Complete Fiscal Year 2024 data now on the Dashboard of the District of Columbia’s Child and Family Services Agency (CFSA) reveal significant changes over the previous fiscal year. Most striking is a large jump in the number of incomplete investigations and a concomitant decline in “substantiated” and “unfounded” reports. The number of children entering foster care increased for the first time in over ten years. There was a drop in in-home case openings but a similar increase in foster care placements during the year. The agency did not respond to this writer’s questions about the meaning of these trends.
Referrals
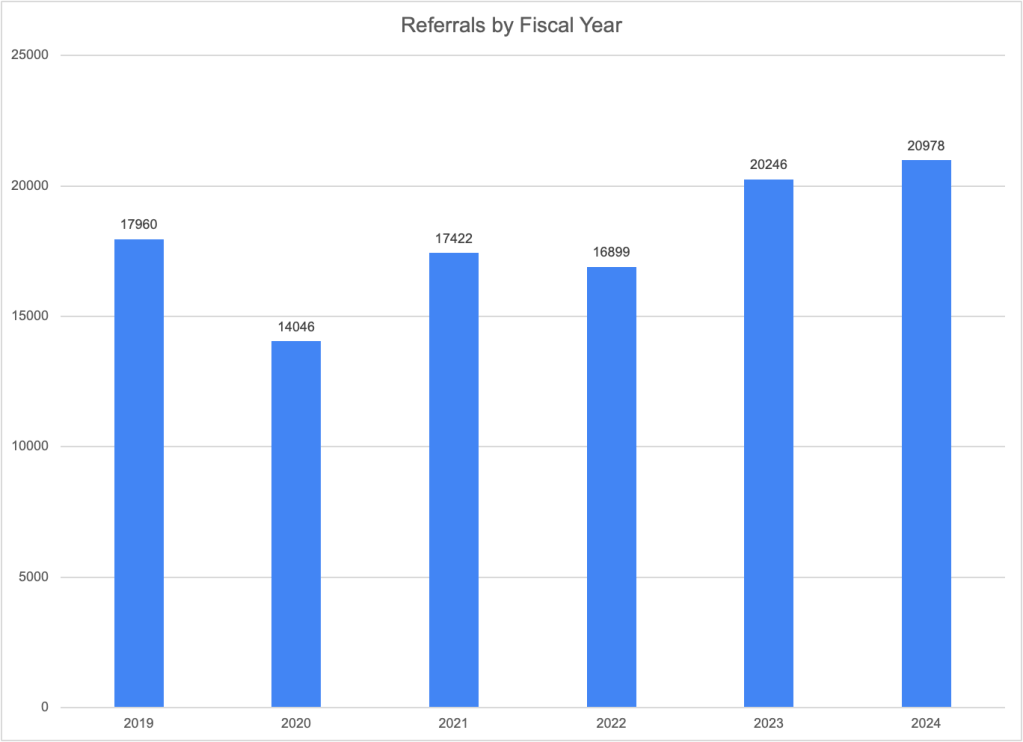
Total referrals (or calls to the CFSA hotline) have increased for the second year in a row. After falling in 2020 and remaining below 2019 levels in 2021 and 2022, the number of referrals jumped from 16,899 in FY2022 to 20,246 in FY2023 and then rose more modestly to 20,978 in 2024–an increase of 3.6 percent. Prominent child welfare scholars like Emily Putnam-Hornstein have concluded that referrals are the best available indicator of actual maltreatment due to the strong correlation between referrals and future reports (regardless of the outcome of any associated investigation) and also evidence of the difficulty of correctly determining whether maltreatment has occurred. Thus, the increase in referrals may well be a sign of increasing maltreatment. Contributing factors might be the end of COVID-19 assistance programs and the growing mental health, substance abuse, and housing crises in the District.
Childcare and school personnel continued to make more than half of the referrals to CFSA, with another 13 percent coming from law enforcement and 11 percent from friends and neighbors. All three of these groups made more referrals in FY2023 than FY2024, while counselors, therapists, social workers and medical professionals made fewer, suggesting that children may be seeing fewer of these professionals with the disappearance of virtual options spawned by the pandemic.
