtz J, Verhoek-Oftedahl W, Palusci V. (2007). Public Health Surveillance of Fatal Child Maltreatment: Analysis of 3 State Programs. American Journal of Public Health. 97:7; Herman-Giddens ME, Brown G, Verbiest S, et al. (199() Underascertainment of child abuse mortality in the United States. JAMA. 282:463–467; Crume TL, DiGuiseppi C, Byers T, Sirotnak AP, Garrett CJ. (2002). Underascertainment of child maltreatment fatalities by death certificates, 1990–1998. Pediatrics. 110(2 pt 1):18.
In contrast to those states that augment their own data with that of other agencies, Alaska delegates the entire process of determining whether a fatality involves maltreatment to medical examiners or coroners.
CAPTA defines maltreatment in part as “an act or failure to act on the part of a parent or caretaker,” but it does not define “caretaker.” There may be some differences among states on who they define as a caretaker, but these are unlikely to affect many cases and cause big differences between states.
DCS also says that CFRT’s fatality count is higher because it counts fatalities caused by a person other than the parent, caregiver, or custodian (which would not normally be counted). Based on CFRT’s tabulations regarding caregivers, this does not seem to be a large issue. DCS also state that the CFRT counts deaths that occur outside the state’s jurisdiction, such as on an Indian reservations. It is true that CFRT includes any death that occurs in Arizona, even if the child is not a state resident. However out-of-state residents were only three percent of the total number of fatalities in 2022, according to its most recent report, Ten percent of the children who died of all causes were American Indians but they do not report on how many lived on reservations.
The remaining deaths that CFRT identified were due to motor vehicle and other transport (14), poisoning (13), other medical causes (12), blunt force injury (10), undetermined (9) causes, firearm injury (8), and other injury (6). Many of these deaths could also be due to accidents that DCS was reluctant to investigate or find neglectful.
Exhibit 4A counts the District of Columbia and Puerto Rico as states, resulting in up to 52 “reporting states” per year.
Child Maltreatment 2022, p. 52.
Other states report improvements in their data collection, but their data do not suggest that they had a long-term beyond one year on fatality numbers. In FFY 2020, New York reported that it began reporting all fatalities, regardless of date of death, as long as the investigation ended during the reporting period and the fatality had not been reported during a prior year. Before that time, New York reported only those deaths that occurred and were reported in the applicable FFY. New York attributed the increase in the number of fatalities from 69 in FFY 2019 to 105 in FFY 2020 to this change. Perhaps the increase came from reporting an extra “batch” of fatalities in FFY2020. However, the state had reported 118 fatalities in 2018. And it then reported 126 in FFY2021 and 105 in FFY2022, so it is hard to understand how the change resulted in an increase in fatalities reported, except as compared to a year with abnormally few of them. When fatalities rose sharply in Mississippi from 49 in FFY2021 to 72 in FFY2022; the state again used the creation of the special unit in FFY 2014 to explain the increase, but that seems unlikely. I have asked West Virginia to speculate about reasons for the increase but have not yet heard from the state. In FYF2019 or perhaps FFY2018 (when the state did not submit commentary), South Carolina created a special unit to receive and investigate reports of child fatalities. The number of fatalities reported jumped from 39 in FFY2018 to 60 in FFY2019. But it then fell to 36 in FFY 2020, 41 in FFY2021, and 38 in FFY2022. So it is does not appear that the creation of the special unit had a long term effect on maltreatment fatality counts.
North Carolina provided revised numbers for FFY2018 and FFY2019 to NCANDS and provided them to me through their press office
Washington reports that between FFY 2021 and FFY 2022 the percentage of child fatalities in the state that were due to opioid ingestion or overdose rose from less than one percent to 23 percent of child fatalities. Of the deaths and near-fatalities that qualified for a review because they occurred in families touched by the system in the previous year, that percentage jumped from 28 to 44 percent.
In its Commentary, West Virginia stated that only one of the 13 fatalities reviewed by its critical incident team did not involve substance abuse as a factor either in the death or the family’s history.
However, it must be reported Exhibit 4-B, Child Fatalities by Age, appears to be inaccurate. It looks very different from every other year, with much higher rates for older children. There is no way that the fatality rate per 100,000 17 year olds would increase from 0.42 to 3.3, from 0.57 to 5.0, for example. It looks almost, but not exactly, like Exhibit 3-D, which shows child maltreatment victims (not deaths) by age. The Children’s Bureau referred my inquiry of March 21 to the “appropriate team,” which has not yet responded.
Brett Drake et al., “Racial/Ethnic Differences in Child Protective Services Reporting, Substantiation, and Placement, With Comparison to Non-CPS Risks and Outcomes: 2005-2019. Child Maltreatment 2023, Vol 0(0) 1-17.
ABC News: Joanna, Terri and Sierra Denton-Carrillo
On May 2, 2024, an extraordinary gathering was held in Washington, DC. It brought together scholars, advocates, and family members of children who lost their lives to abuse and neglect to mark the inauguration of a new project, Lives Cut Short. This project, under the auspices of the American Enterprise Institute and University of North Carolina Chapel Hill, will shed a light on the lives and deaths of abused and neglected children, many of which would never otherwise be known to the public. I am proud to be a part of this project, along with Naomi Schaefer-Riley AEI’s point person on child welfare, and eminent child welfare scholars, Emily Putnam-Hornstein of UNC-Chapel Hill and Sarah Font of Penn State. If you missed the event, you can watch it here.
We are grateful that family members of two children who died of abuse were able to join us for our launch. One of these special guests was the aunt of Joanna (age three), Terry (age two) and Sierra (age six months) Denton-Carrillo, who were drowned by their mother despite desperate efforts by their father to warn the Los Angeles Department of Child and Family Services (DCFS) and LAPD about her deteriorating mental state. Also in attendance was the aunt of Sophia Mason, who was physically and sexually abused and forced to live in a metal shed by her mother and mother’s boyfriend in the months before she died. Alameda County (California) DCFS social workers ignored repeated warnings from school staff and medical professionals and family members about Sophia’s injuries and the danger she was in.
About 1,900 children died of maltreatment in the United States in 2022, according to national statistics that are known to be greatly underestimated. All of these children of them were likely known to a family member who could have reported or intervened. At one time, the fact that a large number of children died of abuse or neglect was a big national issue. A national coalition worked to mobilize support for the funding of the Protect Our Kids Act of 2012, which authorized the Commission to Eliminate Child Abuse and Neglect Fatalities (CECANF) and charged it with developing a national strategy to reduce fatalities from child abuse and neglect. CECANF began work in 2014, holding public hearings around the country. In March 2016, after two years of work, it published Within Our Reach: A National Strategy to Eliminate Child Abuse and Negect Fatalities, a 167-page report with 110 recommendations. Eight years later, the report is forgotten, the recommendations disregarded, and mentioning the issue is considered gauche in ruling circles. An office founded to monitor the progress of this state and local efforts to monitor the CECANF recommendations produced a “First Progress Report” and appears to have been disbanded.
