On December 16, 2025, police were dispatched to a residence in Nampa, Idaho and found a 12-day-old infant named Benji dead in a filthy house with dog feces on the floor. Records show that five children had previously been removed from Benji’s parents due to unsafe living conditions–three in 2019 and two in 2022. Both parents’ rights were terminated to all five children, who were adopted by their foster parents. But that did not save little Benji, despite repeated calls from former foster parents and others asking child protective services (CPS) and police to check on the infant. Less than four months after Benji’s death, the Governor of Idaho signed “Benji’s Law” to expedite safety checks when reports involve infants considered at high risk of abuse or neglect. Unfortunately, Benji’s law does not go far enough. It might have prevented Benji’s death, but not the death of infants who were not the subject of calls to CPS or police.
Benji’s case was not unusual. Having one child who died of abuse or neglect seems, not surprisingly, to be a risk factor for another such tragedy. Here are only a few examples that have recently appeared in the news.
A two-month old infant in Washington State (“F.F.“) was placed on life support and died three days later in December 2024 after allegedly being shaken by his father, who is charged with second degree murder and homicide by abuse. The baby had a brain bleed, four older rib fractures, and a broken collarbone. The father eventually admitted to shaking the baby for five minutes in a fit of anger. The same man was convicted of second-degree crimimal mistreatment after breaking his infant daughter’s femur in 2023. The child was removed and was in foster care at the time of F.F.’s death.
Prosecutors allege that 14-month-old Tilly Servin was was tortured to death in Long Beach, California in November 2025. Tilly’s autopsy showed repeated instances of inflicted trauma including skull fractures and broken bones, as well as evidence that the child was deliberately starved. Her mother is suing Los Angeles County’s child protection agency for leaving Tilly in the custody of her father, who was previously sentenced to four years in prison for exposing two other children to methamphetamine and other drugs in 2021.
In Wichita, Kansas, Shanna Whitton was charged with killing her 15-month-old son in August 2025 by intentionally choking him. The Sheriff’s Department has reopened an investigation into the July 2024 death of Whitton’s two-year-old daughter, which was ruled to be an accidental choking. The child had had been taken to the hospital with injuries at least three times before the choking incident that caused her death.
In the District of Columbia, 20-month-old Kemy Washington was found dead in January 2025 along with the body of her mother, who had overdosed on multiple types of illicit drugs. Kemy had died slowly of starvation and dehydration. Kemy’s older sister had been removed due to her mother’s drug abuse; the child’s guardianship with a relative had been ratified in court only five days after Kemy was born. Kemy’s grandmother called child protective services twice in Kemy’s short life but there was no policy allowing CFSA to investigate Kemy’s safety just because she was born to a mother who lost custody of a previous child for neglect.
Monique Peyre, who adopted three of Benji’s siblings, reported to Idaho News Now that she and others had made multiple calls to the Idaho Department of Health and Welfare (IDHW) and local police asking them to check on Benji in the days before his death, given his parents loss of custody of five other children. She said that IDHW told her they don’t consider history when a new baby is born to a family, and that they had no current concern for the infant. It seems that they finally accepted the referral but labeled it as a “Priority III,” requiring a response within three days and seeing the child within five days. A day later, Benji was dead.
Peyre and others urged the legislature to pass a bill that would require a quicker response to a report of a baby such as Benji. They circulated a petition, spoke to the media and testified before the relevant committees. Benji’s Law was approved by the legislature and was signed by the governor on April 2, 2026. It requires that when any report is made by a mandatory reporter alleging that the parent, guardian or legal custodian of a child aged one or younger has one of four risk factors described in the legislation, IDHD must verify within 12 hours that the reported risk factor is accurate, using internal, criminal or medical records. If the risk factor is verified, the department must initiate a “Priority I Response,” which means that the child must be seen immediately, and the invetigator must complete a full written safety assessment which is described in the law.
The four risk factors listed in the law are: (1) the parent, guardian or legal custodian is listed in the child protection central registry for maltreatment that took place within the past ten years; (2) the parent, guardian or legal custodian has been convicted of an injury to a child; (3) the parent, guardian or legal custodian has had their parental rights terminated due to child abuse or neglect; or (4) a previous child was born with neonatal abstinence syndrome.
Benji’s Law is a good start, but it is far from the comprehensive solution that is needed for children born to parents who have seriously abused or neglected a sibling. The main problem is that it requires an initial report to the agency by a mandated reporter. That leaves out all the babies born to known maltreators who are never reported to the hotline, or reported by someone who is not a mandatory reporter. That rules out the grandmother of Kemy Washington in the District of Columbia, who tried twice to alert the agency to Kemy’s situation. It is often family members, who are not mandatory reporters, who notify child protective services of the danger facing a child born to a known maltreater.
It’s not surprising that the foster and adoptive parents who worked on Benji’s law were trying to address the situation they were facing when they were getting no response to their reports. But it is unfortunate that they did not consider the infants that do not have people looking out for them. They probably did not know that there is a solution well within the reach of any state government. Birth records can be matched against CPS and criminal records, which would identify the infants with first three risk factors cited in the bill. Such a process, called “birth match,” was in use in five states as of May, 2022. (At least three of these states adopted these policies in response to deaths of children born to parents responsible for the death of a previous child.) Each state has a different list of risk factors and a different requirement of what type of assessment must be done when these factors exist. Ideally, Congress would pass a law requiring such a policy as a condition of receiving federal child welfare funds.
The birth of a previous child with neonatal abstinence system, which is one of the risk factors in Benji’s Law, could not be identified by matching birth records with CPS and criminal records. This would probably require a match.with health records, which is authorized in Benji’s Law. However, it is not clear whether the birth of a previous child with neonatal abstinence syndrome makes sense as a reason for investigation. It seems more appropriate to assess the safety of a child who is itself born with neonatal abstinence syndrome and not to use a sibling‘s condition at birth as a trigger for investigation.
Apart from the lack of a birth match, Benji’s law has one major loophole in the definition of risk factors. Ebony Washington of the District of Columbia never had her rights terminated because her first child was placed in guardianship rather than adoption. Relatives often choose guardianship, rather than adoption, to avoid the termination of the parent’s rights. Therefore, the risk category should include all parents who have had a transfer of physical and legal custody due to abuse or neglect of their child.
Monique Peyre, the adoptive parent of Benji’s siblings, had it exactly right when she told Idaho News Now that “[w]hen there’s proven history, convictions, removals, termination of rights, I think there should be more urgency to check on future children rather than sending an infant home to a really high-risk situation…” Not considering history is the ultimate source of so many child and abuse deaths today. Children are left, without monitoring, in situations where history tells us to intervene. We must learn from the past to protect children in the present and future. But the laws and policies designed to do this should protect all children with known risks, not just a select few.
I could not help being skeptical when I read the headline, “Colorado’s child abuse and neglect cases drop 40% in 4 years.” Major changes in social phenomena just don’t happen that fast. And indeed, Colorado’s own data suggests that this “drop” in abuse and neglect reflects little more than an agency’s desire to identify fewer victims.
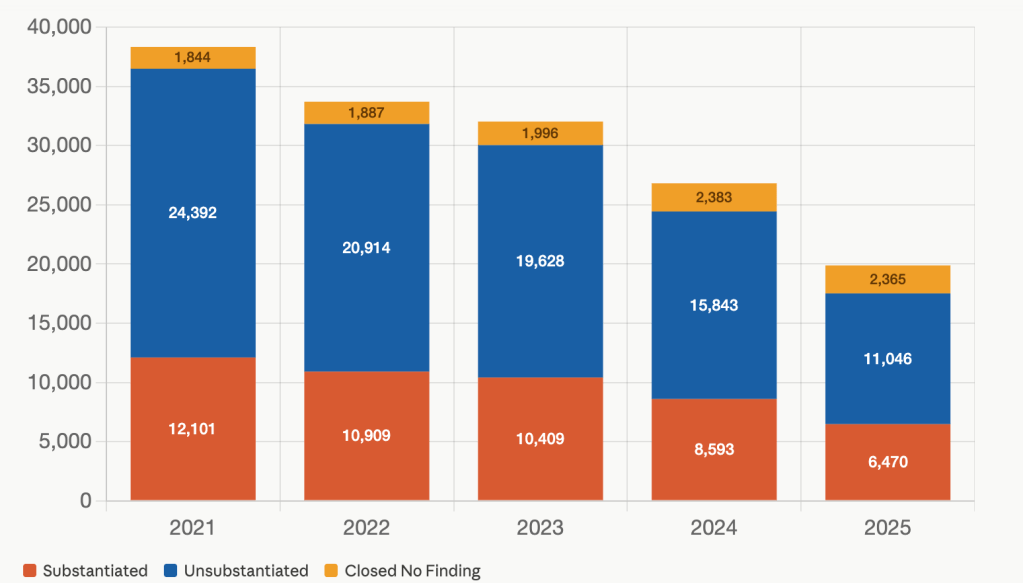
In 2021, according to the public dashboard of the Colorado Department of Human Services (CDHS) as of May 9, 2026, 12,101 children had “experienced substantiated abuse or neglect,” meaning that an investigation confirmed that abuse or neglect had occurred. In 2025, only 6,470 children had experienced substantiated abuse or neglect.
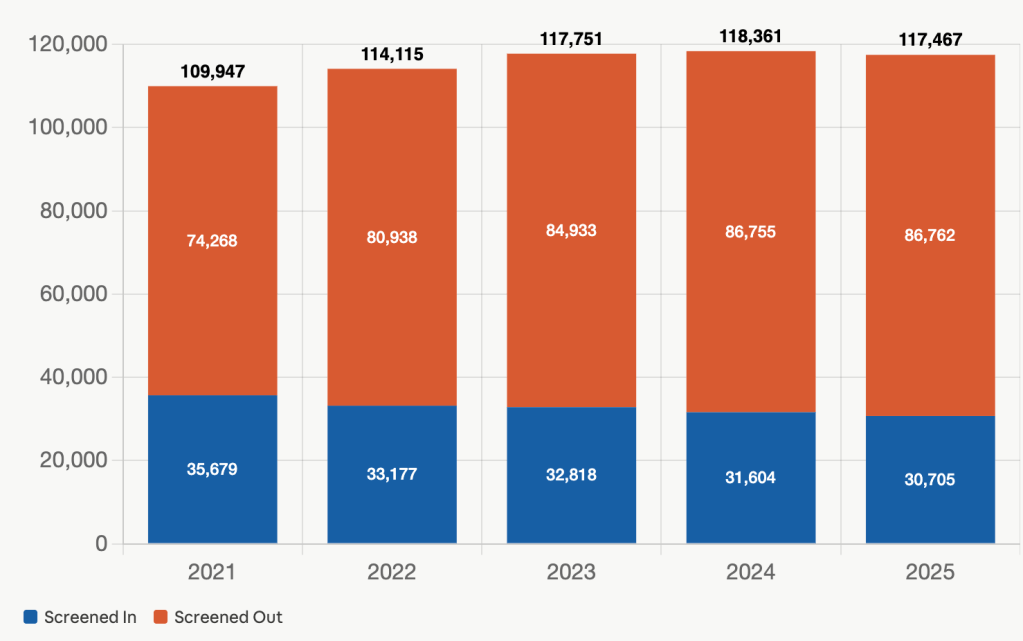
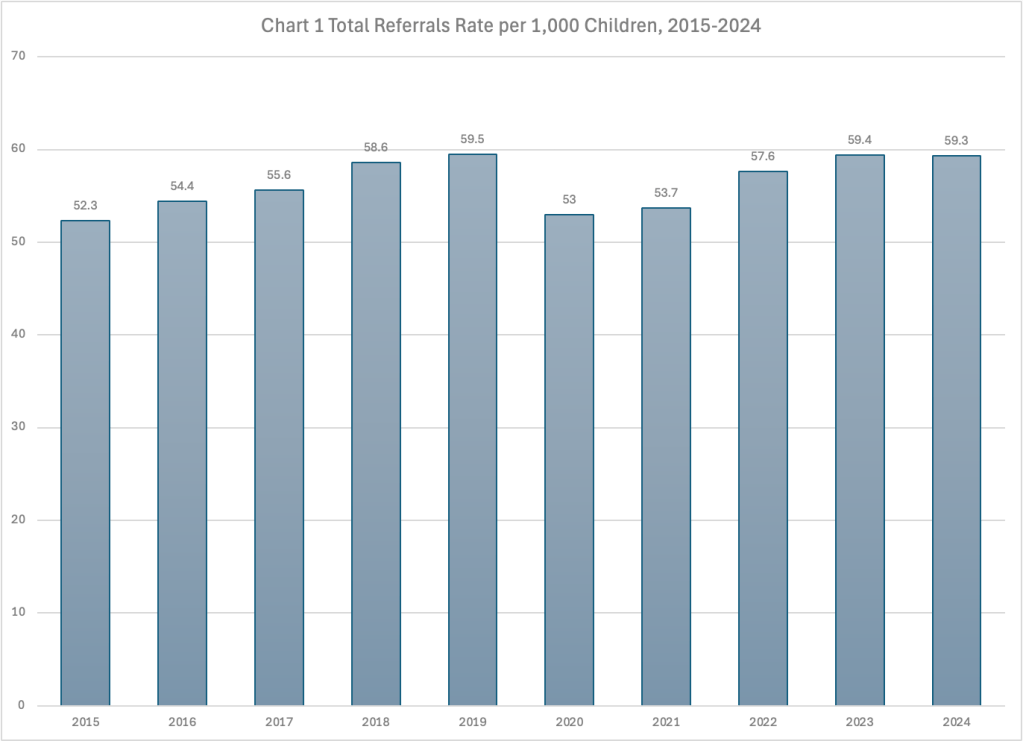
The decrease in confirmed cases of maltreatment was not due to a decrease in calls to the CDHS hotline about suspected abuse or neglect. These reports actually increased in number from 109,947 in 2021 to 117,467 in 2025, according to the Dashboard as of May 10, 2026, as shown in Chart I below. This is likely due in part to schools reopening after the pandemic and teachers being able to see signs of maltreatment.
Chart 1 Total Referrals by Screening Decision, 2021-2025
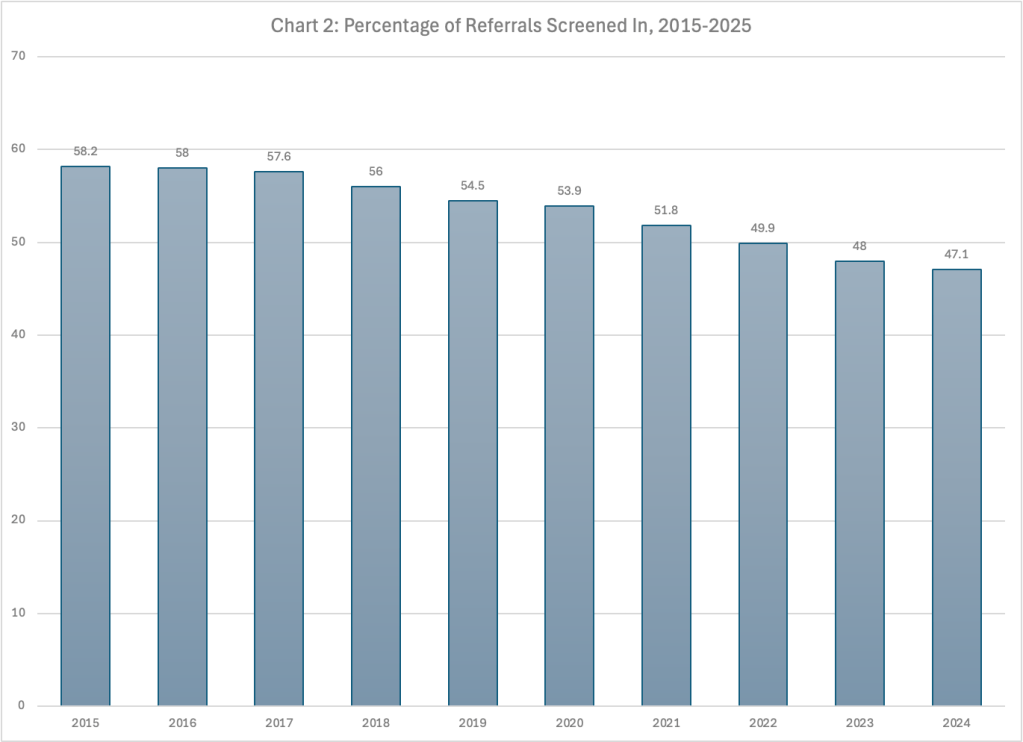
While the number of hotline calls increased, the percent of calls that were “screened in” (accepted) for an in-person response decreased from about a third to a quarter over the same period. As a result, the number of children accepted (as shown in Chart 3) dropped by more than 5,000, reducing the pool of children that could have received a “substantiated” finding.