Looking at CFSA’s response to the referrals, the largest portion, or 73 percent, were screened out. That compares to only 19 percent that were accepted for investigation. The remaining referrals were either linked to an existing investigation (three percent) or classified as an information and referral that does not involve an allegation of abuse or neglect. These percentages are quite similar to those of the previous year.
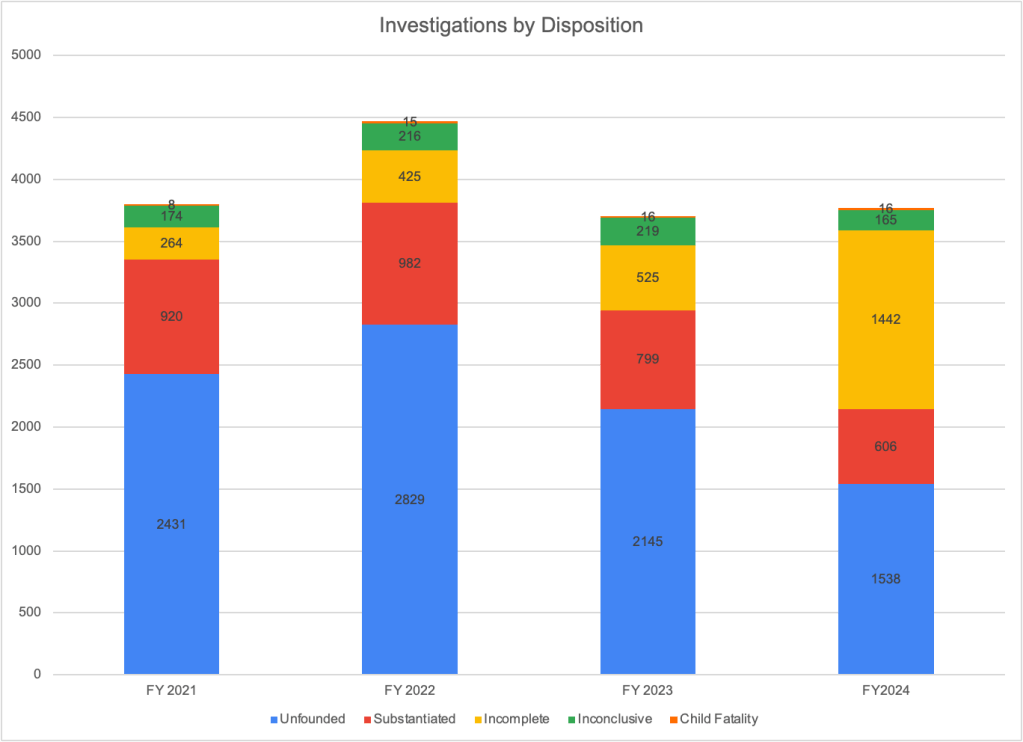
An investigation can have five different dispositions. According to the definitions provided in the Dashboard, unfounded means that there is not enough evidence to conclude that the child has been maltreated or at risk of being maltreated. “Substantiated” means that there is enough evidence to conclude that the child has been maltreated or is at risk of maltreatment. “Inconclusive,” means that “there is insufficient evidence to substantiate the report but there still exists some conflicting information that indicate the abuse or neglect may have occurred.” “Incomplete” means that the investigation could not be completed due to barriers like inability to locate the family, a family’s refusal of access to the home, or finding out that the family lived out of state.