Child welfare leaders, legislators and advocates appear to have lost interest in child maltreatment fatalities. As Naomi Schaefer Riley put it at the project launch, she often hears that talking about child maltreatment deaths is “letting the tail wag the dog.” We can’t make policy based on rare events and small numbers, she is often told. Yet, as she stated, these numbers are not small at all. They far surpass the number of people killed in mass shootings, that get a lot more attention. Perhaps more importantly, if child maltreatment is an iceberg, the fatalities represent the part we cannot see. How many more children are suffering in silence?
The Lives Cut Short project has multiple goals. We seek to draw attention to this issue, knowing that public attention is necessary to build up support for reform. We hope to provide a context for media outlets, who often cover an incident in their area without any knowledge of the context. We will draw attention how differently states are defining, identifying, and reporting child maltreatment fatalities, and how this results in a final tally that is like adding apples to oranges, grapes and other fruit, but in any case is underestimated. Already posted on our website is a report that illustrates this diversity in great detail, showing how the numbers that states report to the federal government reflect their definitions and reporting practices as much or more than they reflect the actual rates of child maltreatment. Entitled A Jumble of Standards: How State and Federal Authorities Have Underestimated Child Maltreatment Fatalities, the report may be the only available resource that describes this diversity in state reporting in such detail. And as several speakers explained on May 2, this diversity creates a paradoxical situation in which states that are more transparent and conscientious about reporting child fatalities end up looking like they have higher fatality rates.
The core of Lives Cut Short is a database called CANDID, which consists of records of children who died of abuse or neglect since 2022 whose deaths that fit the federal definition of maltreatment fatalities–those that are caused by maltreatment or for which maltreatment was a contributing factor. All of the data come from publicly available sources, including media reports and official case summaries or reports from states. Right now, the website enables the user to sort the children by state and age. Clicking on each child’s name will allow the reader to access media and non-media sources of information about the circumstances under which the child died. A detailed state-by-state page provides links to each state’s statute governing disclosure of child fatality information as well as links to any child fatality notifications, case summaries, and case reviews, that each state provides.
We will continue both to add child fatalities and to broaden the information on each death. As our searches yield new media reports and state notifications and reviews, which often appear as much as two years after a child’s death, we will add them to our census of child deaths. We plan to seek out other sources, such as Medical Examiner reports, to learn about cases of which we are still unaware. To broaden the information on each case, we have already begun to enter detailed data about these deaths in a detailed database that will record demographic characteristics of the children and families, causes of death, perpetrator characteristics and risk factors, past involvement with CPS and other services, and systemic factors that may have prevented the discover of these children’s plight before it was too late. By bringing together media reports, official case summaries, and other sources such as wrongful death suits, we will be able to provide a richer description than any one source can provide. This information can then be analyzed to provide valuable information to help prevent such fatalities in the future.
We hope that Lives Cut Short will restart the conversation about how to prevent child maltreatment fatalities, and more broadly, redirect the conversation about how to prevent child maltreatment fatalities, which must start with an honest consideration of what serious child abuse or neglect means. Even more broadly, perhaps it will even change the conversation around child welfare services, bringing child safety and well-being back into focus, but also bringing in other systems and their responsibility to vulnerable children. These goals may be ambitious, but we cannot afford to fail.
I am honored to publish this essay from Christina Faucett. Christina has been a licensed foster parent in the state of Washington for six years and has adopted one child from the foster care system. Prior to becoming a foster parent, she was a CASA for three years. She is currently a member of the DCYF Parental Advisory Group and is passionate about fixing what is broken in our child welfare system to keep Washington kids safe. She lives in the Seattle area with her husband and daughter. You can follow her on X at @DCYFWAtch.
In 2023, the Washington State Department of Children, Youth, and Families (DCYF) completely rewrote their Caregiver Report to Court form. This form is the only voice foster parents have in the dependency process, since they are not parties to the case, and thus are not entitled to receive legal counsel, file motions, read pleadings, or speak in court unless called on by the judge. Given this, one might expect that changes to the caregiver report form would by preceded by extensive communication and feedback from caregivers as part of the editing process. This did not happen.
I first became aware of these changes in the fall of 2023 when I was provided the new form to submit in my foster child’s dependency case. I then reached out to connections I had in DCYF to ask how these changes had come about, and who had participated in the process of editing the form. After being stonewalled by DCYF employees, I submitted a Freedom of Information Act (FOIA) request, the results of which I finally received a couple of weeks ago.
My FOIA response revealed that the committee convened by DCYF to make the changes to the caregiver report to court included only one caregiver. However, it included three representatives of birth parents, including one former birth parent who had a child in foster care, a parent attorney and a social worker from the Office of Public Defense (which represents and provides assistance and advocacy for birth parents in dependency cases), along with other court and DCYF employees, and one CASA representative. At no point were caregivers informed of this committee’s existence, invited to participate on the committee, or asked to give feedback on the committee’s proposed changes.
The only foster parent representative on the committee works with Amara’s Family Connections Program, which encourages foster parents to maintain relationships with biological parents. Although this foster parent is a representative for what is called the “1624 Consultation Team” (named for the bill that created the group), which is a group of elected foster parent representatives who are supposed to raise the questions and concerns of foster parents in meetings with DCYF, no other 1624 representatives appear to have been informed of the pending changes. The Foster Parent Association of Washington also does not appear to have been informed of the pending changes. An August 2, 2023 post to their website states, “This seems to have been a sudden change and not everyone in the system is aware of it.”
Adding to the confusion, DCYF released two different Caregiver Report to Court forms, a long form and a short form. However, the forms have some completely different questions. For example, “Are you maintaining open and viable communication with the child’s biological parent?” is only included in the short form, not the long form. Even after an entire year of work on this by the committee, the reports still have numerous typos and errors. The new report was released with instructions that caregivers could submit it to the child’s CASA, not just their social worker, even though the CASA program in some counties did not want this responsibility and refused to submit the forms to the court on behalf of caregivers.
While not all of the changes to the caregiver report form are bad, a quick look makes it clear that DCYF is trying to limit input from foster parents to information that supports reunification, while simultaneously diminishing their opportunity to highlight their own relationship with the child (whom they may have raised for years, possibly from birth).
Some examples of changes:
A question soliciting caregivers’ thoughts on the Department’s case plan has been replaced with a question asking “Do you have any additional information that may help reunite the child or youth successfully with their biological family?”
A general question about how the child’s visits with parents are going has been replaced with, “What’s working well with family time? Explain.”