After a report is accepted, it is assigned to a traditional investigation or a newer, different pathway called Family Assessment Response (FAR). FAR is designed for low to moderate risk cases and does not result in a finding because FAR is designed to be a non-adversarial process. Thus, children who receive a FAR cannot be found to be substantiated victims of abuse or neglect.
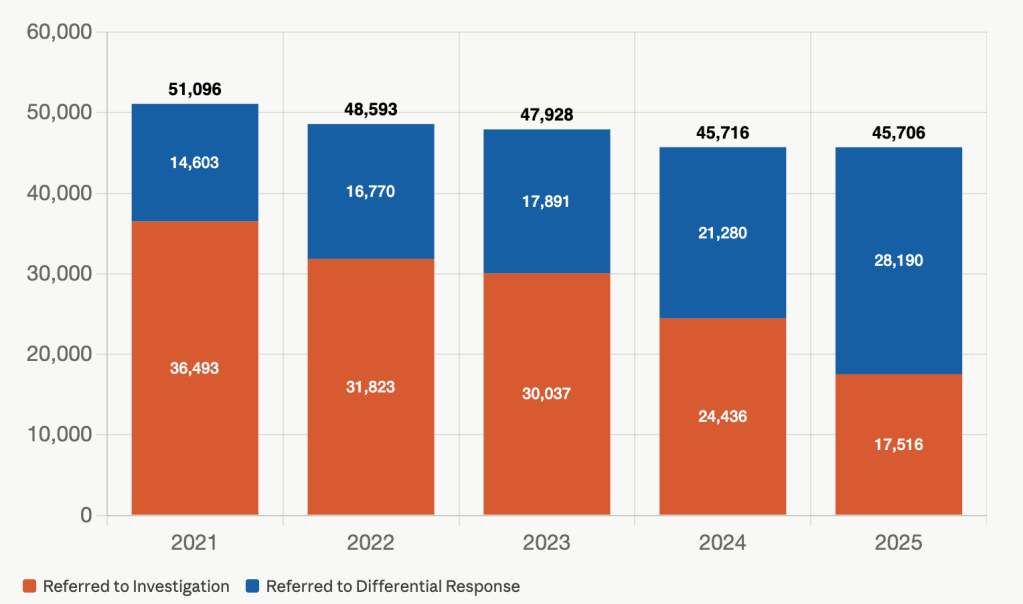
In 2025, 59 percent of the children with screened-in reports were referred to FAR, compared to only 33 percent in 2021. In other words, only 17,516 children were the subject of an investigation in 2025 compared to 36,493 children in 2021—less than half as many children–as shown in Chart 2.
Chart 2: Children Referred to Investigation and Differential Response, 2021-2025
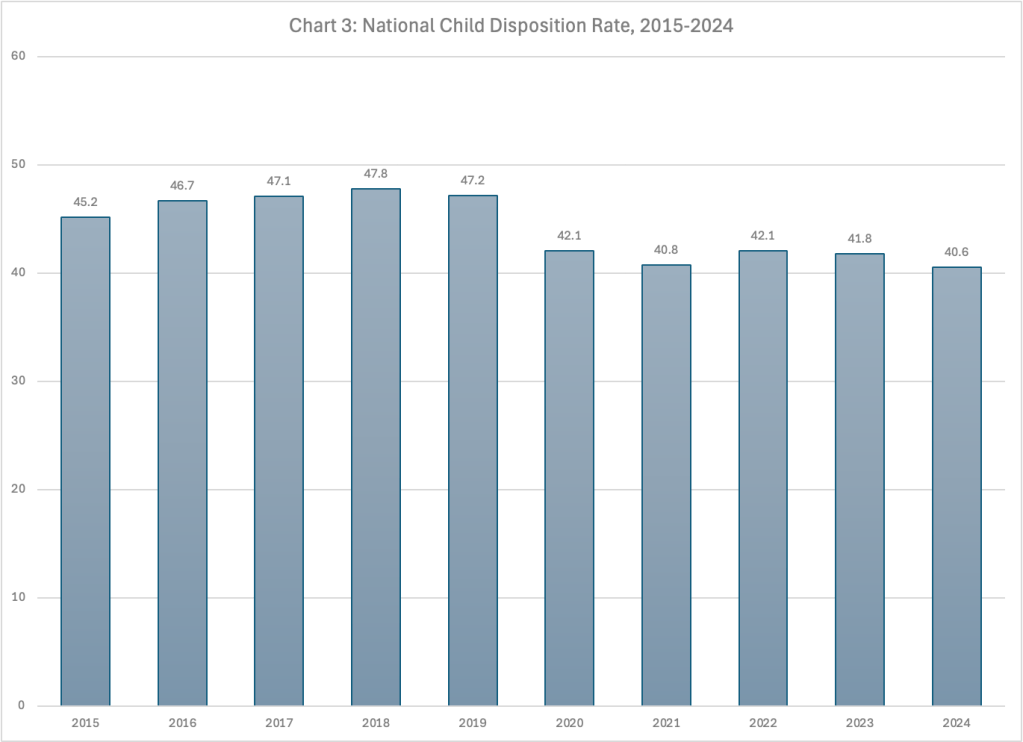
Given the more than 50 percent drop in the number of children who received an investigation, it is not surprising that the number of children with substantiated findings of abuse or neglect dropped by almost 50 percent. Chart 3 shows how the number of children receiving a substantiated finding declined with the drop in the total number of children receiving an investigation.
Chart 3: Children Receiving an Investigation by Disposition, 2021-2025
But why did the number of children assigned to FAR more than double from 2021 to 2025? A CDHS spokesperson told me that the increase in the percentage of assessments assigned as a FAR between 2021 and 2025 is due to 21 additional counties, including two high-volume metro counties, adding the FAR option during the period.
Advocates and researchers have expressed concern that the overuse of an option like FAR can leave children in harm’s way when they are inappropriately assigned to it.
The reductions in the number of children screened in and the increased use of FAR reflect a loss of interest by CDHS in traditional child welfare services to protect children who are already being maltreated–investigation, in-home services and foster care.
Instead of intervening to protect children who are being abused or neglected, “the state has tried to get upstream from abuse and neglect, raising awareness of resources and encouraging the general community to support families,” Thomas Miller, director of children, aging and community services at CDHS told the Post. But Colorado’s new emphasis on prevention has not been accompanied by new resources or programs, according to the CDHS spokesperson.
Miller told the Post that “the majority of abuse cases are avoidable if parents have the right coping skills, the material resources their families need and social support for the inevitable difficult times.” He has a list of 50 ways for neighbors and community organizations to support families that may be at risk of maltreating their children.
It all sounds so simple. Apparently Miller has no concern about the confluence of substance abuse, mental illness, and domestic violence that characterize the families that are frequently encountered by child welfare, problems that are rarely solved by some coping tips or more money.
The Post suggests that Colorado’s new approach has helped reduce child abuse and neglect. But without evidence of such a decline, there is no reason to celebrate.
Some of my happiest days as a social worker were the days I was able to celebrate the adoption of a child by loving foster parents that I had worked with since the child was placed with thm. I will never forget these people that opened their homes and their hearts to a child who was not born to them but who needed their loving care. They were parents in every sense of the word but the biological. Yet, a minority of adoptive parents do not fit this description or even the minimal definition of an adequate parent.
On March 26, an SUV carrying Jennifer and Sarah Hart and their six adopted children drove off a cliff into the Pacific Ocean in Northern California. Days before the crash, Washington State’s Department of Children Youth and Families had opened an investigation of the family after a neighbor called the child abuse hotline. It turned out that the family had a history of abuse reports in three states, starting even before three of the children were adopted. Eventually, we learned that Jennifer and Sarah Hart had received thousands of dollars in adoption subsidies to care for these children while they starved and abused them for years. If federal law had required an annual check-in with the children, they might have been spared years of suffering and untimely death.
There have been many reports of parents collecting adoption subsidies while abusing and neglecting their children or even after killing them. Michael and Shirley Gray collected $3,000 in adoption subsidies per month for four out of their five children adopted in two Tennessee counties while starving them and confining them in cages and closets. Two of the children died and were buried on the family’s property while the parents continued to receive the subsidies. In Iowa, Sabrina Ray and Natalie Finn died of starvation at the hands of their adoptive parents, and Malaiya Knapp ran away from her adoptive home after being locked in a basement and abused for years. Renee Bowman in Maryland beat, choked and starved all three of her children adopted from DC foster care. She killed two of them and kept their bodies on ice in a freezer while collecting $150,000 for raising them. Edward and Linda Bryant in Colorado collected $175,000 in subsidies for the adoption of two boys in 2000; they have not been seen since 2001 and 2003.
Reports of egregious or even fatal abuse of children adopted from foster care appear surprisingly often in the media, but most of these reports do not mention subsidies. But since the vast majority of parents who adopt from foster care (90 percent between 2005 and 2016) receive subsidies, it is likely that most of these “parents” were receiving them.
More common than horrific abuse and neglect are “broken adoptions,” in which the child is legally adopted but is no longer being cared for by the adoptive parents. A survey of 383 youth and adults who exited foster care to adoption1 found that almost 10 percent of the adoptees experienced “formal placement instability;” about eight percent reported re-entering foster care and almost two percent reporting the termination of their adoptive parents’ parental rights or emancipation before the age of 18. Another 30 percent of survey participants reported that they experienced “informal post-adoption instability,” including running away, leaving home before age 18, living with a nonrelative adult other than the adoptive parent, or being homeless. It is worth noting that some adoptive parents (like some birth parents) relinquish their highly challenging children to foster care in order to obtain behavioral health care and fully expecting to get them back. I do not consider these to be broken adoptions unless the parents refuse to take them back after their symptoms have been alleviated.
We do not know how many adoptive parents or guardians continue to receive subsidies after they have permanently stopped caring for their children. But In New York State, this issue has been on the radar of legislators and advocates for more than a decade. Advocacy and services groups in New York City began reporting in the 2010’s that they were working with children who were struggling to survive after leaving or being kicked out by their adoptive parents. The city’s Children’s Law Center set up a project to study these broken adoptions and publicized egregious cases, such as a sibling group whose adoptive parents had received over $200,000 in subsidies after the adoption had broken and and an adoptive father who continued to accrue subsidy payments for his children in jail after he murdered the adoptive mother. New York City’s Daily Newsreported in 2014 that a judicial hearing officer said he dealt with “hundreds” of cases a year where adoptive parents continued receiving subsidies after their children had left their homes. In a letter to the federal Administration on Children and Families (ACF) in 2015, the Commissioner of the city’s Administration for Children’s Services reported that in a single month during the previous year the agency had made subsidy payments for 143 adopted children who had already returned to foster care. That means the government was paying twice for the same children, with one payment going to the foster parent and another to the adoptive parent who was no longer caring for the child.
How can adoptive parents and guardians continue collecting subsidy payments for children that they have stopped caring for, neglected, abused or even killed? The Adoption Assistance and Child Welfare Act of 1980 (AACWA) established the adoption subsidy program to address widespread concern that many children were languishing in foster care because foster parents would have to give up their subsidies in order to adopt. The Fostering Connections to Success and Increasing Adoptions Act of 2008 added the guardianship subsidy program. According to Federal statutes 42 U.S.C. § 673, an adoption or guardianship subsidy may not be paid if the child has turned 18 or 21 (depending state policy and whether the child has a disability), if the state determines that the parents or guardians are no longer legally responsible for the support of the child, or if the state determines that the child is no longer receiving any support from the parents or relative guardians. But the statute provides no mechanism for the state to determine that the parents or guardians are no longer supporting the child. Instead, it states that parents or relative guardians “who have been receiving adoption assistance payments or kinship guardianship assistance payments under this section shall keep the State or local agency administering the program under this section informed of circumstances which would, pursuant to this subsection, make them ineligible for the payments, or eligible for the payments in a different amount.”
Government financial assistance programs do not generally leave it up to the recipient to inform the government that they are no longer eligible for benefits. Other than social security retirement and survivor benefits (which are meant to last a lifetime), federal assistance programs generally require a periodic redetermination of a recipient’s need for assistance. Members of the 96th Congress apparently did not suspect that adoptive parents would abuse, neglect or abandon their adopted children or that they would fraudulently collect adoption subsidies. However, it is important to note that the law does not actually forbid states from requiring periodic redetermination of the need for an adoption subsidy and the wellbeing of the adopted child. Unfortunately, the federal Administration for Children and Families (ACF) has misinterpreted the law to impose such a prohibition.
On December 31, 2007, ACF added to its Child Welfare Policy Manual (CWPM) a new question and answer about adoption subsidies. The new text stated that a title IV-E agency “cannot reduce or suspend adoption assistance solely because the adoptive parents fail to reply to the its request for information, renewal or recertification of the agreement. Once an eligible child is receiving title IV-E adoption assistance pursuant to an agreement, adoption assistance continues until either the adoptive parents concur to a change or one of the statutory conditions are met for termination of the assistance.” The answer continues: “Once an eligible child is receiving title IV-E adoption assistance pursuant to an agreement, adoption assistance continues until either the adoptive parents concur to a change or one of the statutory conditions are met for termination of the assistance (section 473(a)(4) of the Social Security Act and [CWPM] Section 8.2B.9 Q/A #2).”
As mentioned above, section 473(1)(4) of the Social Security Act says that adoption or guardianship assistance cannot be paid after the child ages out or if the state determines that the parents are no longer supporting or responsible for supporting the child. But in a 2001 policy announcement (later incorporated into the CWPM section referenced above) the agency changed the wording to: “[o]nce an adoption assistance agreement is signed and in effect, it can be terminated under the following circumstances only.” Saying the assistance cannot be paid if these circumstances exist is very different from saying the subsidies can be terminated only if these circumstances exist. ACF’s interpretation denies states the opportunity to determine whether the conditions for ending the subsidy are present.
ACF has continued to obstruct any effort to protect children adopted from foster care and impose fiscal discipline on the subsidy program. Twenty-eight years after the passage of AACWA, the 110th Congress passed the Fostering Connections to Success and Increasing Adoptions Act of 2008, which required that every state plan for foster care and adoption assistance provide assurances that each school-age child is indeed attending school or has completed secondary school. To comply with this requirement, New York’s Office of Children and Family Services (OCFS) adopted a new regulation2 requiring local offices to notify adoption subsidy recipients annually that they must certify that their school-age children are in school or have completed high school. The notice had to include a reminder of parents’ obligation to support the child (!!!) and of notify the local agency if they are no longer providing support for the child or are no longer legally responsible to do so. But there was some discussion in OCFS, according to an Administrative Issuance that has since been cancelled, about what to do when adoptive parents do not comply with the request for a certification. Also, there were “questions raised” about “when submission of additional proof (relevant to both support and school attendance) beyond certification, can, or should, be requested.” OCFS brought these questions to ACF and was told in no uncertain terms that “because the federal adoption assistance program is an entitlement, the state may not impose additional criteria beyond the federal requirements.”3 Furthermore, stated OCFS, “ACF advised against any intensive or intrusive inquiry into an adoptive family’s life.” The requirement for certification was allowed, but no attempt to verify it or even follow up when a parent did not answer. Despite Congress’ desire to ensure that all children receiving foster care and adoption assistance were in school, ACF was adamant that no verification was allowed.
The federal government’s pressure on states to keep the pipeline from foster care to adoption flowing has obviously not abated. The American Bar Association has suggested that this pressure may in fact be leading to an increase in the number of adoptions that fail as states encourage adoptions by foster parents who are not actually capable of meeting the children’s needs. The story of Krista and Tyler Schindley illustrates how such pressure can lead to disaster. The Schindleys were sentenced to 40 years in prison for the horrific abuse and attempted murder of their 10-year-old adopted son in Spalding County, Georgia. A neighbor had found the emaciated boy, who had escaped the house where he had been locked up, starved, and beaten. Three years before his escape, the Schindleys had adopted the boy along with his two sets of twin siblings, despite dire warnings against allowing them to do so. A school counselor told the Division of Children and Family Services (DCFS) caseworker that the adoptive mother did not want the boy and urged the agency not to proceed with the adoption. Even worse, the private faith-based foster and adoption agency that placed the children with the Schindleys eventually dropped the plan of adoption and revoked the family’s foster care license, telling DCFS that “the Schindleys were not fit to adopt the boy, or other children.” Unbelievably, DCFS re-licensed the foster home and pushed through the adoption. When the Title IV-E agency has no priority higher than shifting children from foster care to adoption, such things can happen.