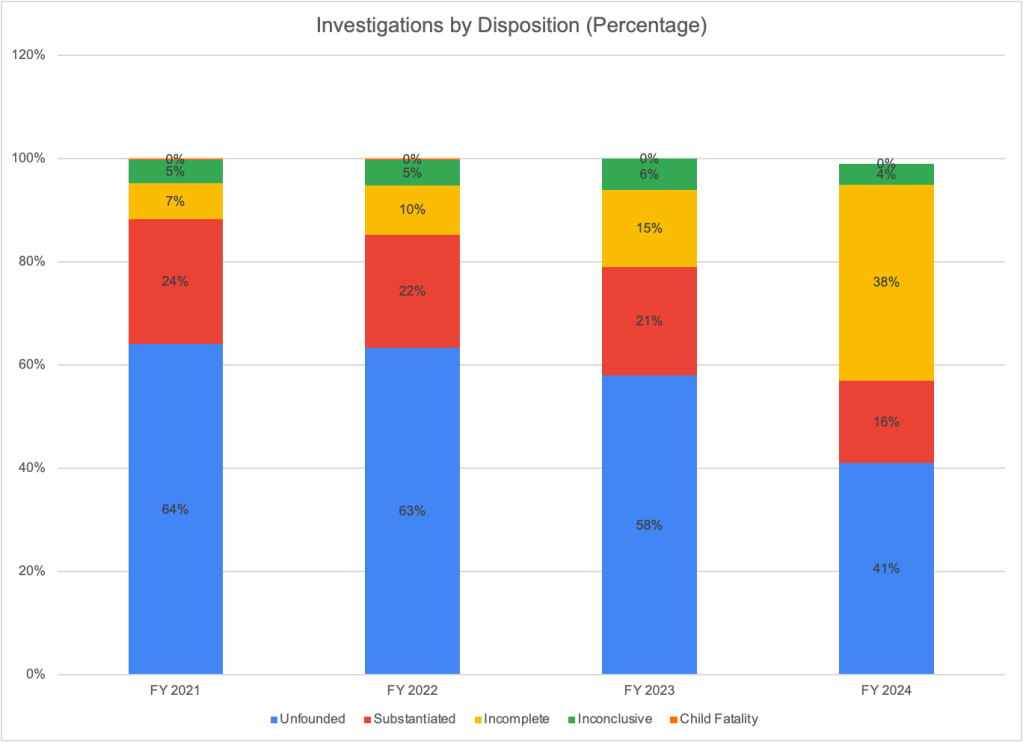
There was a big jump in the number of investigations categorized as incomplete, from 525 in FY2023 to 1,442 in FY2024. That was an increase from 15% of all investigations to 38% of all investigations. As a consequence of the increase in incomplete investigations, the number and percentage of investigations that were unfounded and substantiated dropped drastically. The number of investigations that were substantiated fell from 799 (21 percent of investigations) in FY2023 to 606 (or 16 percent of investigations) in FY2024. Unfounded remained the most common disposition in FY2024, but the proportion of cases that were unfounded dropped from 58 percent to 41 percent.
CFSA’s communications director did not respond to several emails asking for an explanation of the the jump in incomplete investigations. But it seems likely that this trend stems from the workforce crisis that is affecting CFSA and other child welfare and human services agencies around the country. A spreadsheet that the agency provided to the DC Kincare Alliance shows 27 out of the 36 social workers performing investigations as of August 2024 were carrying more than the 12 to 15 cases that CFSA uses as an indicator of satisfactory performance. This included 19 social workers carrying 20 or more cases and five social workers carrying more than 30 cases. Even more concerning is that the number of social workers doing investigations fell from 42 in January 2024 to 36 in August 2024, according to the spreadsheet.
If social workers are not able to complete the required interviews and collect needed information timely, endangered children may suffer further harm. It is possible that most of the incomplete investigations have been essentially concluded with a determination of findings, leaving only the completion of needed documentation and forms undone as workers hurried to start new investigations. Such a scenario might be somewhat less alarming but would still raise concerns that overburdened social workers are not able to thoroughly investigate allegations, thereby endangering vulnerable children.