Other changes imply that caregivers have obligations they do not have. For example: “How have you included the parents of the child in the medical and dental appointments?” It is the social worker’s responsibility, not the caregiver’s, to inform parents of medical/dental appointments. The communication question mentioned above likewise implies that caregivers have an obligation to communicate directly with biological parents. Caregivers may have many legitimate reasons (including privacy and safety reasons) not to communicate directly with birth parents.
The old form had two questions about the child’s relationship with the caregiver and adjustment to living in the caregiver’s home. On the new long form these questions have been replaced with one question which is relegated to the bottom of the form under “additional information.” The short form doesn’t even ask caregivers about their relationship with the child living in their home; it only asks about the child’s behavior in the home. A question asking caregivers to “Describe child or youth’s interactions with positive adults (i.e., coaches, teachers, church, mentors, other relatives)” is given higher billing on the long form than the questions about their relationship with their primary caregiver.
DCYF has lost around 800 licensed foster homes since 2019, and since their six-month pause on issuing all new foster parent licenses from November 2022, to April 2023, the number of unfilled emergent placement needs has skyrocketed. If DCYF wants to achieve their goal of eliminating short-term stays for foster children and youth in offices and hotel rooms by December 2024, they need to start treating caregivers with the respect they deserve, not trying to further stifle their voices.
As readers digest the report that follows, the content may cause significant discomfort stemming from painful, lived personal experiences and perspectives shaped by social constructs made implicit through centuries of white supremacy and structural oppression. Readers are invited to practice self-care while navigating this content and to consider reading the findings with a group to engage in collective reflection.
Tyrone Howard et al, Beyond Blind Removal: Color Consciousness and Anti-Racism in Los Angeles County Child Welfare. UCLA Pritzker Center for Strengthening Children and Families, March 2024, page 5.
For several years, and accelerating after the murder of George Floyd, concerns about the overrepresentation of Black children in child welfare compared to their share of the population have been a leading factor behind proposals to reform child welfare services. One reform proposal–known as “blind removal”–seemed blessedly simple: just hide the race and ethnicity of a child being considered for placement in foster care, and racial differences in child removal will disappear. Los Angeles County was one of the jurisdictions that decided to pilot this new approach, and an evaluation of this pilot was released last month. On first reading, the evaluation looks like evidence that the pilot failed to reduce disproportional Black representation in child welfare. On second reading, the weaknesses of the study come into focus, and it appears to be proof of nothing. On third reading, it becomes clear that the poor quality of the evaluation reflects the evaluators’ and agency’s response to a legislative mandate to pilot a program that they no longer supported because it was “color-blind,” as they proceeded in their plans to develop the “color-conscious” programs they preferred. Apparent from the beginning was that neither the sponsor, nor the agency, nor the researchers stopped to examine the data on blind removals provided in a TED Talk, nor did they consider the basic assumptionbehind this approach.
On July 13, 2021, the Los Angeles Board of Supervisors passed a motion requiring the Los Angeles Department of Child and Family Services (DCFS) to pilot the blind removal concept. The sponsor, Supervisor Holly Mitchell, was influenced by the publicity around an experiment in New York State suggesting that the simple process of hiding racial details about children reported to CPS had been successful in erasing much of the racial disproportionality in foster care placements. A TED talk by Jessica Pryce, the scholar who “discovered” the use of this procedure in Nassau County New York, has been viewed 1.37 million times. In that talk, Pryce presented, to thunderous applause, her finding that after five years of implementing blind removal, the proportion of children entering foster care who were Black plummeted from 57 percent to 21 percent. A post entitled The power of wishful thinking: the case of race-blind removals in child welfare showed that the numbers cited by Pryce were simply wrong. The Black percentage of children who were removed fluctuated from year to year during and after the implementation of blind removals, ending up higher in FY2020 than it was before implementation of the program. But the supporters of blind removal did not seem to have much interest in anything that would cast doubt on this apparently simple fix for the stubborn fact of racial disproportionality in child welfare.
The blind removal pilot evaluation
This month, the Pritzker Center quietly released its report on the Los Angeles pilot, Beyond Blind Removal: Color Consciousness and Anti-Racism in Los Angeles County Child Welfare. The pilot ran from August 2022 to August 2023 in two county offices, West Los Angeles and Compton-Carson. The blind removal process began after the office had investigated an allegation of maltreatment and determined that the removal of a child or children was the only safe alternative. The case was then referred to a panel of administrators in West LA, and to one administrator outside the supervisory line in Compton-Carson. In both offices, the case reviewers were given case details that left out all information that could signal race or ethnicity, including name, race, ethnicity, zip code, income, and school district. Cases were not referred for blind removal when “exigent” circumstances were present, which means there was “reasonable cause to believe that the child was in imminent danger of serious bodily injury (which includes sexual abuse).” In West LA, a “Coach Developer” presented the case to a team of case reviewers with the investigative social worker and supervisor present, and the case reviewers voted at the end of the meeting on the decision to remove the child. The decision would then be conveyed to the social worker and supervisor. In Compton-Carson, the final decision was made in the blind removal meeting between the social worker, supervisor and case reviewer.
To assess the results of the pilot, the researchers used three separate administrative datasets from the Department of Children and Family Services (DCFS) for hotline referrals, petitions filed, and cases that went through the blind removals process. The referral and removal datasets covered five years and three months from April 1, 2018 to June 30, 2023. The blind removal datasets covered the pilot period, from August 1, 2022 to July 31, 2023 in West LA, and September 1, 2022 to August 31, 2023 for Compton-Carson. It is strange and unfortunate that the referral and removal datasets did not cover the last month of the pilot in West LA and the last two months in Compton-Carson; we will see below that this omission caused a serious problem. For referrals and removals, the evaluators calculated a “Disproportionality Index” (DI), which depicts racial overrepresentation when greater than one, equal representation at one, and underrepresentation when less than one.
The researchers found that the total number of children who were removed from their families by each office trended downward during the study period but “racial disproportionality persisted with Black children overrepresented in removals in both offices and Latinx children overrepresented in the West LA office in most quarters.” They found very few non-exigent cases identified for removal in West LA went through the blind removal process. The office petitioned for the removal of 46 children over the period, of whom less than half (21 out of 46) received a blind removal review. The reasons these children were not referred for blind removal were not documented. The researchers report that the pilot was implemented with more fidelity in Compton-Carson, but they reported the results using different categories than they used for West LA, which made it hard to understand or compare the results of the two offices.*
Responses to a survey of workers and administrators provided little evidence of positive change. Social workers and supervisors largely perceived no change in how much they talked about race and ethnicity, the amount of support they received for talking about race and ethnicity and “managing their racial and ethnic biases in their work.” In addition, social workers and supervisors “mostly perceived no changes in how they conducted their daily work.” However, the researchers took pains to share the comments of the minority of employees that expressed positive views, reporting that “[s]ome interviewees came to understand that racial biases and stereotypes might unconsciously affect how decisions are made in the child welfare system.” And a fifth of social workers and supervisors “perceived greater engagement and support across key aspects of their work as defined in the Core Practice Model.”