The number of children in adoptive or guardianship has been quietly increasing as a portion of total Title IV-E caseload since the passage of the Adoption Assistance and Safe Families Act in 1990. While children in foster care were 79 percent of the Total IV-E subsidy caseload in 1990, they had fallen to 17 percent of the subsidy caseload by 2023, with the remaining 83 percent receiving adoption and guardianship subsidies. This is mainly due to the fact that Congress restricted eligibility for federal reimbursement of foster care subsidies as part of welfare reform in 1996 but exempted adoption subsidies from these limits. In FY 2024, an estimated 554,000 children received IV-E adoption subsides each month, 46,000 received guardianship subsidies, and 112,000 received foster care subsidies. In FY 2025, the federal government spent $4.479 billion on adoption and guardianship assistance, which is between 50 and 83 percent of the amount spent by each state or tribe.4
In 2025, after eight years of advocacy, the governor of New York finally signed a bill5 designed to address the problem of fraudulent adoption subsidy receipt, but it is only a very weak start. It requires parents to “certify annually” that they are fulfilling the obligations of their adoption subsidy agreement. But no documentation is required, so any parent can certify that they are fulfilling these obligations regardless of whether the child is even alive, let alone well-cared for. It is only if the parent fails to certify that the state agency is directed to “review all available information in order to confirm the parents’ continued eligibility to receive the subsidy.” Something much stronger is needed.
In order to protect children adopted from foster care, or those who leave foster care for guardianship, there should be at least an annual process to verify that each child is alive, well, and still being supported by the adoptive parents or guardians. The best way to implement this would probably be through a face-to-face meeting with the child. Like a CPS interview, this should be conducted out of earshot of the adoptive parents or guardians. In its Blueprint for Child Welfare Financing, published in 2025, the Child Welfare Financing and Accountability Working Group of the Bipartisan Policy Institute recommended that states be required to conduct annual wellness checks of children as a condition of IV-E reimbursement for subsidy payments. Perhaps there is a way to verify a child’s wellbeing and a parent’s support without a face-to-face meeting, using documentation from a school or pediatrician. What is clear is that there needs to be some process to evaluate the child’s well-being and the parents’ support at least yearly. There is nothing in the law that forbids such a check-in, but it is clear that Congress must act to make it happen.
When foster parents received a subsidy and adoptive parents did not, a perverse incentive kept children in foster care. But when adoption subsidies were added, they did not come with the monthly or bimonthly visits from a social worker that foster care requires. And that provision of money, without oversight, had perverse consequences of its own. The expenditure of billions of dollars without any controls (and the knowledge that at least thousands have been fraudulently spent) would be proof in itself of the need for a change. But the existence of not one or two, but many cases of severe abuse and neglect and sometimes death in these homes, there is no morally acceptable excuse for failing to check on these families. Given what we know now, it is immoral to continue offering adoption subsidies without at least annually verifying that the children are alive, well, and being supported by the adoptive parents who are receiving taxpayers’ money to care for them.
Notes
These were children from the National Surveys of Children and Adolescent Well-being NSCAW I and II are longitudinal surveys of children and families who were subject to Child Protective Services (CPS) investigation. For this study, the researchers conducted new surveys with the families of children who were identified as adopted prior to the end of the original NSCAW I study period (August 2005-December 2007) or the original NSCAW II study period (June 2011 to December 2012). ↩︎
A new report from the Government Accountability Office (GAO) has revealed what many of us have expected: implementation of the Family First Prevention Services Act (often called “Family First”) has not reduced the use of congregate care in most states. There is no reason to be surprised. The failure of Family First to achieve this goal was predicted from the start. Requiring states to stop using existing congregate care facilities while making it difficult to provide alternative placements was not only bound but actually designed to fail as a consequence of the revenue neutrality that was built into the law. GAO’s lack of substantial recommendations to solve the problem is disappointing, as is the failure of Senator Wyden to recognize the fundamental flaws in the law he created and pushed through Congress in 2018.
Family First, passed as part of the Bipartisan Budget Act and signed by President Trump in 2018,1 made two major changes in existing law. Part One extended funding under Title IV-E of the Social Security Act to programs designed to keep children safely at home or with relatives instead of being placed in foster care. Part IV, which is the subject of this post, was to limit funding for all placements that are not foster homes. Such placements are often labeled as “congregate care,” and include group homes, residential treatment centers, and any setting other than a family foster home. While federal funds could be claimed for the placement of any youth in such a setting before Family First, the law limited both the types of congregate care settings that can be funded and the characteristics of the youths who could be placed in these facilities with federal funds. The rationale for these limits was that most children do better in families than in group or institutional settings and that many children were placed in congregate care for lack of an alternative. For those youths who truly need congregate care, the goal was to ensure that these settings are high-quality and truly therapeutic
To reduce the placement of children in congregate care and ensure that such settings are appropriate when used, Family First limited reimbursement for children placed in congregate care facilities after 14 days to four categories (1) a new placement type called a Quality Residential Treatment Program (QRTP) designed for children with “serious emotional or behavioral disorders or disturbances;” (2) a setting designed for pregnant or parenting youth; (3) an independent living setting for youth over age 18; and (4) a setting for children who “have been found to be, or are at risk of becoming, sex trafficking victims.”
As defined in Family First,a QRTP must have a trauma-informed treatment model, have registered or licensed nursing staff available 24/7, have provisions for family involvement in a child’s treatment, be licensed and accredited, and provide “discharge planning and family-based aftercare support for at least six months post-discharge.” To be placed in a QRTP, a youth must be assessed by a “qualified individual” to determine whether his or her needs can be met in a foster family home or with family. If the assessment recommends the placement, it must be approved by a court and reconsidered at every permanency hearing, and the agency head must approve placement in a QRTP for more than 12 months.
Despite Family First’s goal of reducing the use of congregate care, the new GAO Report found that there has been no reduction in the use of such care in the majority of states.2 Based on survey responses from 49 states in in the first half of 2025, GAO found that 26 of these states reported that the percentage of their foster youth who were placed in congregate care settings had either increased or remained the same compared to October 2021. Moreover, 26 states reported that the average number of days that youths spent in congregate care either increased or stayed the same in the same period. Forty-two states reported that they continued to use “stopgap placements” like hotel rooms, office buildings, and hotel emergency rooms because other placements were unavailable. More states reported an increase than a decrease in how much time youths spent at stopgap placements and emergency shelters over the period. And 43 states reported using out-of-state placements, with 29 of them reporting that the use of these placements had increased since October 2021.
GAO found that 34 states (more than two-thirds of the states responding) had at least some QRTP’s. But unfortunately, states were not able to open enough QRTP’s (through conversion of existing facilities to QRTP’s or establishment of new ones) to eliminate congregate care placements that did not meet Family First standards. Of those 34 states, half reported that 50 percent or less of their child welfare congregate care facilities were QRTP’s. Thirty states reported that meeting QRTP requirements was challenging. The requirement that states reported was most difficult to meet was providing family-based aftercare support for at least six months after discharge. Of the 15 states that had no QRTP’s, several reported that the time or cost of meeting QRTP requirements was too burdensome; some said that providers could not meet the requirements. Two states reported that they had implemented QRTP’s but that the facilities had closed or implementation had been paused because of difficulties in meeting the requirements.
With the new limitations on congregate care reimbursement and the difficulty of establishing QRTP’s, GAO found that “the majority of states increased their own spending on congregate care as federal funding diminished.” Twenty-nine of the 49 responding states reported increasing the amount of state, county or local funds used to support youths in congregate care. Drawing from its visits to four states, GAO reported that:
An official in one of these states told us that the goal of reducing the use of congregate care was well intended, but noted that in practice, some youth still required congregate care. Officials in another of these states said that in many cases the state must now pay for the same services that it previously paid for with Title IV-E funds to prevent youth from sleeping in offices or other inappropriate settings. Officials also said that a lack of foster homes and youths’ challenging behaviors made placing youth with families difficult. This leaves the state few options but to continue to place youth in congregate care and pay for those placements with state funds…..Officials in three of four states we visited said that Family First shifted congregate care costs to states. State officials noted that the decline in the percent of federal funds for congregate care since the passage of Family First has been quite large.
In open-ended survey responses, several states reported that the need to shift state and local funds to congregate care has reduced funding for other important priorities, including community based and prevention services and workforce support and training.
All 49 responding states reported challenges in securing enough foster care placements in general, including ten states reporting a challenge in finding family foster homes, both relative and nonrelative, and four reporting a challenge in finding therapeutic foster homes. But securing enough congregate care placements was a challenge for almost all the states. Forty-seven states reported that finding “step-down beds”3 for young people in congregate care was at least a moderate challenge and thirty-nine states reported a lack of behavioral health congregate care placements was at least a moderate challenge.
With only ten states reporting a lack of foster homes as a challenge and compared to 39 reporting the lack of behavioral health congregate care placements as a challenge, it is clear that the placement crisis is worst for children who need the intensive services and supervision only congregate placements can provide. Forty-one state child welfare agencies reported that finding placements for youth with significant behavioral challenges, autism, or intellectual disabilities was very or extremely challenging. And these children, often called “high acuity youth,” are becoming more prevalent in foster care caseloads. Officials in all four states that GAO visited reported that the severity of foster youths’ needs had increased.
Recent news from Tennessee shows how desperate the situation can get. The Department of Children’s Services is supporting a bill that would allow foster children to be locked up in detention centers without being charged with a crime. The bill would create a new class of foster children called “Children in Need of Heightened Supervision,” who could be placed in juvenile jails without any charges. The department claims that these children are violent and there is no other facility that can supervise them adequately.
GAO’s findings should not have been a surprise to anyone. The Family First Act was designed to be revenue-neutral, so that any increased costs would have to be balanced out by savings. Since Part I was expected to result in new expenditures for prevention services, there had to be an equivalent amount of savings, and much of that savings would have to come from reduced spending for congregate care. The Congressional Budget Office in its 2016 cost estimate projected that that ” because states would take several years to recruit and retain additional foster parents, many states would not have enough placements for all children eligible under Title IV-E. CBO estimated that about 70 percent of the children residing in group settings other than [QRTP’s] in 2020 would simply become ineligible for any reimbursement under title IV-E.” Thus, states would be paying the entire cost of these congregate care placements rather than close to half the cost as they were before. Over the ten-year period from 2017 to 2026, CBO estimated that the restriction on non-family placements would on net reduce direct federal spending by $910 million, which would offset almost 70% of the costs of extending IV-E reimbursement to family preservation services.4
CBO expected that the fraction of children whose placements would not be eligible for funding would decrease in future years as the states recruited and retained more foster parents. The cost estimators apparently assumed the entire “placement gap” created by Family First could eventually be filled by recruiting and retaining more foster parents. Their lack of understanding that many of the youths in need of placements have needs and behaviors that are too severe to be met in a normal foster home is quite surprising.
Anyone who claims to be surprised at the GAO results is either disingenuous or has a memory problem. Family First could have achieved its Part IV goal only with less restrictive standards for QRTP’s or increased financial assistance to help states establish or convert existing facilities into QRTP’s. I called attention to the problem before the law was passed in a post called The Family First Act: A Bad Bill that Won’t Go Away.
Surprisingly, GAO has only one recommendation to improve the situation. That recommendation is based on its finding that some states are taking advantage of the lack of guidance about how to define a setting for children who “have been found to be, or are at risk of becoming, sex trafficking victims,” which is one of four settings for which states are allowed to receive IV-E funds after a child has been there for fourteen days. Because this term is not defined and federal guidance provides no further information on how to interpret it, states have been interpreting this language in different ways. For example, at least one state has designated all of its congregate care facilities as this type of setting and claims IV-E funding for all children in congregate care in the state. Other states believe they can claim IV-E funding for any youth placed in a facility designated for actual or potential victims of sex trafficking. Still other states require that a youth placed in such a facility must be individually assessed as a victim or at risk of sex trafficking to be eligible for Title IV-E funds.
Because these different interpretations can result in disparities in Title IV-E funding between states, GAO recommended that The Secretary of Health and Human Services should direct the Administration for Children and Families to clarify its guidance on the appropriate use of Title IV-E funds for youth in facilities designated as settings “providing high-quality residential care and supportive services to children and youth who have been found to be, or are at risk of becoming, sex trafficking victims.”
GAO’s recommendation is shockingly narrow. Having found that the most challenging requirement for a QRTP was providing family-based aftercare support for at least six months after discharge, it is surprising that GAO did not suggest that Congress modify that requirement. It might be more appropriate and realistic to require that each child receive six months of aftercare after attending a QRTP rather than requiring that the QRTP provide that care.
Another recommendation is strikingly missing in the GAO report: exempting QRTP’s from the “IMD exclusion.” An “Institution for Mental Disease” (IMD) is an facility with more than 16 beds that cares for people with “mental diseases.” The “IMD Exclusion” prohibits states from using Medicaid to pay for care provided in IMD’s. This exclusion dates back to the creation of Medicaid in 1965 and was put in place to prohibit the use of Medicaid funds to pay for large mental institutions. The problem is that QRTP’s of more than 16 beds will probably fall victim to the IMD exclusion. According to a letter to Congress signed by more than 500 organizations, “Many high-quality, licensed, and accredited residential providers are considered to have over 16 beds because the bed count includes all beds on a campus or under common ownership, rather than the number of beds in each separate unit, cottage, or family-style home. Further, FFPSA did not include a size restriction in the QRTP requirements, and there is no evidence that programs with 16 beds produce better outcomes than programs with greater capacity.” The letter calls for Congress to fix this problem by exempting QRTP’s from being classified by Center for Medicare and Medicaid Services (part of HHS) as IMD’s. Bills were introduced in 2021 and 2023 to accomplish this, but they did not advance to the floor.5 Senator Ron Wyden, prime architect of the Family First Act, who chaired the Senate Finance Committee from 2021 to 2025, has ignored numerous pleas to fix the IMD exclusion.
It is strange that the term “IMD” does not even appear in the GAO report. The intersection between QRTP’s and the IMD exclusion has been a source of consternation among states and residential providers since the passage of Family First. Over 600 organizations signed the letter to Congress asking it to exempt QRTP’s from this provision. It is quite strange that GAO did not ask about the impact of the IMD exclusion, and it is hard to believe that the states did not mention it in their survey responses or conversations with GAO.
By cynically or naively shifting cost of needed congregate care from the federal government to the states, Congress failed the children most damaged by abuse and neglect. And GAO missed its opportunity to tell Congress that it was responsible for fixing the problems that it created. So it is not surprising that instead of trying to fix the flaws in Family First, like the IMD Exclusion and the overly restrictive QRTP requirements. Senator Wyden chose to criticize ACF for not enforcing its standards, saying “I will continue to hold Alex Adams and the Administration for Children and Families accountable for any action or inaction that allows the intent of the bipartisan Family First Act to be tarnished.” To write a bad bill for which anyone with clear eyes could see the consequences, to refuse to fix it once the effects became clear, and then to demand that it be enforced is betrayal of the most traumatized and needy children in foster care around the nation.
Author’s Note: The same day as I posted this blog, the nonprofit newsroom Searchlight New Mexico published an article reporting that agencies providing treatment foster care (TFC) for New Mexico’s Children Youth and Families Department (CFYD) were turning down referrals of hard-to-place youth. Among those rejected were a teenage girl who had shot and killed her father and another teenager who was currently placed in a psychiatric ward for extreme and aggressive sexual behaviors. As the director of the treatment foster care agency wrote to legislators “These are just two examples of the types of referrals we receive on a constant basis that are not clinically appropriate” for treatment foster care….These are the children that are routinely staying in CYFD offices because TFC agencies say no.” In recent years, CYFD has referred hundreds of children to TFC agencies, and most of them have been rejected. CFYD told Searchlight that all of these children were assessed and approved for TFC by the agency and “managed care providers.” According to the CYFD spokesperson, “The issue isn’t that a child doesn’t meet the clinical need of the TFC, it is that the TFC agency doesn’t have a TFC family that matches to the clinical needs.”
Really? As the Searchlight article explains, these children being turned down have bounced from home to home for years, interspersed with stays in offices and hotels. By the time they are referred to TFC, they need round-the-clock supervision and care, which TFC families are not equipped not provide. These are family homes, after all. Not to mention the fact that no foster home is prepared for children who have killed or displayed extreme and aggressive sexual behaviors. But the needed 24-hour care does not exist in New Mexico. Many residential treatment facilities have shut down, and the state does not have a single QRTP. As the TFC director told Searchlight, “I’m not saying all these kids need to be in residential treatment centers. But what we’ve done is we’ve gone from a system that actually had providers at each level of care to a system that has hardly anything. So there’s nowhere to send these kids.”
And yet CYFD is still trying to force these children into TFC homes. Searchlight reported on a new sense of optimism now that the parties in the Kevin S settlement are setting a new annual target for TFC placements. The power of wishful thinking is great indeed.