In-Home Case Openings and Foster Care Placements
The table below shows the number of in-home case openings and children entering foster care by year. These two numbers cannot be added together because because in-home entries are reported at the case level (with multiple children in many cases) and foster care entries are reported at the child level. However the trends over time can be compared, showing that the number of in-home cases opened dropped between FY2023 and FY2024 while the number of children entering foster care increased. This was the first time the number of children entering foster care increased since FY2021, after the drop in foster care placement due to COVID-19.\
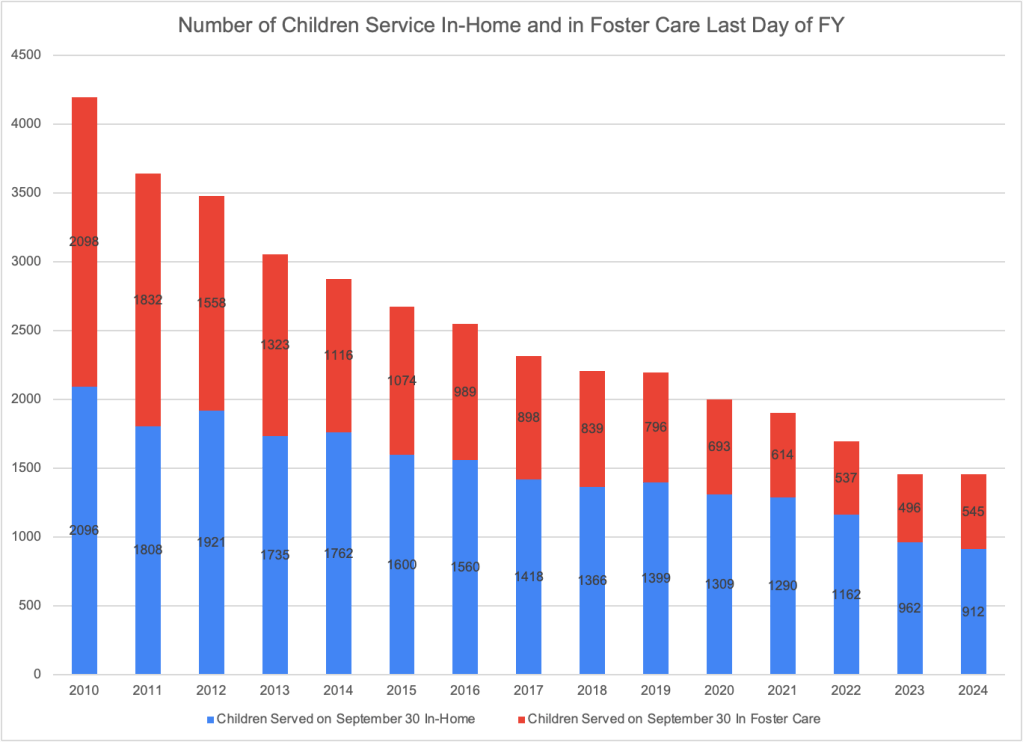
The total number of children served in home and in foster care on the last day of every quarter are available on the CFSA Dashboard and can be added to yield the total number of children served on that date. The chart below shows that the total number of children served on the last day of the fiscal year (September 30) stayed basically the same between FY2023 and FY2024. But the number of children being served in their homes decreased by 50 while the number in foster care increased by 49. FY2024 reverses a trend of annual decreases in the number of children in foster care going back at least as far as 2011.
The increase in the number of children in foster care between September 30, 2023 to September 30, 2024 reflects an excess of entries to foster care over exits from care during FY2024. Specifically, the number of children in foster care at the end of the fiscal year should reflect the number of children in foster care at the end of FY2023, plus the number of entries to foster care during the year, minus the number of exits from foster care. While there is a discrepancy of two between the results of this calculation and the foster care caseload reported by CFSA, the numbers confirm that there were about 50 more entries than exits, so the caseload increased. A similar calculation cannot be performed for children served in their homes, as the entry data are based on cases, not children.
It may be reassuring that the number of children served by CFSA changed so little in FY2023. One can hope that despite the high percentage of incomplete investigations, CPS workers are doing what is necessary to find the children that need help and simply leaving some of the paperwork for later. However, such a situation is not sustainable without endangering children. And the 3.6 percent increase in the number of referrals between FY2023 and FY2024 was not met with an increase in the number of children served, which may be a result of the incomplete cases.
It is not possible to understand the FY2024 data without further information from CFSA. How alarming the increase in incomplete investigations may be depends on whether these investigations are truly incomplete or basically finished except for forms and documentation. More concerning still, CFSA caseload data indicates that there are fewer than half the number of social workers doing this work now than in previous years. It is good that the total number of children being served has not dropped precipitously along with the drop in completed investigations. But the public needs to know more about how CFSA is functioning and what it is doing to alleviate the workforce crisis.