But majorities of the staff interviewed expressed negative views about changes brought about by the pilot. Most important was the perception that the pilot worked against the prevailing approach of addressing disproportionality through race-conscious policies. As the authors put it, the blind removal pilot “was perceived as contradicting concerted efforts to address racial disproportionality in child removals by explicitly talking about race and increasingly building bridges with individuals and organizations in Black communities to support Black families.” The increased workload for administrative staff was a negative outcome, mentioned as a “source of frustration” by the authors.
A sloppy, poorly-planned and badly-documented study
While it would not be surprising if the pilot was not the cure that its sponsors hoped for, the sloppy research design and presentation make it difficult to accept the results as proof of the failure or success of blind removal in achieving its goal in reducing disproportional removals of Black children. The lack of a comparison site was a big problem. One cannot compare trends over time and assume that nothing changed other than the pilot. The two pilot sites chosen were far from ideal. The West LA office has both a small caseload and a very small proportion of Black children in the population served–only 5.9 percent. The authors report that there were only 46 children removed during the entire pilot, only 21 of whom went through the blind removal process. The total number of Black children removed per quarter, as shown in Figure 4 below, ranged from 0 to what looks like six. Compton-Carson had three times as many cases as West LA. However, 81 percent of the service area population was Latino, and only 17 percent was Black. In the Compton-Carson office, the number of Black children removed was five or less in the last four quarters and the bulk of the children removed were Hispanic. The researchers also assessed Hispanic disproportionality, but it was almost nonexistent at Compton-Carson. Almost all of their discussion of disproportionality relates to Black children, so one might expect them to choose two districts with enough Black children to provide meaningful numbers of removals.
Source: Beyond Blind Removal, page 31.
Even more problematic is the way the data were grouped for display and analysis, as shown in Figures 4 for West LA and Figures 9 and 10 for Compton-Carson. The researchers pooled their data for each calendar quarter despite the fact that in both sites, the pilot started and ended in the middle of a quarter. To make matters worse, data for the final month of the West LA pilot and the final two months of the Compton-Carson pilot are not provided because data were not available for the remaining one or two months–as mentioned above. So the reader cannot see the actual numbers of removals for the pilot period at either site; in only two of the four quarters shown was the plot was operational throughout the quarter.
The confounding of the effects of different interventions is another problem with the study design. This one cannot be blamed on the researchers, who warned that it would be a problem, as discussed below. Figure 9 shows that there was a decrease in the proportion of Black children removed in Compton-Carson starting in the second quarter of 2022, and a concurrent increase in the number of Hispanic children who were removed. This trend began before the blind removal pilot started but after the commencement of 4DX, another initiative to reduce disproportionality that was implemented in January 2021. Figure 10 shows the consequent decline in the Black DR, which falls below one in the first half of 2023, meaning that Black children were underrepresented in that period. The researchers conclude that the “decline cannot be attributed to 4DX because the intervention was not evaluated, nor can it be attributed to blind removal because this intervention was confounded by 4DX and other interventions meant to serve Black families more effectively, such as the Eliminating Racial Disparities and Disproportionality (ERDD) roundtables, and interventions designed to improve assessment of safety versus risk.”**
Additional Note: “4DX refers to the “Four Disciplines of Education,” a “leadership and goal-setting concept” implemented in some counties with the goal of reducing disproportionality by 10 percent.
Missing information is also a problem. It would be impossible to assess the effect of the blind removal process without knowing how often the panel or individual reviewing the cases reversed the decision to remove a child, and whether there was any pattern in terms of race and ethnicity. The authors report that of the 21 children who were referred for blind removal in West LA, the panel agreed with the decision to remove all but two of the children. DCFS reported that those children had situations that “stabilized” presumably between the initial removal decision and the meeting, but the numbers are too small to make any general conclusions. In any case, there wre few reversals of the initial decision, and it appears that these reversals did not relate to race but to changes in the child’s situation. In Compton-Carson, the researchers did not even report on how often the initial removal decision was reversed in the blind removal meeting.
It is also odd that the authors devoted so much of their analysis to topics and periods outside of the one-year blind removal pilots. Much of the text and graphics is devoted to analysis of referrals (not addressed by the pilot), and they usually refer to the entire five-and-a-quarter-year period with little mention of what happened during the pilot. Much of the analysis simply documents the disproportionality in referrals and foster care placements throughout the period–something that really does not need more documentation and was not the reason for funding the pilot. Concentrating on the full period also allowed the writers to disregard the effect of the pilot. In the most flagrant example, the authors state that “Further, while overall child removals decreased in the Compton-Carson office, Black children were disproportionately represented in removals by the office during most quarters for which data were analyzed with a very slight upward trend collectively.” Clearly, the quarters during which the pilot was implemented show a downward trend. The authors are probably right that this proves nothing about blind removals, but this presentation gives the impression that they wanted to avoid saying anything that could be quoted by those wanting to demonstrate the pilot’s success.
A pilot that was doomed to fail?
The report’s section on “Timeline and Related Events” provides clues to the origins of the problems with the pilot’s design. In the wake of George Floyd’s murder and the subsequent demonstrations, the authors report that “child welfare systems and their stakeholders began having deeper and more honest conversations about addressing the longstanding connections between racism and the child welfare system.” It was in that context that the Pritzker Center invited Jessica Pryce to present a three-part series on how to eliminate bias in the child welfare system, which included a discussion of blind removal. The following September, DCFS Director Bobby Cagle expressed interest in developing a blind removals pilot, and DCFS and the Pritzker Center worked to develop a pilot and evaluation plan. But at the same time, Casey Family Programs notified the Center that DCFS also wanted to implement a the “Four Disciplines of Execution,” or 4DX, a framework bills itself as a “simple, repeatable formula for executing your most important priorities.” The Pritzker Center evaluators report that they warned against implementing both programs simultaneously in the same offices, as it would be impossible to identify the source of any change that occurred.
In February 2021, DCFS submitted a letter to the Doris Duke Foundation in support of a grant to the Pritzker Center to evaluate blind removal. But in March, 2021, DCFS withdrew its plan to pilot blind removal. Meanwhile, 4DX was implemented in regional offices throughout Los Angeles County with a goal of “safely reducing entries” into foster care for Black children by 10 percent. The Pritzker Center met with DCFS to discuss an evaluation of 4DX, but no plan was developed. Also in July 2021, the LA County Board of Supervisors passed the motion to pilot blind removal and designated the Pritzker Center as evaluator.