It is truly unfortunate that GAO does not list the answers by state. It is the total number of children experiencing these conditions that matters more than the number of states that experienced a decline. ↩︎
This term generally refers to a placement that is less intensive and restrictive than the previous level, but more intensive than traditional foster care. It could be a less restrictive congregate care placement or a therapeutic foster home. ↩︎
This cost estimate was for the Family First Prevention Services Act of 2016. This bill was incorporated and passed, with some changes, in the Bipartisan Budget Act of 2018. The CBO cost estimate for this bill does not contain a detailed narrative about Family First but reduces the estimated savings from the congregate care restrictions to $641. It is not clear why the savings estimate was reduced but it is clear that these provisions were still expected to produce savings. ↩︎
The 2023 bill was included by the House Energy and Commerce Committee’s Subcommittee on Health as part of the SUPPORT Act but was not included in the act that was passed. In its FY 2021 budget, the Trump Administration also asked Congress to exempt QRTP’s from the IMD exclusion ↩︎
I Saw a Child Who Seemed Neglected. Should I Have Done Something? was the title of a column from Kwame Anthony Appiah, who writes the “Ethicist” Column for the New York Times. Appiah is a respected philosopher and writer, but he lacks in-depth knowledge about the child welfare system. In this case, he was relying on misinformation about our child protection system that has become so prevalent that it is taken for truth.
The anonymous writer told The Ethicist about a child she saw in her home town in upstate New York, which she described as a poor rural area that has been hit hard by the lost of industry and the opioid epidemic. On a “bitterly cold day,” she stopped into a local dollar store and saw two young woman who entered with a child under five years old. She noticed the child was wearing only shorts and a T-shirt, with no socks or shoes. The child also appeared extremely dirty, as if the child had not been bathed in days. The writer also noticed that the child’s hair was dyed neon green and he or she had black nail polish on fingers and toes. It seemed odd to her that somebody found time for these “fun touches” while basic care was missing. As the group left the store, she noticed the child stepping barefoot into slush and climbing into a car where the driver was smoking a cigarette. She watched the group drive away and reported, “I couldn’t shake the feeling that I may have seen a child who needed help and I simply walked away. At the same time, I worry that I’m piling assumptions onto a family I know nothing about, a family that might be doing its best. … I also know that calling Child Protective Services can create serious harm for families who don’t deserve it. What should I have done?”
Here is “The Ethicist’s” answer, paragraph by paragraph, followed by my response,:
This probably wouldn’t be a hard call if we all trusted the ability of social services to intervene — and to refrain from intervening — thoughtfully and protectively. After all, child abuse and neglect take place on a distressing scale. In an ideal world, you could note the car’s plate number, report what you’d seen and be confident that you were more likely to help than harm. A widespread concern, though, is that C.P.S. can do a great deal of damage; indeed, some child-welfare experts have concluded that, on net, these programs do more harm than good.
Many of these “child welfare experts” that Appiah is talking about cite statistics showing the abysmal outcomes of youth who age out of foster care, such as low high school graduation and college attendance rates and high rates of teen pregnancy, homelessness and criminal justice involvement. They often talk about “the foster-care-to-prison pipeline.” But we do not know the extent to which these bad outcomes reflect the child’s earlier experiences at home versus the effects of foster care. Many of the children who are removed from abusive or neglectful homes might have fared even worse if they not been removed. It is certainly a shame that we do not have a foster care system that is nurturing and generous enough to erase the disadvantages with which children enter it, but that is not to say that our inadequate foster care system is responsible for the poor outcomes that foster children and youth experience. Moreover, youths who age out of care (the ones who are usually studied) are likely more disadvantaged than the majority of foster youth who return home, go to relatives, or get adopted, and using them to gauge the impact of foster care is misleading.
Whether foster care does more harm than good is a difficult question to research because it is not possible to do a controlled experiment in which abused or neglected children are randomly assigned to stay home or go to foster care. In marginal (lower-risk) cases where the decision to remove a child depends on the investigator assigned to the case, studies have been done using the best available methods (which are not very satisfactory) and different studies have reached different conclusions.1 These methods cannot be used to estimate the effects of foster care for children who are at higher risk, whom investigators would tend to agree should be removed. But in these cases, it is highly plausible that foster care is likely to do more good than harm. It is impossible to know the risks facing the particular child discussed in this column because we have no idea what a visit to the child’s home would reveal.
A big problem is that C.P.S. [Child Protective Services]’s most powerful instrument is family separation, which can be traumatic for both children and parents. Despite efforts to reduce reliance on it, a built-in asymmetry of blame can lead to overuse. Headlines and public outrage can ensue when a caseworker makes a judgment that leaves a child in a dangerous situation; there’s seldom much notice when a caseworker makes a judgment that unnecessarily separates a family. As one social-policy expert has put it, this imbalance of incentives means that those in the child-protection sector aren’t so much “risk averse” as “risk-to-self averse.”
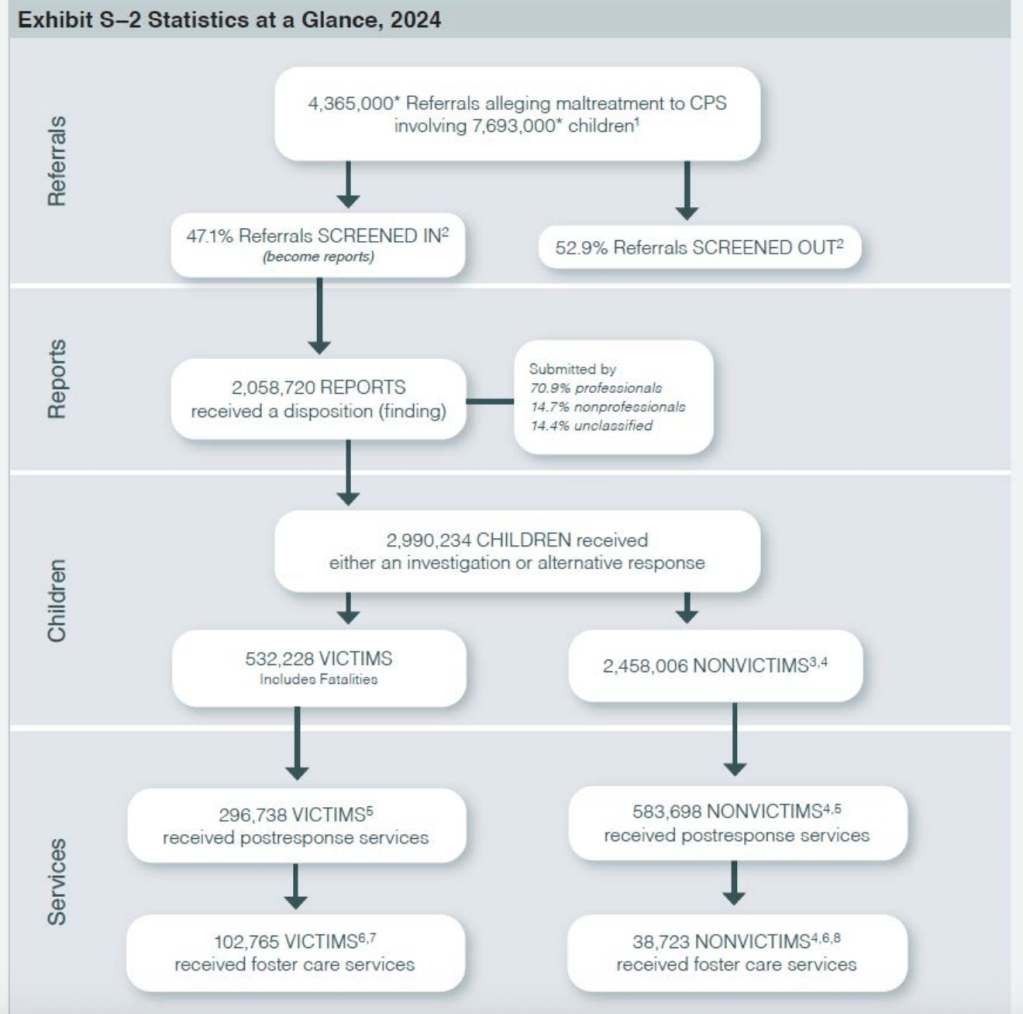
Appiah is right that CPS’ “most powerful” instrument is family separation, but it is not the most common response to a report or abuse or neglect. First, the report must be screened in to receive an investigation or an alternative esponse. Based on the latest data compiled by the federal government from state submissions, about 4.365 million reports involving 7.693 million children were made to CPS in 2024. Less than half of the calls were screened in for an investigation or an “alternative response” (often called a family assessment) which is a process often used for lower-risk cases and is designed to focus on a family’s service needs rather than determining whether maltreatment occurred. About three million (2,990,234) children received either an investigation or an alternative response. If the social worker doing the investigation or assessment decides that the child cannot be safely maintained at home, that child will likely be placed in foster care. But in cases where maltreatment is found but the child is not deemed to be in imminent danger, it is more likely that the family will receive case management and services (such as parenting education, drug treatment, and mental health services) through the opening of an in-home case.
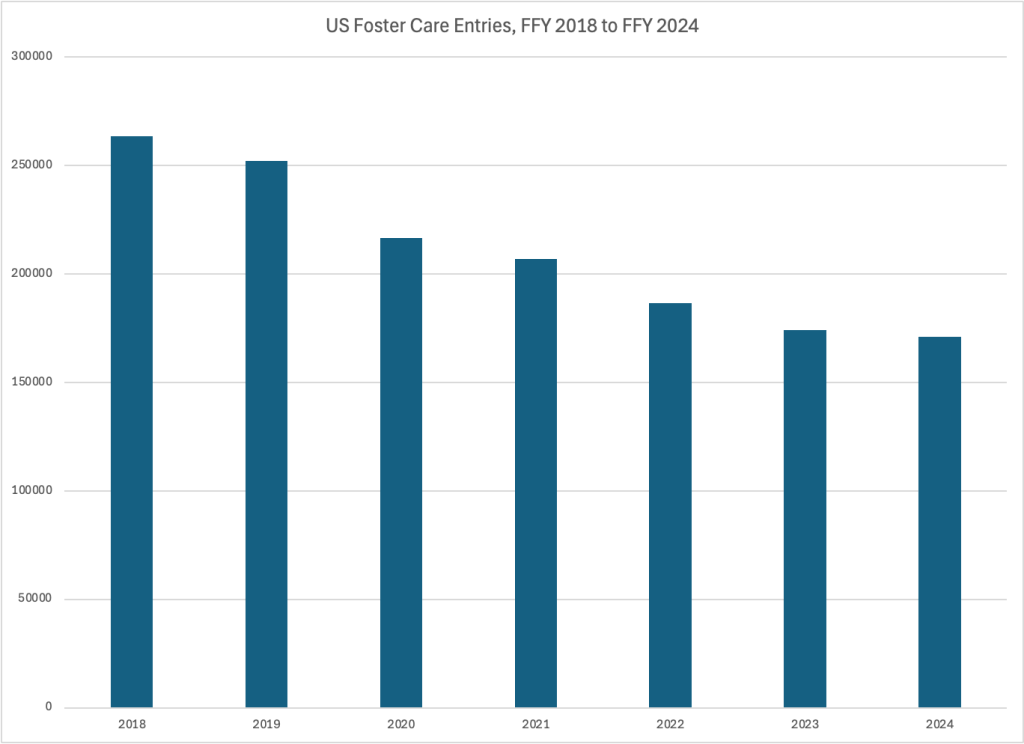
The total number of children placed in foster care in FFY 2024 was 170,955, which is less than six percent of the three million children who received an investigation or alternative response, and barely two percent of the children who were the subject of a call to CPS. Unfortunately we do not know how many children receive in-home services because the Children’s Bureau does not collect that data.2 But clearly the number placed in foster care is small relative to the number of children who are the subject of calls and the number who are investigated.
Appiah seems to be living in another world when he says that “Headlines and public outrage can ensue when a caseworker makes a judgment that leaves a child in a dangerous situation;….. this imbalance of incentives means that those in the child-protection sector aren’t so much “risk averse” as “risk-to-self averse.” That may be the case, but the national conversation in child welfare for at least ten years has been all about keeping families together and kids out of foster care. Every day brings a new report of a child being left in an obviously dangerous home and ultimately dying. Right now, we may have to worry more about children being left in dangerous homes than about them being unnecessarily removed.
When people talk as if all that matters is the “best interests of the child,” they turn an important idea into a simplifying rule. It isn’t as if we believe that billionaires are entitled to take the babies of low-income parents on the grounds that they can promise better life chances. The harm done to parents, along with the harm done to children by tearing their families apart, has to figure into any proper moral accounting.
Here, Appiah has created a straw man. Nobody is saying that children should be removed when they could have a better life in a different family or that the best interests of the child is grounds for removal. Harm to parents? Yes, parents are harmed by the removal of their children. But when the parents have been severely abusing or neglecting their child, I don’t think their well-being should enter into the equation at all.
All of that brings us back to your position in this episode. As you say, you don’t really know much about this situation, and your letter indicates a certain class distance that may add to your uncertainty. What you witnessed was worrisome, but you did not see someone shivering or sick. Nor do you live in the community. Others in the store, townspeople, saw the child, too. The child presumably has neighbors who see the preschooler’s everyday life, and any of them could have reported what they knew (and, for all you know, have done so). They may know the local record of C.P.S. and have a keener sense than you of both the risk to the child and the risk of calling in the state. So you shouldn’t reproach yourself for not reporting this child. That’s not because C.P.S. couldn’t possibly have helped. It’s because you didn’t know enough to decide what was needed and there were others better placed to do so.
A child who is wearing shorts and a tee shirt and no socks, shoes or coat in cold weather is clearly neglected, and some kind of intervention is necessary. But Appiah’s point about residents of the community being in a better position to report is a good one. This child is clearly not being hidden away, so others in the community probably have a better sense of what is going on than a stranger observing this group for the first time. Can one be sure that this child goes to school or is regularly exposed to people in the community who would be inclined to report? Based on my ignorance about the answer to this question, I would probably call CPS, despite my doubts about whether the call would be accepted given that only a license plate could be provided to identify the child and family.
The Ethicist’s final conclusion that the anonymous writer should not reproach herself for not calling CPS about this child is reasonable. But that conclusion stems from the writer’s position as a stranger in the community and is not applicable to the more common scenario in which a potential reporter has longer-term knowledge about a child’s circumstances. What is more important is that the three preceding paragraphs contain misinformation that may discourage people from reporting in situations when they really should do so. It is unfortunate that The Ethicist has fallen victim to the current ideological climate, where right and left agree in opposing government interference in the lives of children, even those who are abused or neglected.
Notes
Joseph Doyle of MIT, in a pathbreaking study, found a way to simulate such an experiment by taking advantage of the fact that children are essentially randomly assigned to different investigators who have different propensities to place children in foster care. Treating assignment to an investigator as an “instrumental variable,” Doyle was able to estimate the effects of foster care in marginal cases, where the assignment of an investigator determines whether the child will be placed in foster care. His results, using data from Illinois, suggested that “children on the margins of placement tend to have better outcomes when they remain at home.” But Doyle’s data are over two decades old and from a state with an atypical foster care system. Use of the same method with data from Michigan, Gross and Baron found that assignment to foster care for children at the margin of placement improved children’s safety and educational outcomes and in the long-term reduced the chances of adult arrests, convictions and incarceration. A similar study in Rhode Island found that found that removal significantly increased test scores and reduced grade repetition for girls and had not discernible impacts for boys. ↩︎
In its Child Maltreatment reports, the Children’s Bureau provides an estimate of the number of children reported to CPS and how many of those children ultimately end up receiving “postresponse services,” which includes both foster care and in-home services. Unfortunately, the numbers are duplicated, so that the same child can be counted more than once if that child is the subject of a new report after leaving foster care or having an in-home case closed. Moreover, the concept of “postresponse services” is quite broad and includes very limited services, such as information and referral, that may not require the opening of a case. ↩︎
In Home Visiting: More Hype than Hope, I wrote about the failure of decades of studies to prove that home visiting programs have real-life outcomes for children and families. In this post, I explain how the federal government promotes these and other programs as interventions to prevent foster care despite the lack of meaningful evidence for their success. A “Prevention Services Clearinghouse” established by federal legislation approves programs for reimbursement based on the results of outcome studies, with virtually no attention to the quality of the measures used, the lack of corroboration, the total weight of the evidence, or the logic and size of the impacts. There is little evidence to support the effectiveness of these programs in making it possible for children who are maltreated (or at risk of foster care for another reason) to remain safely in their homes. Congress should consider eliminating the Clearinghouse and changing the type of services services eligible for federal funding.