I am grateful to be publishing this essay by a gifted and needed young voice in the child welfare space. Liliana “Patty” Flores, MSW is a clinician, researcher, advocate, educator, and motivational speaker. Her intersectionality and affiliation with marginalized identities such as being an undocumented Salvadoran female, LGBTQ+, foster youth, homeless, and cycling in and out of juvenile jails, have shaped the way she sees social issues. Patty was born in El Salvador and migrated to the U.S. at age 10. She spent half of her life in foster care, struggling with substance abuse. Patty turned 18 years old in jail. She eventually graduated high school and enrolled in college while still incarcerated. She now has an A.A. in Social and Behavioral Sciences, an A.S. in Administration of Justice from Pierce College, a B.A. in Sociology from UC Riverside, and a Master’s in Social Work from Smith College. Her goal is to empower those of similar backgrounds like herself. Read more about Patty and her work at www.defyinglabels.com. –Marie Cohen
Imagine going to school with bumps on your head and bruises on your back and legs from being repeatedly punched and kicked; this was my reality as a kid. Youth with lived experiences in foster care face countless challenges, even when the abuse finally stops – one way or another. For me, it stopped because at age 12 I reported it. I then found myself in foster care and having to navigate the complicated child welfare system, speaking little English and knowing nothing about how the child protection system (CPS) works in this country. Although my experience in care was hard for numerous reasons, including substance use, incarceration, homelessness, and being undocumented, I am alive only because this country has a system of protection in place for children and youth like me who have been victimized by their parents.
The movement to abolish the current child welfare system –spearheaded by the organization upEND and its co-founder, Alan Detlaff–has sparked useless controversy and divided the community of people who are concerned with child safety, permanency, and wellbeing. Former foster youth like me, who are pursuing college and graduate education, are silenced in our classrooms. Also silenced are our allies, who are shamed for wanting to pursue a career in child welfare. The child welfare abolition movement originated from academics like Detlaff who have no lived experience of foster care. Who are these ivory tower elites to tell anyone that foster care is unnecessary and should be eliminated when they’ve not lived through it themselves?
The child welfare abolitionists have chosen to ignore those of us with lived experience of child abuse and neglect who refuse to endorse their program of eliminating the child protection system. Are they too uncomfortable to talk about the cruel truth of being an abused or neglected child? Do they fear this conversation will thwart their efforts to abolish the system? It’s much easier to ignore the issues of child abuse and child deaths, to avoid engagement with survivors, and to see only the adult perpetrators as victims, than to recognize the reality of child abuse and neglect. It is also much easier to talk about tearing a system down than to grapple with the question of how to build one up that truly promotes child safety, permanency, and well-being. It is harder to acknowledge the harms of child maltreatment and work together with us to find solutions that ensure our safety, stability, and well-being. Abolitionists are choosing the easy, less messy way out. They argue that foster care is not the answer. But for some of us, it is the only answer after experiencing abuse and neglect without extended family support.
I was born in El Salvador and am a descendant of the Pueblo Pipil, an indigenous group of people in El Salvador. I migrated to the United States as an unaccompanied minor at the age of ten. My background is rooted in a history of civil war and the struggle of oppressed indigenous people to overthrow those in power. In the United States, child welfare abolitionists often label themselves as “revolutionary” or claim to be engaging in “revolutionary” social work, but they are mistaken. True revolution occurs when the community rises up against oppression from those in power, not the other way around. These are the lessons I have learned from my revolutionary ancestors.
Child welfare abolitionists use the term to brand themselves as social justice warriors and silence those with lived foster care experiences. They discuss child protection and foster care among themselves, excluding the very people most affected. It is an abuse of power for the “abolitionists” to neglect the voices of those with lived experiences in foster care, while enhancing their own prestige within the elite ivory tower.
Advocates for abolishing the child welfare system (or as they call it, the “family policing system”) argue that collective efforts and community involvement are the solution in cases of child abuse and neglect. Yet nearly five years have passed since the inauguration of upEND, and the child welfare abolition movement has not provided specifics about how this would look in practice. Nor have I heard Dettlaff or other child welfare abolitionists discuss the experiences of young people like me who endured abuse and neglect. Are they afraid of the harsh realities we’ve experienced? How can they even talk about the child welfare system when they refuse to acknowledge our existence?