In October 2021, DCFS began meetings with the Pritzker Center to plan the blind removal pilot. It appears that they considered only sites that were in the supervisory district of Holly Mitchell, the Supervisor who had pressed for the pilot. The updates from DCFS to the Board of Supervisors shed more light on the site selection. Only one site was required in the motion that was passed by the Board of Supervisors. In its first update, dated September 13, 2021, Director Bobby Cagle proposed selecting just the West LA office, because it was apparently the only appropriate site that had not implemented 4DX. Cagle argued that it would be a mistake to pilot blind removal at one of the other sites because the “core of the 4DX work is rooted in authentically seeing and addressing families through a cultural lens.” Shifting to a methodology that negates this approach, Cagle argued, would be “contradictory to helping staff make the adaptive change toward leaning into a family’s natural strengths, focusing on natural supports, and activating community partners as resources to mitigate Black/African American children from entering care.” But in the second progress report, dated May 2, 2022, Compton-Carson was listed as a second pilot site with no explanation. And in the third progress report, dated August 1, 2022, the new DCFS Director, Brandon Nichols, explained that Compton-Carson was added because it had already implemented 4DX, unlike the other sites that were still in the implementation phase.
It is understandable that a second site was added, as the numbers in West LA are so small, even though Cagle inexplicably reported to the the Supervisors that the two offices “have the additional benefit of serving a large enough population of Black/African American children to allow for sufficient sample sizes during the pilot phase.” We can now understand the lack of a comparison site, since it appears that no sites were available within the supervisory district that had not implemented 4DX or other interventions, and the small number of available sites may not have included one that was comparable to West LA. But it is clear that not only did the implementation of 4DX possibly contaminate the results of the pilot, but the various programs got into each other’s way in Compton-Carson. That office implemented not only blind removals and 4DX but also another program called Eliminating Racial Disparities and Disproportionality (ERDD), which provided “roundtables, cultural brokers, and father involvement.” The authors of the study report that because of the blind removal process, Black children could not be referred to ERDD until they had been removed, while it was normally used to prevent removals.
Reading between the lines, it appears that DCFS and the Pritzker Center were saddled with the blind removal pilot at a time when they had already lost interest in that program. Both the Center in its evaluation and Cagle in his updates made clear that they saw a conflict between the idea of blind removals and the color-conscious vision behind the other approaches they were implementing, and they both favored the latter. The Pritzker authors wrote, “Colorblind approaches are widely considered harmful to Black people and people of color because they seek to negate race and all the experiences that come with being a racial minority in this country.”
The Pritzker Center also had methodological reasons to avoid blind removals: they had already warned about the problems of evaluating any program when another program is implemented at the same time. Even though the 4DX implementation was complete, one might assume that lasting effects would be expected–and hoped for. It does not appear that anyone had looked closely at Pryce’s data; Cagle was still saying on August 1, 2022, that “[g]iven the successful research findings from New York’s study, …DCFS is excited about piloting Blind Removals in the hopes of achieving similar outcomes…”
To add insult to injury, the county was forced to pay for its no-longer-wanted blind removals pilot. In a classic example of an unfunded mandate, the Board of Supervisors directed DCFS to find $150,000 to fund the blind removals pilot, a directive with which DCFS duly complied. And the Pritzker Center had no choice but to accept the funds that DCFS was directed to provide. Despite their clear negative feelings, the authors tried to justify their work on blind removal, arguing post facto that “the blind removal pilot was viewed as an opportunity to assess the attitudes and perspectives of DCFS staff and social workers toward race, racism and racial bias. Thus, whereas the strategy itself involved a color-blind protocol, the day-to-day experience of blind removal involved significant and insightful discussion about the role of race in child removal.” But it seems unlikely that the pilot was viewed beforehand as an opportunity to assess staff attitudes. And the “insightful discussions” are hard to reconcile with the survey results showing no change in how most workers did their jobs or talked about race and ethnicity.
In the end, the authors tried to reconcile their original goal with the final product by saying the report “articulates a vision that thoroughly documents the pilot, but necessarily urges readers and stakeholders to imagine a color-conscious future for Black families that goes well beyond blind removal.” Bizarrely, though, they insisted that for some jurisdictions, “blind removal may be a worthwhile effort given the possibilities it holds when implemented with proper support and the insights it can afford concerning race and racism within the agency.”
Blinded by ideology
In addition to the difficulties caused by the adoption of multiple interventions at the same time, the blind removal evaluation was flawed from the beginning by the failure to question basic assumptions behind the concept. In their explanation of the idea, the report authors state that “It is hypothesized that racial disproportionality will be reduced because the investigative team’s implicit biases will be mitigated by the case reviewers’ input on the case’s merits for removal.” The missing piece is the assumption that such implicit biases are a major cause of disproportionate removals of Black children. The agency and the evaluators completely ignored the research that suggests that the bias (if any) is probably in the other direction. Most recently, a paper by Brett Drake and a star-studded group of researchers*** shows that once reported to CPS, Black children were slightly more likely to have been substantiated as victims of neglect and placed in foster care than White children until 2011 and somewhat less likely to be substantiated or placed thereafter. In the last few years before the Covid-19 pandemic, they calculated that Black children were about 80 percent as likely to be substantiated and placed as white children, whether or not demographic factors were held constant. Perhaps the increasing concern about disproportionate removals of Black children has been causing social workers and supervisors to be biased in the opposite direction.
Even if the evaluators did not learn from prior research, they could have tried to assess whether investigator bias was actually a cause of disproportionate removal of Black children. They could have collected data at both sites about the proportion of decisions that were overturned by the reviewers, the reason for these reversals, and whether being blind to race had any impact at all. Perhaps they would have learned something about what happens when race and ethnicity are hidden, or perhaps they would have found that hiding these characteristics is impossible. But the authors of the evaluation were apparently too blinded by ideology to even consider the possibility that past rather than current racism is behind current disproportionalities in child welfare. Of course it is not just the researchers, but also the leadership of DCFS, that labored under the assumption that the biases of social workers determine the disproportionality in child removals.
The assumption that disproportional representation in child removals reflects racism in the child welfare system does more damage than simply leading to the adoption of ineffective programs. If the assumption is wrong, as the research suggests, then Black children’s overrepresentation in reporting, substantiations, and removals reflects their real need for protection. And if a child welfare system finds a method that is actually effective in reducing Black children’s representation in child welfare systems, then we are effectively lowering our standards for safely parenting Black children. And that is obviously fine with the authors, who made no bones about their feeling that concerns about child safety unnecessarily interfered with implementation of the pilot. As they wrote:
In general, the West LA staff strongly believed that the slightest concern about safety trumped involvement in the pilot. Though well intentioned, these safety concerns may be informed by bias and thus impede the widespread application of blind removal to families in the West LA office. Across child welfare systems, safety concerns are often prioritized over diverting families from system involvement.
Beyond Blind Removal, page 27.
It is obvious that the authors believe child safety should take a back seat to diverting Black families from child welfare involvement. And there is reason to fear that this happened in Compton-Carson, where removals of Black children fell sharply between Quarter 2 of 2022 and and the same quarter of 2023. Perhaps the LA County has found an intervention that is effective in reducing the removals of Black children absolutely and relative to other groups. Cagle reported that 4DX produced a 47 percent decrease in Black children removed within seven months. That is a pretty radical change–a change that may have severe costs to Black children.