The stated purpose of the Family FIrst Prevention Services Act (FFPSA),1 which was signed by President Trump in 2018, was to “provide enhanced support to children and families and prevent foster care placements through the provision of mental health and substance abuse prevention and treatment services, in-home parent skill-based programs, and kinship navigator services.” To achieve this purpose, FFPSA expanded the use of Title IV-E funds from foster care and adoption to what it called “foster care prevention services and programs” designed to prevent the removal of children from their homes.2 These programs were nothing new; at the state level, they are often called in-home services, family preservation services, or intact family services. Under FFPSA, these services are available to children who are “candidates for foster care” [meaning the child is at imminent risk of entering foster care but can safely remain at home or with a relative with the provision of services provided under the Act3] and to pregnant or parenting foster youth and the parents or kin caregivers of these children.4
Under FFPSA, these “foster care prevention services” must be provided “in accordance with practices that meet the requirements for being promising, supported, or well-supported practices.” Among the requirements, the components of the practice must be described in a book or manual, there must be no evidence suggesting the program does more harm than good, and when there are multiple studies of one program, the “overall weight of the evidence” must support the benefits of the practice. Each practice must be found to be “superior to an appropriate comparison practice using conventional standards of statistical significance in terms of demonstrated meaningful improvements in validated measures of important child and parent outcomes, such as mental health, substance abuse, and child safety and well-being.”
To receive the highest rating of “well-supported,” a practice must have data from at least two randomized controlled trials (RCT’s), or quasi-experimental research designs if RCT’s are not available. At least one of the studies must demonstrate that the practice has a sustained effect lasting at least a year. The requirements are somewhat lower to be a “supported” practice and lower still to be a “promising” practice. In order for a program to be rated as “supported” or “well-supported,” the supporting studies must have been conducted in a “usual care or practice” setting, which is defined as an existing service provider that delivers substance abuse, mental health, parenting or kinship navigator services as part of its typical operations.
In order to further define the requirements and apply them to existing programs, FFPSA created the Title IV-E Prevention Services Clearinghouse (“the Clearinghouse” from now on), which is run under contract by Abt Global, formerly Abt Associates. The Clearinghouse has published a Handbook of Standards and Procedures describing the methodology it has developed to evaluate whether a program meets the requirements established by FFPSA.5 Program ratings are based on what the handbook calls “contrasts.” A contrast is defined as “a comparison of an eligible intervention condition to an eligible comparison condition on a specific outcome for a specific posttest measurement.” A “contrast” might be a comparison of the number of substantiated child abuse reports for the experimental vs the control group in one study, for example. A contrast must be statistically significant based on conventional standards in order to be considered favorable.6
The Clearinghouse staff has interpreted the requirements written by Congress in a way that sets a very low bar for a program to be judged “well-supported,” “supported,” or “promising.” To be “well-supported,” the Clearinghouse requires no more than two contrasts from different studies that show favorable effects.” At least one of the contrasts must demonstrate a “sustained favorable effect” of at least 12 months. This is a low standard for many reasons.
A program can be rated “well-supported” with as few as two positive contrasts, even if they are wildly outnumbered by contrasts that fail to show an impact. Even within a specific category (such as parental drug abuse, for example), one favorable contrast is enough, no matter how many other related indicators from the same or other studies show no effect.
Any positive contrast is counted, regardless of whether it is based on objective indicators or subjective ones like self-reports. Improvements on subjective measures are counted even if objective measures fail to find impacts.
Any pattern of impacts (or contrasts) is accepted, regardless of whether it is predicted by the program’s theory or logic model. If a program is supposed to work by changing parental behavior, but it instead changes children’s behavior directly, the outcome is counted. There is no requirement that a program impact be explained by its logic model or theory.
There is no requirement that a specific contrast reported by one study be corroborated by another study. Many of the individual impacts that are reported are supported by only one study, with each study cited providing evidence of a different impact.
Any contrast that is statistically significant is accepted, regardless of whether it is of practical significance. The American Statistical Association has stated that “[S]tatistical significance is not equivalent to scientific, human, or economic significance.” A tiny effect can be statistically significant if the sample size or measurement precision is large enough.
Studies are counted even when the specific populations studied are very different from those eligible for Title IV-E Prevention services.
Examining the Clearinghouse evidence on some of the most popular programs clearly reveals the flaws of its methodology, providing multiple examples of the problems noted above.
Parents as Teachers is the most popular program rated by the Clearinghouse, having been included by 31 states in their Title IV-E Prevention plans as of August 2024. PAT is a home visiting program that describes its mission as “To promote the optimal early development, learning and health of children by supporting and engaging their parents and caregivers.” The rating of “well-supported” was based on only three studies, one of which was not conducted in a “usual care and practice setting” and another of which was conducted in Switzerland–with a very different population from that of the U.S. The Clearinghouse found three favorable contrasts (out of six total contrasts) on child social functioning, all from one study, along with one unfavorable contrast and two showing no effect. They found two favorable contrasts on child cognitive abilities (one from the Swiss study) compared to 10 findings of no effect). And they found two small favorable contrasts on child welfare administrative reports (with two showing no effect) from a comparison group study that was not done in a “usual care or practice setting,” Only one study reviewed looked at the quality of parenting or the home environment, and it found no favorable effects. The authors of that study said that the results “raised questions about the underlying premise of PAT that focusing services on parents to improve parenting knowledge, attitudes, and behaviors is an effective way to benefit children.” They also concluded that their results (including the three positive contrasts on child social functioning and one on child cognitive functioning) “are consistent with the overall research base for family-focused early childhood programs, which have produced ‘modest and inconsistent effects.'” (ee Appendix A for more detail on all the contrasts discussed here).
Functional Family Therapy (FFT) is second in popularity only to Parents as Teachers, being included in the plans of 25 states as of August, 2024. As described by the Clearinghouse, FFT “aims to address risk and protective factors that impact the adaptive development of 11 to 18 year old youth who have been referred for behavioral or emotional problems.” The Clearinghouse rated FFT as “well-supported” based on the results of six studies. The Clearinghouse reported two favorable contrasts, 23 contrasts showing no effect, and one unfavorable contrast on Child Behavioral and Emotional Functioning–the core goal of the program. It showed two favorable contrasts, two unfavorable contrasts, and 16 contrasts showing no effect on child delinquent behavior. No contrasts showed an effect on positive parenting practices and only two out of 13 contrasts showed an favorable effect on family functioning. Ten contrasts showed a favorable impact on children’s substance abuse, compared to eight findings of no effect. But all of these favorable contrasts came from one study of alcohol-abusing youths who resided in a shelter after running away–a very specific population that may not be generalizable to children abusing other substances or those who are living at home.
Like FFT, Motivational Interviewing (MI) was included by 25 states in their Family First plans as of August 2024. MI, according to the Clearinghouse, is a” method of counseling clients designed to promote behavior change and improve physiological, psychological, and lifestyle outcomes.” The Clearinghouse reviewed studies of MI focused on illicit substance and alcohol use or abuse among youth and adults, and nicotine or tobacco use among youth under the age of 18. These programs are typically delivered in one to three sessions with each session lasting about 30 to 50 minutes. The Clearinghouse rated MI as “well-supported” based on results from 21 studies. The contrasts reviewed showed no effects on child substance use, caregiver mental health, caregiver criminal behavior, family functioning, parent/caregiver physical health, or economic and housing stability. The only favorable effects were on parent/caregiver substance abuse, for which there were sixteen favorable contrasts, two unfavorable contrasts, and 91 showing no effect. Eleven of the favorable contrasts came from one study of heavy-drinking college students–a very different population from parents of children at risk of foster care placement; presumably few if any were parents at all. It was also not conducted in a “usual care or practic setting.” It is no surprise that a program of one to three sessions would not lead to major changes in parents’ and children’s lives, but it is strange that serious analysts would accept these results as proof that such a minimal program would change lives.
The Clearinghouse rated the Healthy Families America (HFA) home visiting program (included by 22 states in their Title IV-E Prevention Plans) to be “well-supported” based on the results of six studies. Healthy Families America was developed as an intervention to prevent child maltreatment and is now the signature program of an organization called Prevent Child Abuse America, as I discussed in an earlier post. Yet, HFA’s effects on child maltreatment are decidedly underwhelming. The Clearinghouse found five positive contrasts on self-reported measures of maltreatment and no favorable contrasts on 99 more objective measures like CPS reports, hospitalizations and injuries. Of the 16 remaining favorable contrasts for the entire program, five come from improvements in parental reports of child behavioral and emotional functioning (a self-reported item with possible bias), another was on the child’s self reports about skipping school “often,” and none were corroborated by another study.
Some readers might observe that the standard critiques of the clearinghouse focus on the difficulty, not the ease, of meeting its standards. Critics like The Child Welfare League of America have stated that the “high evidentiary standards for the clearinghouse require rigorous, costly research that many states, Tribes and programs are unable to fund. This barrier is particularly onerous for programs that focus on underserved populations, such as Black and Native families, children of more than one race, and rural communities.” This assertion is not inconsistent with my conclusions about the Clearinghouse. That is because there are two types of standards. The standards for the rigor of the studies themselves may be too high for many programs to meet. But once a study meets the requirements to be reviewed, the requirements for being “well-supported” are almost laughable.
Another problem with the Clearinghouse is that many of the programs included are generally paid for by Medicaid, private insurance, or other state and federal programs, such as the federal home visiting program. And Title IV-E is required to be the payer of last resort for these services so it cannot pay if another source is available. The idea was apparently that Family First could be used to supplement these sources for families without private health insurance or where these funds are not available, but this does not seem to be occurring on a large scale, as I explain below.7
Finally, the Clearinghouse does not include what may be the most important foster care prevention service of all–case management. All of the services in the clearinghouse depend on relationships, but it is the relationship with the social worker managing the in-home case that may be the most important intervention for a maltreating parent. It is the case manager who refers the client to the parenting, substance abuse and mental health programs prescribed by the Act and who maintains contact with the programs to monitor the parent’s participation and progress. The case manager is responsible, through home visits, for monitoring the safety of the child or children who have not been placed in foster care. Without such monitoring, there can be no foster care prevention services.
Currently, case management is treated as an administrative cost under Title IV-E, which means it cannot be paid for unless the client is receiving other services that are supported by the Clearinghouse. At least one agency, the District of Columbia’s Child and Family Services Agency, has found a way to adapt one of the “well-supported practices” listed in the Clearinghouse as a case management model, allowing it to claim Title IV-E funding for case management for all children receiving foster care prevention services. CFSA adapted the practice of Motivational Interviewing (MI, discussed above), which is in the Clearinghouse as a substance abuse intervention, as a model for case management for all in-home services. As one account puts it, the approval of this use for MI was “particularly notable because while [MI] was approved by the Title IV-E Clearinghouse for Family First reimbursement only as a substance abuse service, DC received approval to implement and claim for it as an integral component of CFSA’s case management practice for all families.” But it should not be necessary for states to go through this type of charade in order to obtain Title IV-E funding for their case management services.
All of the problems mentioned above may explain why states are not drawing down large amounts of Title IV-E funding for foster care prevention programs. The federal government spent only $182 million reimbursing states for Title IV-E prevention services in FY2024, serving only about 18,300 children per month. A recent federal report showed that reported reimbursement claims on Title IV-E prevention services constituted less than two percent of overall Title IV-E program reimbursement claims in FY 2023, serving about two percent of the children receiving Title IV-E funded services.
What can be done?
Raising the standards for “promising,” “supported,” ‘well-supported” to be meaningful is simply not a viable option. Adjusting the three ratings to incorporate the quality of the measures, the need for corroboration, the weight of the evidence and the logic and size of the impacts, would probably mean that few if any programs would be classified in the top tier. So there is not really a way to classify programs based on evidence that will work well for the purpose of funding foster care prevention programs in Title IV-E.
Perhaps this is not surprising. The concept of evidence-based practice was adapted from medicine. When applied to social services, the concept has many limitations. Research conducted under controlled, small-scale, well-funded conditions, even if conducted in a “usual care and practice” setting is often not applicable to the messy, underfunded world of social services practice. It is well-known that effect sizes often shrink when a small pilot program is expanded to cover a larger population. Moreover, a study conducted on one population may not be generalizable to other groups. The population of parents at risk of losing their children to foster care is distinct from many other populations included in the studies mentioned above. The antecedents of child maltreatment, substance abuse and mental illness are extremely complex and may go back for generations. The idea that a three-session, three-month or even a three-year program can eliminate these problems may be unrealistic.
Finally, in relationship-intensive services like all of those included in the Clearinghouse, the characteristics of the practitioner probably matter more more than the specific model. In psychotherapy, multiple studies have concluded that “who your therapist is matters more than the model they use.” Ordinary people dealing with mental illness or addiction do not usually look for an “evidence-based practice.” They look for the best provider they can find–the one they have heard by word-of-mouth, or by scanning the internet for ratings. As mentioned above, the quality of the therapist matters more than the model, and the same applies to program staff. When I was a foster care social worker, and we had a child who had complex mental health needs, we used available funds to reimburse a top-notch provider who did not accept Medicaid. I don’t think we ever talked about what “model” they offered, and they met with clients for much longer than than program manuals prescribe. Medicaid itself does not require proof that a program is evidence-based.
In light of these issues, Congress should consider eliminating the Title IV-E Clearinghouse, as proposed by the Bipartisan Policy Center’s child welfare working group in its recent Blueprint for Child Welfare Financing and Accountability Reform.” The group of 15 child welfare experts representing different professional experiences and perspectives agreed that the clearinghouse process for approving programs as evidence-based “is cumbersome, is idiosyncratic, and impedes states from meeting the needs of families….” The group recommended replacing the clearinghouse with an expert panel convened by the U.S. Department of Health and Human Services that would consider proposals from the states for programs they want to provide using Title IV-E funds. States would be required to submit “evidence to support the efficacy of the interventions, and data that demonstrates the why states believe that proposed interventions would reduce child welfare involvement or improve outcomes of child welfare-involved children and families.”
Congress should also change the definition of the “prevention” services that can receive federal reimbursement under Title IV-E. Instead of continuing to pay for programs that belong to the field of mental health and substance abuse or are generally funded by Medicaid or private insurance, Title IV-E funds should be used for the critical service provided either directly or under contract by child welfare agencies–case management. Agencies should not have to go through the contortions that DC’s Child and Family Services Agency went through to adapt a three-session substance abuse cessation program into a case management model only to receive reimbursement from Title IV-E. This is the main service that they provide directly and it should be funded. Congress could also add a provision for states to be reimbursed to provide services mental health or drug treatment for the small number of parents who do not have public or private coverage for such services–in other words, where a payer of last resort is needed.
In drafting and passing FFPSA, Congress hoped to make new funds available to programs that would ameliorate the problems that were putting children at risk of being removed from their homes. In its effort to ensure that effective programs were funded, Congress instead created a process that awards ratings to programs based on the mindless and mechanical application of standards that mean little–and that fails to unlock the hoped-for source of funding for foster care prevention. The law must be changed in order to fulfill the intent of its framers.
There is something odd about the concept of services to prevent foster care. Prevention usually refers to a social problem like child maltreatment or teen pregnancy, not a government policy, which is itself a response to the problem of child maltreatment. It is like talking about preventing hospitalization rather than preventing illness. It would be more natural to think of services to prevent the underlying problem that result in foster care, which is usually child abuse or neglect, but can also be children’s behavioral health problems that are so severe that parents feel compelled to relinquish their care to the state. But this is the term used by FFPSA and I will use it here. ↩︎
A note about foster care candidacy is in order here. In general, children are placed in foster care because they are abused or neglected or are at imminent risk of abuse or neglect. However , there is another group of children entering foster care who have drawn increasing attention. These are children whose parents voluntarily relinquish them because they are unable to care for them at home or obtain needed services–usually care for severe behavioral issues. ↩︎
Federal research has estimated that as many as five percent of all children entering foster care between 2017 and 2019 may have entered care primarily to receive behavioral health or disability services, not because of maltreatment. ↩︎
The Handbook has already been revised once, but the language on this specific issue has not been revised. ↩︎
See pages 83-84 for more on statistical significance. This author did not find a statement of the required p-level. ↩︎
Also problematic is the failure to include domestic violence services in the clearinghouse. This was always puzzling. Child welfare social workers and academics often speak of the “Big Three” factors that result in child welfare involvement– drug abuse, mental illness and domestic violence. So the omission of domestic violence was strange–especially because domestic violence programs are greatly underfunded and not chargeable to an another program like Medicaid. ↩︎
Appendix
Parents as Teachers Contrasts Cited by Clearinghouse
Two small favorable contrasts from the matched comparison group study, which was not carried out in a usual care or practice setting and two contrasts showing no effect on child welfare administrative reports;
One contrast showing no effect on out-of-home placement;
Three favorable contrasts, two contrasts showing no effect and one unfavorable contrast on child social functioning;
Two small favorable contrasts and ten contrasts showing no effect on child cognitive functions and abilities;
Three contrasts showing no effect on child physical development and health;
One contrast showing no effect on adult parenting practices;
Eight contrasts showing no effect and one showing an unfavorable effect on family functioning;
Nine contrasts showing no effect and one showing an unfavorable effect on adult economic and housing stability.