The blind removal report tells a strange and complicated story. It is the story of a pilot program that was apparently imposed by a politicians on a child welfare agency and an evaluator that had moved beyond that program in search of more color-conscious approaches. It is a story of an agency that adopted these preferred approaches simultaneously with blind removal, making it impossible to evaluate any of the interventions. It is the story of researchers and an agency who never stopped to examine the data on blind removals provided in a TED Talk, and who never stopped to think about the assumptionsbehind this approach. It is the story of an attempt to make it appear that this pilot was anything other than a waste of time and money.
Many thanks to Brett Drake, who made me aware of this report and who shared his thoughts about it.
Notes
*They report that Compton-Carson had higher fidelity to the model because more children’s cases (195) were referred to blind removal than the number of children for whom court petitions were filed (146). But this is confusing compared to the description for West LA, which speaks of the proportion of petitioned children who were subject to blind removal. When I requested clarification from the researchers, they simply restated the language from the report.
**In his first update to the Board of Supervisors, Cagle reported that the offices participating in 4DX had experienced a 47 percent reduction in Black children removed between January and August of 2021. The Compton-Carson data shown above documents part of that drop in the Compton-Carson office.
***Brett Drake et al., “Racial/Ethnic Differences in Child Protective Services Reporting, Substantiation, and Placement, With Comparison to Non-CPS Risks and Outcomes: 2005-2019. Child Maltreatment 2023, Vol 0(0) 1-17.
Greetings to my faithful readers! I’m trying out a different format for Child Welfare Monitor–a monthly newsletter format that highlights events and information that catch my eye. I’m not ruling out a single-issue piece now and then, particularly when there is a major new report or data source to discuss and analyze. Please let me know what you think of the new format. If you can think of a more exciting title than “Child Welfare Update,” let me know. And if you do find this to be a useful resource, please share it with your colleagues.
Adam Montgomery convicted of Harmony Montgomery’s death
In December 2021, Manchester, New Hampshire Police announced the disappearance of Harmony Montgomery, who would have been six years old if she were alive. We learned that Harmony’s noncustodial mother, Crystal Sorey, had called the police a month earlier to say that she had not seen or heard from her daughter since April 2019, two-and-a-half years earlier. The country was rapidly transfixed by the search for Harmony. We soon learned that the little girl, who was blind in one eye, had first been removed from Sorey at the age of two months by the Massachusetts Department of Children and Families (DCF) due to Sorey’s substance abuse. Harmony’s father, Adam Montgomery, was in jail at the time. Harmony was returned to her mother at seven months, and removed again at ten months. At almost three years old, and after two straight years in foster care with the same family that fostered her from the start and wanted to adopt her, Harmony was returned to her mother for the second time. At age three-and-a-half, Harmony was removed from her mother for the third time. Since Harmony was first removed, Adam Montgomery had been released from prison and begun visiting her. In February, 2018, a judge awarded Montgomery immediate custody of Harmony, without waiting for an assessment of his wife or a study of his living situation in New Hampshire.
A shattering report by the Massachusetts Child Advocate revealed the many missteps by all the professionals tasked with keeping Harmony safe. The OCA concluded that “Harmony’s individual needs, wellbeing, and safety were not prioritized or considered on an equal footing with the assertion of her parents’ rights to care for her in any aspect of the decision making by any state entity.”
Two years after the search for Harmony began, Adam Montgomery has been convicted of her death, thanks to the testimony of his wife. She told prosecutors that after Harmony soiled her bed at night he beat her viciously on the head in the morning of December 9, 2019 and again that afternoon in the car when she soiled herself once more. He then injected opioids and ate fast food as Harmony died of her injuries in the back of the car. He concealed Harmony’s body for months until renting a U-Haul and dumping her remains somewhere outside Boston. Her body has never been found. Montgomery is already serving 32 1/2 years in prison for another case and I hope he will never see the light of day, but what about all the professionals who failed to prioritize Harmony’s needs? And what has Massachusetts done to ensure that there will be no more Harmonies? The adoptive parents of Harmony’s brother have been speaking out; I assume Harmony’s foster parents are too devastated to do so, but their hearts must be broken.
Race trumps child welfare I: Black children don’t get attached?
Harmony Montgomery’s case illustrates, among other things, what happens when the importance of attachment for young children is disregarded. Attachment theory, which is widely accepted and taught in classes on psychology, social work and human development, posits that a strong attachment is central to the development of infants and affects their brain development and their ability to form relationships throughout life. The critical role of attachment in human development, which has been confirmed in mammals as well as humans, is the reason that the Adoption and Safe Families Act (ASFA) set a timeline requiring states to file for termination of parental rights after a child had spent 15 of the last 22 months in foster care. That is the deadline that Harmony’s team disregarded when they returned her to her mother after two years in foster care and continued to work with both parents after her return to foster care at the age of three-and-a-half. The continued disruptions were so devastating for Harmony that her foster parents, according to the OCA, could no longer meet her needs when she was placed with them for the third time, and asked that she be transferred to a specialized therapeutic home.
But some lawyers that counsel parents in child protection cases are being told that attachment theory does not apply to Black children. In Race Trumps Child Welfare, Naomi Schaefer Riley calls attention to a paper called “The Weaponization of Whiteness in Child Welfare,” originally published by the National Association of Counsel for Children. The paper calls attachment theory a “tool to justify the separation of families” and a manifestation of “racism in psychology.” The authors take aim at professionals who utilize attachment theory to argue for the adoption of Black children by White foster families who have raised them from infancy rather than returning them to their parents or placing them with kin. They argue that a Black child who has lived with a White foster family for the entire two-and-a-half years of his life should be placed with a relative who has never even seen the child. Black families, they say, belong to a collective culture, which emphasizes the needs of the group as a whole over the needs of an individual. Thus, any suffering to an individual child, they imply, is justified by the gain to the group–though it is hard to understand how Black people as a whole gain from the traumatization of young Black children.
Race Trumps Child Welfare II: ABA “addressing bias in medical mandated reporting” in Michigan
The American Bar Association (ABA) has announced that its Center for Children and the Law is piloting a new initiative in Michigan “to address overreporting by medical professionals of Black, Indigenous and Latino/a children to the child welfare system.” Without a footnote, the ABA reports that “injuries in Black children are 9 times more likely than those in White children to be reported as abuse despite evidence that child abuse and neglect occur at equal rates across races.” (Italics are mine.) Equal across races? I wonder what data they are using. While I am the first to acknowledge that maltreatment substantiation rates may not reflect actual incidence of abuse or neglect, evidence suggests that the two-to-one Blsck-White difference in child maltreatment substantiation rates is likely an understatement, not an overstatement. Moreover, Latino children nationwide are not reported to CPS disproportionately to their share of the population.