Functional Family Therapy (FFT) Contrasts Cited by Clearinghouse
Two favorable contrasts, 23 contrasts showing no effect, and one unfavorable contrast on Child Behavioral and Emotional Functioning–the core goal of the program. One of the two favorable contrasts is on “Strengths and Needs Assessment: Child Behavioral/Emotional Needs” immediately after completing the program. But another study shows no impact on the same outcome.
Two favorable contrasts, two unfavorable contrasts, and 16 contrasts showing no effect on chid delinquent behavior;
Nine contrasts showing no effect on positive parenting practices;
Two favorable contrasts and 13 contrasts showing no effect on family functioning.
Ten contrasts showing a favorable impact compared to only eight showing no effect on children’s substance abuse. But all of these effects came from one study of alcohol-abusing youths who resided in a shelter after running away–a very specific population that may not be generalizable to children who are living at home.
Motivational Interviewing (MI) Contrasts Cited by Clearinghouse
Thirteen contrasts showing no effects on child substance use;
Five contrasts showing no effect on caregiver mental health;
Sixteen contrasts showing a favorable effect, 91 showing no effect, and two showing an unfavorable effect on parent/caregiver substance use. Among the favorable contrasts, one study shows a favorable effect on the number of drinks per week while there is no effect on the number of drinks per day but the Clearinghouse did not apparently take account of such contradictions.
Seven contrasts showing no effect on parent/caregiver criminal behavior;
One contrast showing no effect on family functioning;
Ten contrasts showing no effect on parent-caregiver physical health;
One contrast showing no effect on economic and housing stability.
Healthy Families America (HFA) Contrasts Cited by Clearinghouse
Forty-three contrasts showing no effect on child safety as measured by child welfare administrative reports, medical indicators of maltreatment risk, or “maltreatment risk assessment” measures.
Five favorable contrasts, 38 contrasts showing no impact, and one showing a negative impact on child safety based on parental self-reports of maltreatment. Clearly these self-reports are less valid than more objective measures, since parents clearly know what answers are expected after having been through the program. A parent’s negative answer to the question of whether she ever used physical abuse in the past year (one of the actual indicators used) cannot be trusted to be accurate.
Seven contrasts showing no effect on child safety as measured by “medical indicators of maltreatment risk,” a strange heading for a group of questions from the Adolescent-Adult Parenting Inventory including “Inappropriate Expectations, Lack of Empathy, and “Belief in Corporal Punishment.”
Eleven contrasts showing no effect on “Maltreatment Risk Assessment” measures such as hospitalizations and injuries needing medical care.
Five favorable contrasts and two showing no effect on parent reports of child behavioral and emotional functioning, also a self-reported item;
Two favorable contrasts, six showing no effect, and one unfavorable contrast on child cognitive functions and abilities.
One favorable contrast on “child delinquent behavior;” The measure was actually “child skips school often,” self-reported by children in first or second grade, according to the study.
One favorable contrast and two showing no effect on child educational achievement and attainment. This was a positive contrast on the percentage of children retained in first grade. However, the percentage of children who performed above or below grad level did not change.
Three favorable contrasts and 24 showing no effect on positive parenting practices. The three favorable contrasts came from observations of “Positive Parenting” from researchers’ observations of parents during a puzzle task, a “delay of gratification” task, and a cleanup task. However observations of harsh parenting during those same tasks did not show a statistically significant change.
Three contrasts showing a favorable impact and 16 contrasts showing no effect on parent/caregiver mental or emotional health;
Fifteen contrasts showing no effect on parent/caregiver substance use;
Three contrasts showing a favorable effect and 28 contrasts showing no effect on family functioning. Twenty-two of the contrasts were measures of intimate partner violence (IPV) or family violencefrom one study only and not corroborated. The positive impacts were on three specific measures based on the perpetrator, the type of violence and the age of the child. Only three of those 30 contrasts showed a positive impact and no effect sizes were provided.
Five contrasts showing no effect on economic and housing stability.
Maltreatment Reports, Victims and Fatalities All Down in 2024, reported The Imprint upon the release of the new federal report, on child maltreatment data for Federal Fiscal Year 2024. In my last post, I showed how the child fatality numbers from that report are too flawed to allow a conclusion that child deaths decreased. Five states account for over 100 percent of the decline in child maltreatment fatalities reported by the states for FFY 2024. All of these states have acknowledged that the declines in fatalities that they reported for FFY 2024 reflected changes and errors in how child maltreatment deaths were counted, not real trends in child maltreatment fatalities. But could it be that the number of reports and child maltreatment victims are more accurate than the fatality counts, which are based on smaller and more unstable numbers? The evidence suggests that these declines are also too heavily influenced by state policy and practice changes to be taken as true indicators of actual maltreatment trends.
The annual Child Maltreatment reports, produced by the Children’s Bureau of the US Department of Health and Human Services, are based on data that states submit to the National Child Abuse and Neglect (NCANDS) data system. The new report, Child Maltreatment 2024 (CM2024), provides data for Federal Fiscal Year (FFY) 2024, which ended on September 30, 2025. Exhibit S-2 summarizes the findings of the newest report. Child welfare systems operate somewhat like a funnel, at each stage selecting a fraction of the cases or children to proceed to the next stage.. Child welfare agencies received 4.365 million “referrals” alleging maltreatment and “screened in” 47.1 percent of them as “reports,” of which 2,058,720 reports received an investigation or alternative response. The investigations resulted in a total of 532,228 children determined to be victims of child abuse and neglect.1
In discussing each stage of the child protective services process, CM2024 follows the regular practice in these reports of showing the changes in key indicators over time for the five years leading up to and including FFY 2024. But 2020-2024 is an unfortunate period to feature, given the onset of the COVID-19 pandemic in 2020. A more thoughtful approach would have been to start from 2019 or an earlier year before the onset of the pandemic. That approach would allow the observation of trends before they were interrupted by the pandemic. To facilitate such observation, I have provided charts of the changes in key indicators between 2015 and 2024, using the five-year trend data provided in CM 2019 and CM 2024.
Referrals
NCANDS uses the term “referrals” to mean reports to child welfare agencies alleging maltreatment. According to CM 2024, child welfare agencies received an estimated total of 4,365,000 referrals, or 59.3 referrals per 1,000 children, through their child abuse hotlines or central registries in that year. The number is an estimate because the states do not provide data on the total number of referrals, only on the number that were screened in and (usually) the number that were screened out. But not all states are able to provide the number of screened-out referrals; there were five jurisdictions that were not able to do this in FFY 2023 and FFY 2024, and more in earlier years.2 To estimate the total number of referrals nationally, the Children’s Bureau imputes numbers for the nonresponding states based on the national referral rate for the responding states.3
A state’s referral rate depends on what referrals it actually counts. The state-by-state tables for 2024 document large differences in referral rates, from 19.2 per 1,000 children in Hawaii to 169.1 per 1,000 in Vermont–also the top and bottom states in 2023. Vermont’s Department of Children and Families reports that the state is unique because its juvenile justice system is integrated with its child welfare system; The hotline handles calls about juvenile delinquency, truancy and other non-maltreatment concerns, helping to account for its high number of referrals.4 Connecticut reports that none of the calls that are assigned to alternative response are included in NCANDS, resulting in a lower number of rererrals than many states report. Hawaii does not submit commentary so reasons for its very low referral rate are unknown.
As shown in Chart 1, the total referral rate had been increasing until the onset of the pandemic in 2020, when it fell sharply; it then rose only slightly in 2021. It increased for the next two years, almost reaching its pre-pandemic level in 2023. In FFY 2024, the estimated number of referrals decreased slightly from 4.380 million to 4.365 million, and the referral rate decreased from 59.4 to 59.3 per 1,000 children.
Source: Child Maltreatment 2019 and Child Maltreatment 2024, Exhibit S-1.
The very small decrease in the referral rate between 2023 and 2024 could have been caused by changes in policy, practice, and the types of messaging coming fom child welfare agencies, state officials and advocates around mandatory reporting of child abuse and neglect. State legislators, agency heads and advocates have recently worked to discourage calls to their child abuse hotlines based on the prevailing belief that many of these calls do not concern maltreatment but rather poverty and are often influenced by bias against parents of color. Agencies have been revising their mandatory reporter training5 to discourage reporting of concerns that are allegedly about poverty rather than child abuse or neglect. Implicit bias training is often included based on the belief that mandatory reporters are influenced by racial, cultural and class bias. In some states, “warmlines” are being set up to accept calls that are allegedly related to poverty rather than child maltreatment.6 Some states have banned anonymous reports to child abuse hotlines on the grounds that such reports are frivolous and expose children and families to unnecessary trauma–an assertion that has been challenged by based on research showing that anonymous reports save children’s lives. Such bans passed by the legislatures in Texas and Arkansas took effect shortly before the beginning of FFY 2024. In Texas, the number of referrals fell from 249,283 in 2023 to 233,112 in 2024. In Arkansas, it fell from 63,732 to 57,371. (A ban on anonymous reporting has been signed by the Governor of New York State and will take effect next summer; we may see its effect in the following fiscal year.)
Once a state agency receives a referral, it will be “screened in” or “screened out” by agency staff. In general, referrals are screened out if they are deemed not to contain an allegation of child abuse or neglect, contain too little information on which to act, are more appropriately assigned to another agency, or for some other reason do not fall under the mandate of the child welfare agency. In NCANDS, a referral becomes a “report” once it is screened in. “Reports” are assigned for an investigation or “alternative response.”
The Children’s Bureau, as it does every year, chooses to show screened-in referrals divided by the child population, calling the result the National Screened-In Referrals Rate. This is an ambiguous indicator that reflects both the number of referrals and the proportion of those that are screened in. It is more useful to look at the percentage of referrals that an agency decides to screen in, which is an indicator of its willingness to intervene with families to protect children. Unfortunately, the the lack of screened-out numbers from some states makes this number an estimate because the total number of referrals in those states is unknown.7 Nevertheless, a clear pattern emerges when the percentage of referrals that were screened in between 2015 and 2024 is plotted in Chart 2. That percentage has decreased every year since 2015, especially after 2017, with the decline continuing during and after the pandemic. Between 2017 and 2024, the percentage of referrals that were screened in dropped from 57.6 to 47.1.
Source: Author’s Calculations from Child Matlreatment 2015, Child Maltreatment 2016, Child Maltreatment 2017, Child Maltreatment 2018, Child Maltreatment 2019, and Child Maltreatment 2024. These numbers are based on screened-out referral rates for 44 states in FFY 2015, 45 states in 2016, 2017, 2018, and 2019, 47 states in 2020 and 2022, and 46 states in 2021 and 2023. The states that did not report screened-out referrals in all ten years include New Jersey, New York, Pennsylvania, and North Dakota.
Some states with larger decreases in the number of screened-in referrals attributed them in their commentaries to more consistent screening processes with the implementation of centralized intake, more structured processes for determining if a report meets criteria for acceptance, or new screening tools such as a Structured Decision-Making model. Nebraska reports that in July 2023 it dropped a policy that was implemented in June 2019 that required the acceptance of all reports made by medical professionals about a child aged five or under. The state reports a modest decline in the number of screened-in referrals in the following year. Considering changes in the prevailing child welfare climate mentioned above, it is likely that other states made policy or practice changes designed to reduce the number of reports that were screened in.
National Child Disposition Rate
An informative rate reported by the Children’s Bureau is the “national child disposition rate,” which is the number of children subject to an investigation or alternative response. This rate is a good measure of the “footprint” of CPS–what proportion of children it touches. This rate ranges from 12.0 per 1,000 children in Hawaii (the lowest again) to a high of 90.4 per 1,000 in West Virginia–nearly one out of every ten children. The West Virginia rate, which has fallen significantly from the high of 148.8 in FFY 2019k presumably reflects the state’s substance abuse (particularly opioid) epidemic.
The National Child Disposition Rate rose from 2015 to 2019, falling drastically with the pandemic in 2020 and again 2021. In 2022 it was back to the 2020 level of 40.1 per 1,000 children, but then began declining. The pandemic may have masked what would have been an annual decline in this rate every year between 2018 and 2024. The proportion of children touched by CPS has dropped significantly since its high of 47.8 per 1,000 in 2018 to 40.6 in 2024. Given the lack of a decrease in referrals during that time period except for the very small decrease in 2024, this pattern must reflect the drop in the proportion of reports that were screened in over the period.
“Victimization”
Once a referral is assigned for investigation or alternative response, the next phase in the funnel is the determination of whether abuse or neglect has occurred, or in NCANDS parlance, whether the child is a “victim.” A “victim” is defined as “a child for whom the state determined at least one allegation of maltreatment was substantiated or indicated8; and a disposition of substantiated or indicated was assigned for a child in a report.” “Victims” include children who died of abuse or neglect if the maltreatment was verified. Those children who receive an “alternative response”9 instead of an investigation are not counted as victims because alternative response does not result in substantiation or “indication” of a report. The Children’s Bureau somewhat tautologically treats “alternative response” as one of the possible dispositions for children assigned to an investigation or alternative response.
As I explain every year (with apologies to my faithful readers), the number of “victims” reported by states does not represent the true number of children who experienced abuse or neglect, which is unknown. Many cases of child maltreatment go unreported. Children assigned to alternative response are not found to be victims unless their case is reassigned to the investigation track. And finally, substantiation may not be an accurate reflection of whether maltreatment occurred. Making a determination of whether maltreatment occurred is difficult. Adults and children do not always tell the truth, the youngest children are nonverbal or not sufficiently articulate to answer the relevant questions. So it is not surprising that research suggests that substantiation decisions are inaccurate10 and a report to the hotline predicts future maltreatment reports and developmental outcomes almost as well as a substantiated report.11
The vast difference in state “victimization rates” illustrates how these rates may reflect agency policy and practices as well as underlying rates of abuse and neglect. These rates range from a low of 1.2 per 1,000 children in New Jersey (even lower than Hawaii and even lower than last year’s rate of 1.5) to a high of 15.4 in Maine. It is unlikely that Maine has more than ten times more child abuse and neglect victims than New Jersey. “”Victimization rates” reflect what happens at earlier stages in the funnel of child welfare–reports, screening, and the use of alternative response to divert a child from the investigative track. They also reflect policies including different definitions of abuse or neglect and levels of evidence required to confirm maltreatment. They also state idiosyncracies in state systems: referrals concerning less serious neglect that are routed to General Protective Services in Pennsylvania do not appear at all in NCANDS. In Calendar Year 2024, the Pennsylvania Department of Human Services received 176,496 General Protective Services reports and only 41,070 Child Protective Services reports, so the overwhelming majority of referrals in Pennsylvania are not included in NCANDS In view of the deceptiveness of these terms, I have put the terms “victims” and “victimization rates,” when not qualified, in quotation marks in this post.
But what about changes over time? The fact that “victimization rates” reflect different policies and practices does not mean that trends over time don’t reflect real changes in the incidence of abuse and neglect. The national “victimization rate” declined in 2024 as it has done every year since 2018, even after the pandemic. It was down to 7.2 per 1,000 children in FFY 2024, compared to 9.2 per 1,000 children in 2018. Couldn’t this be good news about a decline in child abuse and neglect?
Victimization rates depend on screening decisions, and investigators’ decisions about whether a screened-in report will be substantiated as abuse or neglect. And these things can change over time. As mentioned above, recent changes have reflected the increasing prevalence of an ideology professing that child welfare involvement does more harm than good to children and families, and that agencies should scale back child removals into foster care and perhaps even in-home services. One way to do this is to make it more difficult to substantiate maltreatment, as New York and Texas (two states on the opposite ends of the political spectrum) have recently done. In Texas, the Legislature changed the definition of neglect to require both “blatant disregard” for the consequences of a parent’s action or inaction and either a “resulting harm or immediate danger.” New York changed the level of evidence required to substantiate an allegation of abuse or neglect from “some credible evidence” to “a fair preponderance of the evidence.” Both of these states mention these changes in explaining their declines in “victimization” counts.
Surprisingly, plotting the number of children who received an investigation or alternative response by disposition (see Table 1) casts some doubt on opinion of states like New York and Texas that the decreased number of victims they found reflects state policies making it more difficult to substantiate maltreatment. The proportion of children judged to be victims of abuse or neglect dropped from 16.8 percent in 2018 to 15.8 percent in 2024. Yet the percentage of children who received a disposition of “unsubstantiated” hardly changed during the period, nor did the proportion of children receiving an alternative response. The only category that increased enough to account for the decrease in substantiations was a category called “no alleged maltreatment,” which increased from 10.4 to 11.8 percent of the children. According to CM 202412 that category would include children who are not the subject of an allegation but who are investigated because they live in a state that provides a response to all children in a family, even those who are not the subject of an allegation. It is not clear why the percentage of children in this category would have increased so much since 2018.
Table 1 Children who Received an Investigation or Alternative Response by Disposition (Percentage), FFY 2018-2024
The number and rate of child maltreatment referrals registered by states saw a small decline in Federal Fiscal Year 2024. This decline may reflect changed messaging from states regarding mandatory reporting of child maltreatment as much or more than a real reduction in concerns regarding children being maltreated. States report a declining number of child maltreatment victims as well, but it is not possible to say with any confidence that the number of victims and their proportion of the population decreased in FFY 2024 or in the past five or ten years. There are simply too many factors influencing these numbers and how they change over time, including recent changes in policy and practice by state child welfare agencies designed to reduce their intervention with families. Adding to the confusion is the existence of unexplained changes, such as the reduction in the percentage of children who received an investigation or alternative response with “no alleged maltreatment.” Sadly, Child Maltreatment 2024, like its predecessors, tells us little about the true state of maltreatment in America.
Note: This blog was edited on February 17, 2024 to incorporate information about the disposition category of “no alleged maltreatment” and also to add a mention of Pennslvania’s General Protective Services cases not being included in CM 2024. It was modified again on February 19, 2024 to add information provided by the Vermont Department of Children and Families about why it receives such a high number of referrals.
Notes
Of those victims, 296,738 received some type of services, which are not discussed in this blog. ↩︎
I use the term “states” to mean “jurisdictions,” including the District of Columbia and Puerto Rico. Four states were unable to report complete data for both FFY 2023 and FFY 2024: New Jersey, New York, North Dakota and Pennsylvania. West Virginia did not report complete data for FFY 2023 so its data could also not be used for a year-to-year comparison. ↩︎
Substantated is defined as “supported or founded by state law or policy.” “Indicated” is a less commonly used term meaning a “disposition that concludes maltreatment could not be substantiated understate law or policy, but there is a reason to suspect that at least one child may have been maltreated or is at risk of maltreatment.” ↩︎
An “alternative response” includes an assessment and referral to appropriate services if the parent agrees to participate. There is no determination on whether abuse or neglect occurred and no child removal unless the case is transferred to the investigative track. ↩︎
Theodore Cross and Cecilia Casanueva, “Caseworker Judgments and Substantiation,” Child Maltreatment, 14, 1 (2009): 38-52; Desmond K. Runyan et al, “Describing Maltreatment: Do child protective services reports and research definitions agree?” Child Abuse and Neglect 29 (2005): 461-477; Brett Drake, “Unraveling ‘Unsubstantiated,’” Child Maltreatment, August 1996; and Amy M. Smith Slep and Richard E. Heyman, “Creating and Field-Testing Child Maltreatment Definitions: Improving the Reliability of Substantiation Determinations,” Child Maltreatment, 11, 3 (August 2006): 217-236. ↩︎
Brett Drake, Melissa Jonson-Reid, Ineke Wy and Silke Chung, “Substantiation and Recidivism,” Child Maltreatment 8,4 (2003): 248-260; Jon M. Hussey et al., “Defining maltreatment according to substantiation: Distinction without a difference?” Child Abuse and Neglect 29 (2005): 479-492; Patricia L. Kohl, Melissa Jonson-Reid, and Brett Drake, “Time to Leave Substantiation Behind: Findings from a National Probability Study,” Child Maltreatment, 14 (2009), 17-26; Jeffrey Leiter, Kristen A. Myers, and Matthew T. Zingraff, “Substantiated and unsubstantiated cases of child maltreatment: do their consequences differ?” Social Work Research 18 (1994): 67-82; and Diana J. English et al, “Causes and Consequences of the Substantiation Decision in Washington State Child Protective Services,” Children and Youth Services Review, 24, 11 (2002): 817-851 ↩︎
This post was originally published on Lives Cut Short website.
The Children’s Bureau’s eagerly awaited Child Maltreatment report has been published and the child welfare newsletter The Imprint lost no time in announcing that Maltreatment Reports, Victims and Fatalities All Down in 2024. Others are sure to follow with commentaries celebrating a 10 percent drop in the number of child maltreatment fatalities. This would be great news if it were true, but making any conclusion based on these data is not warranted. The state-by-state data show that the reductions reflect changing policies and practices, as well as reporting problems, rather than actual reductions in child maltreatment deaths.
On January 8, 2025, the Administration on Children and Families (ACF) of the U.S. Department of Health and Human Services published Child Maltreatment 2024 (CM2024), its latest compendium of data on states’ responses to reports of child abuse and neglect. These annual publications, produced by the Children’s Bureau of ACF, are based on data that states submit to the National Child Abuse and Neglect (NCANDS) data system. CM2024 provides data for FFY 2024, which ended on September 30, 2024. Based on reports from all 50 states, the District of Columbia, and Puerto Rico, CM 2024 reports that the number of child maltreatment fatalities dropped from 1,979 or 2.68 per 1,000 children in Federal Fiscal Year (FFY) 2023 to 1,773 or 2.41 per 1,000 children in FFY 2024. Of course,we should celebrate if these numbers are believable. But that is not the case.
An analysis of last year’s Child Maltreatment report explained how the numbers in the annual federal reports cannot be taken as a good estimate of child maltreatment deaths for any given year. It is widely accepted that these numbers greatly understate the actual number of deaths due to child abuse or neglect. Well-functioning child death review teams identify many more child maltreatment fatalities than are reported to NCANDS. Based on only publicly available sources, Lives Cut Short has counted more child maltreatment deaths than those reported to NCANDS in more than half of states in either 2022 or 2023. The undercounts in NCANDS are due to a variety of state policies and practices including restrictive definitions of child maltreatment fatalities, failure to consult all available sources, restrictions on which reports are investigated, and constraints on finding maltreatment in fatality investigations.
Of course it is theoretically possible that while NCANDS underestimates child maltreatment deaths, the trends it finds over time are still valid. But state-by-state data clearly disprove that thesis. The 50 states, the District of Columbia and Puerto Rico reported 206 fewer child maltreatment deaths in FFY 2024 than in FFY 2023. Five states–Texas, Maryland, North Carolina, Illinois and Virginia–together account for a decrease of 210 fatalities–more than 100 percent of the total decrease for the year overall. Explanations from all of these states indicate that the drops they reported reflect factors other than the actual number of child maltreatment deaths.
The number of child maltreatment deaths in Texas that were reported in Child Maltreatment 2024 fell from 187 in FFY 2023 to 107 in FFY 2024, an enormous drop. In its own annual report on child fatalities and near fatalities for FY 2024, the Texas Department of Family and Protective Services (DFPS) reports a smaller but still substantial decrease from 164 child maltreatment fatalities in state fiscal year (SFY) 2023 to 99 in SFY 2024.1 The number of investigated child fatalities fell from 690 to 587–a decline of 587, or 14.9 percent. Out of the investigated families, the number of fatalities where abuse and neglect was confirmed fell from 164 or 23.7 percent of fatalities investigated to 99, or 16.9 percent of fatalities.
In its report, DFPS suggests that the decline in both investigations and maltreatment findings reflects a change in the definition of child neglect adopted by the Legislature that took effect in FY 2022. This change required the agency to find that a parent exhibited “blatant disregard” for the consequences of an act or failure to the act that results in harm or immediate danger to a child. DFPS believes this law affected investigations and dispositions in both FY 2023 and FY 2024. (NOTE: This does not explain the drop in findings of abuse, however.)
DFPS also reported that two other factors affected the fatality numbers. Starting in 2022, the agency changed its screening policy so that reports involving a child fatality but include no explicit concern for abuse and neglect are not investigated if the reporter “or first responders” had no concern for abuse or neglect. According to DFPS, this contributed to the decrease in investigations and ultimately in fatalities reported both in FY 2023 and in FY 2024. DFPS also reported that in FY 2024 it imposed an additional level of review for certain investigations that found neglect (like those involving drowning or unsafe sleep) to ensure that the investigator had followed the new neglect definition incorporating “blatant disregard.” This change almost certainly contributed to the reduced number of maltreatment fatalities found.
North Carolina reported a large drop in child maltreatment fatalities from 107 in FFY 2023 to 46 in FFY 2024. In response to a question about the cause for this large decrease, a spokesperson for the North Carolina Department of Health and Human Services (NCHDHHS) provided the following explanation, which makes clear that the reported decline in child maltreatment fatalities in FFY 2024 is not valid and should not have been included in CM 2024:
NCDHHS is aware of probable discrepancies in the state’s historic child fatality data, particularly in 2023-2025. Prior to 2025, the state was using an outdated database platform that became increasingly unstable and subject to error. Recognizing this, NCDHHS made significant investments in designing and building a new, comprehensive Child Welfare Fatality Information System that launched for state users in 2025. While data from the old database was transferred to the new system, these numbers likely include inconsistencies and should not be used to analyze trends in child fatalities.
Maryland reported 46 child maltreatment deaths in FFY 2024, compared to 83 in FFY 2023.The large drop in Maryland’s child maltreatment fatalities was predictable in advance and is as irrelevant to actual child deaths as those in Texas and North Carolina. In 2025, Maryland’s child maltreatment fatality reports to the Children’s Bureau made the news when a reporter discovered the state had the second highest number in the country. Department of Human Services (DHS) officials soon realized that the agency had for years been reporting the number of death cases investigated for abuse and neglect, whether or not they were confirmed as due to maltreatment. Maryland reported this issue in its commentary to CM2024, stating that it had submitted correct information for 2024. However, Maryland’s entries for previous years have not been corrected, resulting in the misleading appearance of a large reduction in child maltreatment fatalities between FFY 2023 and FFY 2024.
Illinois reported a smaller but still sizable decline from 83 child maltreatment fatalities in FFY 2023 (itself a drop from 110 in FFY 2022) to 66 in FFY 2024. In its commentary, DCFS reported that the decrease in confirmed maltreatment fatalities in both years stems from the introduction of an administrative review process for sleep-related deaths. For any sleep-related death allegation, a senior administrator reviews the investigation “to ensure consistent evaluation of whether the sleep-related death included evidence of blatant disregard,” referring to the parent’s disregard of the danger to the child of unsafe sleeping arrangements. This is the same concept that is included in Texas’ new definition of child neglect. DCFS reports that this new review process has continued to result in fewer sleep-related deaths being “indicated” as due to maltreatment.
Virginia reported a significant decrease in child maltreatment fatalities from 55 in FFY 2023 to 40 in FFY 2024. In its commentary, the Virginia Department of Social Services suggests that this decline was due to a decrease in fatality investigations in FFY 2024, which in turn stemmed from “more local agencies having overdue investigations that were not closed timely or in accordance with VDSS guidance.”
The explanations provided by Texas and Illinois have something in common. In both states, the decline in confirmed child maltreatment fatalities was the intended result of policies–like a changed definition of neglect in Texas and the imposition of administrative reviews to enforce such a restrictive definition in both states–that were designed to find fewer child maltreatment fatalities. Those policies and practices are only part of an overall effort designed to reduce the involvement of child welfare agencies in the lives of families in those two states and in many other states around the country. So it is not surprising that the number of reports accepted for investigation and the number of children found to be victims of abuse or neglect also declined in FFY 2024.
In conclusion, five states account for over 100 percent of the decline in child maltreatment fatalities reported in Child Maltreatment 2024. All of these states have acknowledged that the decline in fatalities that they reported for FFY 2024 was caused by the fatality determination and reporting process itself, not real trends in child maltreatment deaths. The bottom line is that the numbers contained in the Children’s Bureau’s Child Maltreatment reports are not reliable for determining national or state-level trends in child maltreatment deaths, or in child maltreatment in general. Responsible reporters and researchers should know by now not to rely on these data, but they continue to do so, confusing the public and depriving policymakers of the information they need to make good decisions.
It is not clear why the SFY numbers are so different from the FFY numbers, as the two years overlap by 11 months, DFPS has not yet responded to a request for an explanation. ↩︎
This blog has often focused on the uncritical use of flawed research to support desired conclusions. A good example of this has now become available. The authors of a new study conclude that decreasing rates of entry into foster care are not associated with changes in mortality from child abuse and neglect. Advocates of continuing reductions in foster care or its total abolition have lost no time in sharing the results, undaunted by what should have been obvious to any knowledgeable reader. The study is too flawed by the nature of its data on child maltreatment fatalities to make any conclusions about the presence or absence of a connection between foster care reductions and changes to child maltreatment mortality.
The number of children entering foster care in the United States has fallen from 252,198 in Federal Fiscal Year (FFY) 2019 to 170,955 in FFY 2024. As computed by Frank Edwards, Kelley Fong, and Robert Apel in their new paper, foster care entry rates have decreased from 3.49 to 2.47 entries per 1000 children between 2018 and 2023, a decrease of about 29 percent. This large drop in foster care entries was in large part the result of a growing bipartisan consensus on the federal level and in red and blue states around the need to reduce or entirely terminate the use of foster care to protect children from continuing abuse or neglect.
Some child advocates and media outlets around the country have argued that the reductions in the use of foster care have gone too far. The Seattle Times Editorial Board recently told readers to “Stop dodging and face facts: More kids are dying on DCYF’s watch,” citing a 35% drop in dependency petitions to take kids into foster care since 2021 along with a 67 percent increase in child deaths and near-deaths between 2020 and 2024. A series from Texas Public Radio called When Home is the Danger suggests that a 40 percent reduction in removals of children to foster care, at the same time as in-home services were being curtailed, has resulted in more children dying as a consequence of abuse or neglect. Child advocates across the country have expressed similar fears, but there has been no good data to support or refute this claim.
Edwards, Fong and Apel say their new study shows these fears are baseless. They report that they “found no evidence of a negative association between foster care entries and child maltreatment fatalities at the population level.” They came to this conclusion by estimating the association between child maltreatment mortality rates and foster care entry rates at the state level, using state administrative data from Federal Fiscal Years 2010 to 2023. Even after controlling for variations in population disadvantage, other state features, and national temporal effects they found no association between foster care entry rates and child maltreatment mortality rates.
Advocates of continuing reductions in, or outright elimination of, foster care have been circulating the article widely, using it to counter any claim that excessive foster care reductions may be leading to child fatalities. But a cursory review shows that the study is fatally flawed and would not have been published had the peer reviewers been familiar with the sources of the data used. Four of the leading academic researchers in the field have already posted comments pointing to issues with the data and the model. These comments are summarized and explained below, along with examples from my research on child maltreatment fatality data.
Flawed Data
The Edwards study uses child maltreatment fatality data from the National Child Abuse and Neglect Data System (NCANDS) to represent child maltreatment deaths. These numbers appear in the annual Child Maltreatment reports released by the Children’s Bureau. In a report called A Jumble of Standards: How State and Federal Authorities Have Underestimated Child Maltreatment Fatalities, I summarized the results of my review of ten years of federal Child Maltreatment reports, including all the state commentaries provided in each report. My work points to multiple reasons that these numbers reported by the states should never be used in such a study.
Screening Policies
The number of child maltreatment fatalities a state will find depends first on which deaths it accepts for investigation and which ones it screens out. And when these change, the number of fatalities found will probably change. For example, some states or counties historically screened out cases where there were no other children in the home,1 because investigations were not considered necessary to protect the other children in the home. West Virginia began investigating cases with no surviving children in the home in FFY 2016. Alaska changed its policy in 2023 so that it will now investigate cases where there are no surviving children in the home, which will affect future counts. We do not know how many states may have made this or similar changes over the span covered by the Edwards paper.
Texas changed its screening policy as of September 2022 so that “reports that involve a child fatality but include no explicit concern for abuse and neglect” are not investigated until the reporter or first responders are interviewed to find out if they had any concerns for abuse or neglect. Only if they had such concerns is the report investigated. DFPS reported that as a result, the number of child fatalities it investigated decreased from 997 in FY2022 to 690 in FY2023 (a 31 percent decrease) due to this new screening policy. And the number of child maltreatment fatalities found fell from 182 to 164.
Changed screening policies can also lead to an increase in reported child maltreatment fatalities. In 2022, Maryland implemented a policy that requires local agencies to screen in sleep-related fatalities, which often involve parental substance abuse. In its commentary, the agency indicated that this was the reason it reported an increase in child deaths from 68 in FFY 2022 to 83 in FFY 2023.
Definitions
NCANDS defines a child maltreatment fatality as “the death of a child as a result of abuse or neglect because either: (a) an injury resulting from child abuse or neglect was the cause of death; or (b) abuse and/or neglect were contributing factors to the cause of death.” So a state’s definition of a maltreatment fatality depends on its definition of child abuse and neglect. And if that definition changes over time, that will affect the trend in child maltreatment fatalities reported. For example, Texas changed its definition of child neglect in 2021 to require “blatant disregard” for the consequences of an act or failure to act. Texas reported a drop of in the number of child maltreatment fatalities from 255 in 2020 to 205 in 2021 to 176 in 2022. The state has attributed that decline in reported neglect deaths to the 2021 law.