The pilots, funded by the Children’s Bureau, will use a “multisystem approach developed by the ABA’s Stop Overreporting Our People (STOP) project” to “address each decision made from the time a medical provider has a concern about maltreatment through child welfare hotline report and investigation to the decision of the judicial officer to remove the child from the home.” In Michigan, according to Child Maltreatment2022, of the 174,000 referrals to the hotline in Federal Fiscal Year 2022, about 68,000 were screened in, about 139,000 children received an investigation or alternative response (down 12 percent from the previous year), and 23,500 were substantiated as victims of abuse or neglect–a whopping 37.7 percent drop over the previous year. Of those “victims,” a total of 2,760 or 11 percent were placed in foster care–along with an additional 956 children who were not substantiated as victims but may have been siblings who were deemed to be equally endangered. Despite the precipitous drops in investigations and substantiations and the very low proportion of children substantiated as victims that were placed in foster care, the ABA isn’t satisfied…or doesn’t bother to look at data. The Michigan pilots will also focus on how doctors are trained to report maltreatment, according to the ABA. Discouraging doctors from reporting the signs that they are uniquely trained to spot may not strike all readers as a good idea.
Where was CPS?
Utah:Abuse in plain sight: Ruby Franke, a parenting influencer who achieved fame by promoting her strict parenting style, was sentenced to up to thirty years after pleading guilty to aggravated child abuse of two of her children. Franke rose to prominence with a youtube channel called 8 Passengers (now taken down) that documented her life with her husband and six children and was criticized for promoting abusive discipline methods. She eventually formed a business partnership with another woman named Jodi Hildebrandt, who encouraged and participated in the abuse of Franke’s children. Both women were arrested in August 2023, after one of Franke’s children escaped the home and ran to a neighbor’s house asking for food and water. The neighbor noticed the child’s open wounds, duct tape around his ankles and wrists and emaciation and called the police. After the arrest, the oldest daughter posted on social media that: “We’ve been trying to tell the police and CPS for years about this, and so glad they finally decided to step up.” “Several of us tried to help,” one neighbor told the Salt Lake Tribune. “I know people left food on doorsteps knowing the kids might not be eating; I know people were making phone calls to DCFS, to the police — people really did try and care. No one was looking the other way.”
New Mexico: $5.5 million settlement reached in eight-year-old girl’s brutal death: The Santa Fe New Mexicanreports that the New Mexico Children Youth and Families Department (CFYD) has agreed to pay $5.5 million to the brother and half-siblings of Samantha Rubino, acknowledging that it placed Samantha and her brother in the care of a man (Juan Lerma) with a history of child abuse and domestic violence, who had been investigated once before for abusing her and had not seen either Samantha or her brother for two years. Samantha died of blunt force trauma to the head, and Lerma placed her body in the trash. This is the latest in a series of big-money settlements by CYFD, funded by the taxpayers. New Mexico’s system is in crisis, with a backlog of 2,000 investigations of abuse and neglect. Is it too much to hope that the legislature will decide it is better to spend money up front to keep children safe than to pay massive settlements to their survivors?
The march continues to remove protections for homeschooled children
The powerful homeschool lobby continues its crusade to eliminate the few regulations that still exist to protect homeschooled children. In Nebraska, LB 1027 would eliminate two of the three minimal documents required for homeschool enrollments. It would bar school districts and Health and Human Services from investigating educational neglect in a homeschool setting. And it would give one parent the power to make homeschooling decisions without input from the other parent. The unicameral legislature’s Education Committee heard testimony from the Nebraska Christian Home Educators Association, the president of a Christian homeschoolers’ co-op, and another homeschooling parent. There was no testimony against the bill. The Education Committee has recommended the bill, and it is headed for a floor vote.
In West Virginia, legislators have tried to bar abusive parents from homeschooling ever since an eight-year-old girl named Raylee Browning died of sepsis, possibly caused by drinking toilet water, in 2018. Teachers had called CPS multiple times because Raylee was constantly hungry and covered in bruises. To avoid further problems, her guardians removed her from school for the ostensible purpose of homeschooling, thus enabling them to torture ber to death without interference. Every year since 2019, legislators have introduced Raylee’s Law, which would prohibit homeschooling if the parent or home educator had a pending investigation for child abuse or neglect or had been convicted of abuse, neglect or domestic violence. This very modest bill, which probably wouldn’t even have saved Raylee because her guardians did not have a pending investigation when they withdrew her from school, nor were they convicted of abuse, has never gotten through the legislature. This year it was voted down in the Education Committee by 15-5 after several legislators outlined their concerns–such as the fear that it would force children to enter public school before an investigation could be completed!
This year, the sponsors of Raylee’s Law managed to get a version of the legislation included in a bill that removes certain testing requirements for homeschooled children, and it passed by a voice vote. Unfortunately the amendment that passed was watered down further from the original bill, which itself was very weak The amendment that passed requires that a parent cannot withdraw a child for homeschooling if there is a pending child abuse or neglect investigation. But if the complaint is not substantiated within 14 days, the superintendent must authorize homeschooling. And the bill to which it was attached (HB 5180) reduces protection of homeschooled children by removing the requirement that parents submit academic assessments for homeschooled children in certain grades, as well as the requirement that the parent or home educator submit evidence that they have a high school or post-secondary degree.
Readers who care about the protection of homeschooled children and the drastic disproportion of power between homeschooling parents and advocates for their children should give to one of my favorite organizations, the Coalition for Responsible Home Education. They are doing their best on a shoestring budget, but they can’t afford to go to every state where protective legislation is threatened.
From the “Are you kidding me?” department
“Safe Haven laws” are a way for new parents who are not ready to raise a child to surrender their newborns safely without any questions or legal consequences. The laws exist in all 50 states. The Committee to Eliminate Child Abuse and Neglect Fatalities has endorsed these laws as a way to protect vulnerable infants and recommended that they be amended to extend the age of protected infants to age 1 and to expand the types of safe havens allowed. And it turns out that this option has existed in Europe since Pope Innocent III required churches to install “Foundling Wheels” in 1198!
In New Mexico, mothers are told they can anonymously surrender their infants through “safe haven baby boxes” located around the state. But recent media coverage from local stations KRQE and KOB4 has revealed the state’s Children Youth and Families Department (CYFD) has been investigating these surrenders–because they are required to do so by the state’s safe haven law. CYFD Secretary Teresa Casados told KRQE that “state law requires CYFD to investigate to ensure the mother was not forced to give up her baby, to make sure she is safe, and to inform the father of the child as well.” (She was apparently not asked what would happen if the father had raped or abused the mother.) She also explained that the Indian Child Welfare Act (ICWA) requires CYFD to look into each case and notify “all the tribes and pueblos” to ensure they are following the Act’s requirement that placement with a Native family be preferred. It is not clear that any other state has interpreted ICWA this way. New Mexico legislators rushed to draft legislation to retain the right of mothers to surrender their infants safely and anonymously, but the short session ended before a bill could be passed.
Never underestimate a persistent child advocate
John Hill, the Investigative Editor at Civil Beat, a nonprofit news outlet in Honolulu, Hawaii, has never given up on his quest to find out how a six-year-old girl named Ariel Sellers was placed with Lehua and Isaac Kalua, the adoptive parents who tortured her, culminating in her murder two-and-a-half years ago. The Kaluas have been charged with murder and abuse of both Ariel and her then 12-year-old sister, among other charges. The prosecution alleges that Ariel was kept in a dog cage and denied food, and that Lehua Kalua caused her death by duct-taping her mouth and nose. For more than two years, according to Hill, the Hawaii Department of Human Services has stonewalled in accounting for its actions in the adoption of Ariel, who was renamed “Isabella Kalua” by her adoptive parents. But Hawaii’s Public First Law Center, motivated by a series of columns written by Hill, has filed a motion to receive the foster and adoption records for Ariel and her siblings. Now Hill is asking uncomfortable questions about the January 2024 death of 10-year-old Geanna Bradley, who was also allegedly tortured and starved to death by her adoptive parents.
In a bizarre twist, the Honolulu Star Advertiser has reported that the Kaluas have retained custody over Isabella’s three sisters, who were removed from the home in September 2021. But apparently the state of Hawaii hasn’t moved to terminate the parental rights of the Kaluas. A special master appointed to oversee the interests of Ariel’s sisters is concerned that the failure to terminate the rights of the Kaluas will interfere with efforts to find permanent families and educational opportunities for the girls. (And already has, I would think!)
The guaranteed income craze continues
At its February oversight hearing, the Director of the District of Columbia Child and Family Services Agency announced a forthcoming grant from the Doris Duke Foundation to a guaranteed income for some low-income families. The announcement was greeted with congratulations from the Council Chair who referenced the great results from the recent Strong Families, Strong Futures pilot, which provided 132 new and expecting mothers with $10,800 in the course of a year. I don’t know where she got her information. An article in the Washington Post reported on interviews with three of the mothers participating in the pilot. One of the mothers took the money as a lump sum. Setting aside about $5,000 for essential expenses, she used the remaining money on a $6,000 trip to Miami preceded by the purchase of new clothes, shoes, gadgets and toys for all of her three children and a $180 hair and nails treatment for herself. Another mother decided to spend $525 on a birthday party for her one-year-old, who clearly couldn’t appreciate it. Program coordinators said that the mothers reported spending most of their funds on needs such as housing, food and transportation. But I’m not sure how I feel as a DC taxpayer to see my money spent in ways that I personally find wasteful, nor am I sure that allowing such spending provides appropriate training in how to budget scarce resources. Such no-strings-attached money giveaways might not be the best use of taxpayer money, even if foundations choose to support it.
And the prize for cynical use of data goes to….
Kentucky! The State’s Cabinet for Health and Family Services (CHFS) is crowing about Kentucky’s drop from the highest rate of child maltreatment “victimization” to number 13 among the 50 states and the District of Columbia. In a statement reported by Spectrum News1, CHFS said this improvement “demonstrates the efforts made by the Department for Community Based Services and its many partners to increase the provision of child welfare prevention services and reduce child abuse and neglect within the Commonwealth.” But child advocates and family court judges are not convinced, citing a longstanding problem with hotline workers screening out cases that should be investigated–exacerbated by the adoption of an actuarial screening tool at the hotline in April 2022. The report quotes two family court judges and a CASA program director who linked child deaths to the failure to investigate prior reports involving the same families. According to one judge, “The alarm has to be sounded because I’m not joking when I say children are perishing in the state of Kentucky because of this ‘Structured Decision Making’ tool….'” The judges are right. One has only to look at Kentucky’s commentary in the Children’s Bureau’s report, Child Maltreatment 2022.
An overall decrease for child victims was observed between FFY 2021 and FFY 2022. Kentucky has worked diligently over the past several years to implement a safety model which includes the implementation of SDM® Intake Assessment Tool and a thorough review and modification of the state’s acceptance criteria to ensure a focus upon children and families with true safety threats versus risk factors. This shift in the approach to the work may have contributed to the decrease in child victims this year.
Children’s Bureau, Child Maltreatment 2022, p. 13
In other words, they changed the screening criteria to screen out more cases and voilà! Fewer child victims! Amazing! The percentage of referrals that was screened in decreased from 45.5 percent in 2021 to 39.9 percent in 2022, and the maltreatment substantiation rate decreased from 14.9 to 12.3 per thousand children during the same period. But both of these rates have been decreasing since FFY 2018, so more factors than the new screening tool are likely responsible. It’s unlikely that a decrease in actual maltreatment is among them.
The placement and workforce crises continue
Every month brings another crop of articles on the intertwined placement and workforce shortages plaguing child welfare. February’s news on the placement crisis included a story from Texas Public Radio reporting on the release of hundreds of incident reports about “Children Without Placements” in the state from 2021 to 2023. They include stories of children squaring off to fight each other in the hallway of a Houston hotel that resulted in the hospitalization of one youth. These incidents, occurring at a rate of about two a day, often involved injured staff, injured youth, and calls to police.
In a state that requires some social workers to supervise youths in hotels and other unlicensed placements, its not surprising that about one in four caseworkers left the job in January, according to the head of the Department of Family and Protective Services (DFPS). And even workers who don’t have to supervise unruly youths are dealing with untenable caseloads and terrible working conditions. Some states are taking action to attract and retain workers. The Governor of Maine announced a series of three one-time lump-sum payments of $1,000 to recruit and retain child welfare workers. Let us hope it is enough to reduce the state’s high caseloads.
And now for some good news: efforts to keep siblings together
It’s always nice to read about people who see a need and create a program to meet it. February brought news of two new “foster care villages” to house larger sibling groups, an idea I have promoted in the past. In California, the actor Christian Bale achieved a dream he has nurtured for 16 years–breaking ground on Together California, a new foster home community in Palmdale, Los Angeles County. The project will include a dozen foster homes built to accommodate up to six siblings and staffed by full time, professional foster parents. A 7,000-square foot community center will offer academic, therapeutic, social, and recreational activities for young people in the foster homes and the surrounding community, which is very short on such resources.
In South Carolina, a new foster care “village” called Thornwell is transforming old houses built about 100 years ago to house foster families and large sibling groups. Two homes are in use, a third is under renovation and more homes await renovation provided the funds and parents can be found. Foster parents will pay one dollar of rent per month and receive free utilities. Children will be eligible for Thornwell’s early learning center, charter school, and recreational facilities. Here’s hoping for more programs like Together California and Thornwell!