A similar decrease in reported child fatalities occurred in Illinois, where “blatant disregard” was already included in the definition of neglect but the requirement was enforced through a new administrative review process for sleep-related deaths. A senior administrator reviews the investigation to ensure that death included evidence of “blatant disregard.” In its 2023 commentary, Illinois links this new policy with a decrease of 24.6 percent in reported child fatalities in FFY 2023.
Data Sources
Experts widely agree that NCANDS underestimates the total number of child maltreatment fatalities, as Edwards et al. acknowledge. One reason is that many states do not use all of the available sources for possible child maltreatment fatalities, which include reports to child protective services, state vital statistics departments, state child death review teams, law enforcement agencies, and medical examiners or coroners. Some states have recently been broadening the sources of data they use, and such changes may have resulted in an increase in reported fatalities. For example, North Carolina originally reported only deaths that the chief medical examiner classified as “homicide” by a parent or caregiver as child maltreatment fatalities. (This does not jibe with the NCANDS definition of child maltreatment fatality, but there is no consequence applied to states who do not use it.) After the agency began to include child deaths that were substantiated as maltreatment by CPS, as well as increasing their collaboration with vital statistics and criminal justice agencies to identify maltreatment deaths, North Carolina’s reported child fatalities increased from 64 in FFY2018 to 111 in FFY2019 (a 73 percent increase).
Historically, Mississippi also reported only deaths that the chief medical examiner had classified as homicide by a parent or caregiver but in 2007 began including fatalities substantiated by CPS as due to maltreatment. In FFY 2014, Mississippi developed a Special Investigations Unit to investigate all reports of child fatality that meet criteria for investigation. Mississippi reported that the having dedicated, specialized investigators resulted in a higher count of maltreatment fatalities in that year and thereafter.2 The state also reported that public awareness campaigns to prevent deaths caused by unsafe sleep and children left in hot cars led to an increase in reporting of such fatalities, also contributing to an increase in reported deaths. The number of child maltreatment fatalities reported by Mississippi increased from 17 in FFY 2010 to 76 in FFY 2023.
Reporting Errors
In 2025, a reporter at the Baltimore Banner noticed that Maryland was reporting an alarming rate of child fatalities. With a reported 83 children dying of abuse or neglect in FFY 2023, Maryland had one of the worst child maltreatment fatality rates in the nation. Taken by surprise, state Department of Human Services officials soon realized that they had been reporting incorrect numbers for the past five years. Instead of reporting the deaths for which maltreatment was confirmed, they had been reporting all child deaths that had been investigated for maltreatment. The department now believes that there were 173 child maltreatment fatalities, not the 285 reported, between FFY’s 2020 and 2023. We do not know how many other states have been reporting erroneous numbers, given the little attention that these reports usually receive.
Time Lags
A key flaw of Edwards et al.’s analysis is the assumption that child maltreatment fatalities reported for a specific year reflect the deaths that occurred in that year. That is far from being the case. As the Children’s Bureau explained in Child Maltreatment 2023, “The child fatality count in this report reflects the federal fiscal year (FFY) in which the deaths are determined as due to maltreatment. The year in which a determination is made may be different from the year in which the child died.”3 There is similar language in reports from the previous years. States have explained in their commentaries that the actual dates the children died may have occurred as much as seven years before the year they were reported. As Sarah Font of Washington University and Emily Putnam-Hornstein of the University of North Carolina explain in their comment (posted below the article), “the Edwards et al. analysis largely models whether state foster care entry rates predict past [child maltreatment fatalities] — a nonsensical question with no bearing on whether foster care is a protective intervention. Indeed, if states respond to rising [child maltreatment fatalities] by placing more high-risk children in foster care, one would expect higher past [child maltreatment fatality] rates to be associated with higher current foster care entry rates.”
Even if the fatalities did occur in the same year as they were reported, it would not make sense to expect an increase in deaths only in the same year as a decrease in foster care, Brett Drake of Washington University raises this concern in his comment. Any maltreatment fatality resulting from a failure to remove a child will not necessarily occur in the same year. A foster care removal may save a child’s life in a subsequent year. Many of the most horrific child fatality cases involve child fatalities that could have been prevented by removal in prior years. In some of these cases, the child suffered through years of abuse or neglect before dying. But as Font and Putnam-Hornstein point out, the Edwards model attempts to correlate removal rates with past child maltreatment fatalities. And there is no way that makes sense.
Other flaws in the model
Font and Putnam-Hornstein, as well as Richard Barth of the University of Maryland, draw attention to another problem. Children under age five account for 82 percent of reported child maltreatment fatalities but less than half of foster care entries. But proportional decreases in foster care entries were largest among older children: there was a 49 percent reduction in entries of 17-year-olds versus an 18 percent reduction in infant entries. It might have been more sensible to focus on younger children only, though fixing this problem would not address all the other problems with the analysis.
Barth suggests another problem with the model. Placing a child in foster care may prevent that child dying from other causes, not just maltreatment. And indeed, we have learned that maltreatment is correlated with deaths from all causes, not just from child maltreatment. Research shows that children who have been reported for maltreatment are more likely to die of accidents in their first five years, sudden infant deaths and medical causes as infants, and suicide as teenagers. It is also obvious from my personal experience reviewing child fatalities in the District of Columbia that children who die of homicide as teenagers and young adults are likely to have a family history of child abuse and neglect reports. Child maltreatment mortality is only one type of child mortality we should care about.
It is unfortunate that so many child welfare leaders and commentators are so quick to grab hold of any research that supports their point of view without critically examining the methodology and considering whether the findings justify the claims. I hope that the peer reviewers for this study were as unfamiliar with state child maltreatment data as the study authors themselves; otherwise their motives in approving the study are suspect. As Font and Putnam Hornstein put it, “[t]he conclusions of Edwards et al. rest on a mis-specified model and deeply-flawed data; deficiencies unaddressed by the authors’ numerous sensitivity analyses.” These findings have no relevance to the discussion of whether the decline in foster care removals is putting children at risk of dying.
Notes
Some jurisdictions still do this, including the District of Columbia (as I learned from requesting child fatality information) and some counties in Ohio, as described in Child Maltreatment 2022. ↩︎
Like many statements in the CM reports, this is not exactly true. A few states (including California) do attempt to capture only the deaths that occurred in the reporting year. This involves reporting on only deaths that occurred in the reporting year and then amending the numbers in future years. See A Jumble of Standards. In their eAppendix 1, Edwards, Fong and Appel note that they include the most recent revisions into their estimates. But as I describe in A Jumble of Standards, it appears that only a few states make such revisions. ↩︎
On December 19, 2025, the Administration for Children and Families (ACF) released CFSR Technical Bulletin No. 14, the first step in its plan to replace the the existing process by which it reviews state child welfare performance with one that is less burdensome and more useful. The replacement is long overdue. But ACF’s attempt to reorganize all outcomes under one slogan–A Home for Every Child–is highly problematic. It disregards the need for larger homes for sibling groups and residential treatment for some young people. And it devalues and disincentivizes the central function of child welfare–protecting children from harm.
In an article in The Imprint called Why We Are Putting the PIP on a PIP, Alex Adams, the Assistant Secretary for ACF, explains the shortcomings of the Child and Family Services Reviews (CFSR’s), which are the periodic federal reviews of state child welfare systems to assess their performance and ensure they are in compliance with federal requirements. In 25 years, no state has been in substantial compliance with all the outcomes and systemic factors that are evaluated, and every state has been placed on a Performance Improvement Plan (PIP). Meanwhile, the administrative burden is heavy. Adams rightly states that “this is busywork–expensive, repetitive, punitive busywork–and it has not improved child or family outcomes.” I don’t think many child welfare stakeholders would disagree. It is time for the CFSR’s to be put out of their misery.
But what will replace the CFSR’s? As a first step to a solution, ACF has announced a pilot PIP process that states can opt to follow instead of the standard PIP procedure. As described in the Technical Bulletin, “this Administration is creating a pilot opportunity for states….to center their program improvement efforts around the A Home for Every Child goal.” Interestingly, the goal is not defined in the Technical Bulletin;1 the definition is found in several other places including a press release stating that “A Home for Every Child sets an ambitious goal of achieving a foster home-to-child ratio greater than 1:1 in every state. The initiative will focus on both sides of the equation — increasing the availability of safe homes through diligent recruitment, prioritizing kin, and improving retention of existing caregivers while reducing entries into foster care through effective prevention and faster pathways to permanency.” This sounds reasonable at first, but there are problems with centering program improvement planning around this goal–problems with the concept itself and with the implications of using it as an organizing principle in the assessment and improvement of child welfare performance.
A Flawed Concept
A Home for Every Child as a goal of child welfare seems to make sense on its face. To take a child into foster care when there is no place to put that child seems like folly, and a state that cannot equalize the supply and demand for foster care might need to rethink its rules about when to remove a child. But ACFs definition of that goal–one licensed home per foster child– makes no sense. Many foster homes can accommodate more than one child, and we need more larger homes to welcome sibling groups. And some young people in foster care need residential treatment before they can flourish in a foster home. For these reasons, child welfare administrators tend to use the concept of “beds” rather than “homes” when counting available placements for foster youth. What matters is not how many homes there are, but how many children can be accommodated in a placement that meets their needs. The two issues of multi-child homes and placements that are not foster homes are discussed below.
Foster homes with more than one child
As mentioned above, many if not most foster homes can accommodate more than one child. Many children come into care as part of sibling groups, and child welfare agencies hope to place as many of them together as possible. Despite their efforts, siblings are often separated in foster care for lack of homes that can accommodate them. We need more programs like Together California, a new community of 12 homes each built to house up to six siblings with full-time, professionally trained foster parents. Similar programs exist in Illinois, Florida and other states. Such homes could also be offered to relatives who are do not have room to take in larger sibling groups. The requirement of one home per child encourages states to focus on assembling as many foster homes as possible, rather than developing programs to keep sibling groups together.
Placements that are not foster homes
Secondly, A Home for Every Child should not include just foster homes. Most experts acknowledge that some children and youth need residential treatment before they can thrive in a foster home. Secretary Adams wrote in The Imprint that when the number of foster homes exceeds the number of children needing them, “[c]hildren avoid sleeping in offices or cycling through short-term rentals.” But most of the children sleeping in hotels, offices, short-term rentals, and other inappropriate placements have complex behavioral health needs and have been through many foster homes already. Media reports from California, Colorado, Hawaii, Illinois, Kentucky, Maryland, Massachusetts, Michigan, Missouri, New Mexico, North Carolina, Ohio, Oregon, Pennsylvania, Rhode Island, South Carolina, Tennessee, Texas, Washington,West Virginia, and Wisconsin document the preponderance of high-needs children among those in unlicensed, inappropriate placements.2 In Adams’ own state of Idaho, the child welfare agency under his leadership reported that short-term rentals were until recently used to “temporarily house children with complex needs.” Many of these high-needs young people need residential treatment, maybe for six months or a year, before they can live in a foster home. Otherwise, they will simply be bounced from home to home until they end up in another inappropriate placement or worse.
Unfortunately Adams gives short shrift to the need for residential treatment. He writes in The Imprint that “I saw firsthand the power of this ratio [of licensed homes to children] when I ran Idaho’s child welfare system. In just one year, Idaho increased from 74 to 104 foster homes per 100 children—eliminating emergency short-term placements, expanding kinship care, augmenting prevention services, improving licensing timeliness, reducing congregate care, lowering costs, and restoring public trust.” But the press release announcing the end of Idaho foster youth being placed in short-term rentals also credited the opening of a new 16-bed assessment center which “immediately reduced the department’s reliance on temporary housing.” The center is “designed to serve as a homelike setting for foster youth until an ideal placement in a foster home or residential treatment facility [my italics] is located.” Another such center is planned. So reducing the child-to-home ratio may have helped in closing the short-term rentals, but it certainly was not the only factor that allowed these rentals to be closed.
Moreover, Idaho is still struggling to find treatment for the youth with the most complex needs, the Idaho Press reported in October 2024, shortly before the last short-term rental closed. The article concluded that “Many of the youth require residential care for mental health, substance abuse disorder or other behavioral health issues, and there still isn’t enough of this treatment available in the state.” As of December 30, 2025, DHW reports having 173 children in “congregate care,”3 of which 32 were out of state.4 If Idaho is like most states, it is the lack of high-quality, trauma-informed residential treatment facilities, rather than foster homes, that is the main cause of the stays in inappropriate placements. The Family First Prevention Services Act defined a new option for providing such care–a Qualified Residential Treatment Program (QRTP). But based on a recent listing of residential facilities, Idaho appears to have only two QRTP’s. Having a goal like “A Home for Every Child” provides no incentive to develop the needed therapeutic placements for youth with complex needs.5
Equalizing the number of licensed homes with the number of children in foster care is an arbitrary goal that does not encourage the development of needed resources, like larger foster homes and residential treatment programs. But replacing it with a one-to-one ratio of available placement slots to youth is not a good idea either. A well-functioning system needs a sizable excess capacity, because existing vacancies may not be in the right geographical area or in the right type of placement for a child who comes into care. Moreover, many existing homes and residential treatment programs are probably substandard and should be closed.6A Home for Every Child encourages states to maximize the number of homes, regardless of quality, capacity, or the need for residential treatment.
What about safety?
The ratio of homes to children can be improved in two ways, as ACF has stated: increasing the number of foster homes or decreasing the number of children in foster care. But the latter means taking fewer children into foster care. An easy way to do this is to redefine “safety” to make it harder to find a child unsafe. It appears that states have been doing this already, driving foster care numbers down to their lowest level in years and raising concerns about children being left in unsafe conditions in states as diverse as Washington, Texas, Indiana and New Jersey. As Naomi Schaefer Riley puts it, “foster care numbers are close to record lows and there are plenty of reasons to think that states are pushing them lower and sacrificing child safety in the process. If the federal government provides them with an excuse to double down on their plans to reduce the number of kids in care, many states will jump at the chance.”
The Technical Bulletin states that A Home for Every Child “provides a unifying construct that reflects the full continuum of good practice in child welfare—from prevention and family strengthening to permanency and post-permanency support—offering a cohesive framework for aligning state efforts with what works.” “From prevention to permanency” conveniently leaves out the screening and investigation of child maltreatment reports. With A Home for Every Child as the metric, the incentive is clearly to reduce entries into foster care regardless of trends in child abuse and neglect.
Some language in the Technical Bulletin suggests that other factors can be considered outside of the child-to-home ratio. States participating in the pilot must also include in their PIP’s “wraparound measures related to safety, permanency, and child and family well-being, such as adverse placement scores.” But the next sentence is “Wraparound measures should be chosen such that they will show performance improvement in areas that are expected to lead to improvements in the ratio of homes to child.” But, again, the only way child protective services can do that is reducing foster care removals. Clearly, A Home for Every Child does not center child safety.
The leadership of ACF is to be commended for seeking to reduce the burden imposed by the Child and Family Services Reviews. But the attempt to build a new quality review around a simplistic slogan like A Home for Every Child is not adequate for such a complex and serious problem as child abuse and neglect. It ignores the needs for larger foster homes to keep siblings together and for high-quality residential placements. It also creates an incentive to reduce foster care entries regardless of safety. One hopes that the current pilot will be succeeded by a more comprehensive approach that keeps safety in the forefront and recognizes the diverse needs of foster youth.
Note: After this post was published, Dr. Sarah Font of Washington University in St. Louis reminded me of another problem with A Home for Every Child. Many states rely heavily on unlicensed relatives to care for children who need placements. These states can greatly increase their count of licensed homes simply by licensing these relatives, without actually increasing the number of available placements.
Notes
It does appear in the technical bulletin as an adverbial phrase in the following sentence: “In furthering efforts to achieve the 1:1 ratio of licensed foster homes to children in foster care, states will not be required to address every item or practice area identified in the CFSR Final Report.” ↩︎
In New York, these young people are often sent to residential programs that are not equipped to provide the level of care that they need. ↩︎
“Congregate care” is a term used, often pejoratively, to describe placements that are not foster homes. ↩︎
Email from A.J. AJ McWhorter, Public Information Officer, Office of the Director |Idaho Department of Health and Welfare, December 30, 2025. ↩︎
The Technical Bulletin does say that “The 1:1 ratio does not preclude states from pursuing placements outside of foster homes or from placing multiple children, for example, siblings, in one home but rather is intended to serve as an indicator spanning the full child welfare spectrum.” But the meaning of “intended to serve as an indicator spanning the full child welfare spectrum” is unclear. Placements outside of foster homes, or of more than one children in one home, do not count toward the goal of A Home for Every Child as defined by ACF. ↩︎
This statement is based on my own personal experience in the District of Columbia and Maryland as well as personal accounts from youth around the country and media reports of abuse and neglect in foster care. ↩︎