I keep asking myself these questions: where was the community when I witnessed my mother being violently attacked, with a gun held to her head by my father? Where was the community when Gabriel Fernandez lost his life? Where was the community when Danieal Kelly was starved to death by her mother? Or much more recently, as four-year-old Jahmeik Modlin, slowly starved to death in an apartment stocked with food? Where is the community when children continue to lose their lives at the hands of their caregivers daily? When I’ve spoken to community members about their role in intervening when child maltreatment or violence on the streets occurs (a “solution” prescribed by the “abolitionists”), they’ve expressed fears of retaliation or concerns about getting themselves into dangerous situations where they could be attacked by the perpetrators.
The child welfare abolitionists have manipulated many young people, students, and activists into adopting oversimplified, Black and White narratives that erase other ethnic groups and the intersectionality children like me experience. To support their argument, they assert that the media is responsible for over-emphasizing cases of abuse and deaths, which they contend are infrequent. But when you grow up witnessing so much violence, abuse, and neglect firsthand, you don’t have to watch the stories on the news. In fact, I did not grow up watching any TV. I learned about all this violence because I lived it.
College and university professors who support abolition (and who have never worked in the system) consistently push the narrative that CPS serves only to break Black and Brown families apart. They rarely if ever acknowledge the suffering endured by the over half a million children and youth who are abused and neglected annually and the need for a system of child protection in this country. As a young person with lived experience in an abusive family, I felt compelled to speak up in the classroom. And I did, immediately standing out with my thick accent and visible head tattoos. Fortunately, many of my classmates, including peers with experience in foster care, supported me and together we pushed back against professors’ biases and prejudice. I felt powerless growing up, and I still feel powerless as I navigate the racist, sexist, and classist world of academia.
In Defying Labels: From Negative Credentials to Positive Credentials?, an article I wrote for a newsletter at UC Riverside, I explained that society often shifts blame to the child for revealing family secrets in cases of abuse and neglect. The last thing I want as an adult is to keep being torn down and silenced by those in positions of power – professors, researchers, policy analysts, lawyers, and others. The abolition movement is tearing foster youth apart. Why not actually listen to what we have to say? This is the only way toward a safer world for all.
A fourteen-year-old boy and a fifteen-year-old girl are charged as adults, one for a mass shooting and the other for selling a fentanyl tablet that killed an older teenager. These two young people had something in common–a long history of neglect (and sometimes abuse) by their parents and a failure to intervene by child welfare services despite multiple reports that children were in danger. Ignoring chronically maltreated children when they could have been saved and then locking them up for life is both inhumane and costly. We must intervene to help maltreated children before they are irrevocably damaged by years of abuse and neglect.
On September 4, 2024, fourteen-year-old Colt Gray shot and killed two teachers and two students at Apalachee High School in Winder, Georgia with an AR-15 style rifle given to him by his father. He has been charged as an adult and is awaiting trial. It did not take long for the media to uncover that Colt had grown up in a chronically abusive and neglectful home. As the Washington Post put it in a devastating article, “Colt’s parents, each addicted to drugs and alcohol, were perpetually inattentive, often cruel and sometimes entirely absent, according to family members, neighbors, investigators, police reports and court records.” In November 2022, Colt’s mother, Marcee Gray, left his father, Colin Gray, and moved to southern Georgia with her two younger children. It appears that DCFS had opened a case at some point because In October of 2023, a spot drug-test revealed Marcee’s renewed drug use. Colin Gray was ordered to retrieve the other children, or they would be placed in foster care. Shortly thereafter, it appears that the case was closed.
There is no information from media reports about whether DCFS evaluated Colin Gray for his fitness to take care of his three children or to monitor their well-being in his care before closing the child welfare case. Yet, relatives reported to the New York Post that Colin Gray relentlessly bullied his son, calling him names like “sissy” and “bitch.” The Washington Post reported that Colt first came to the attention of authorities at the age of 11, when his school flagged him for searching the internet for ideas on how to kill his father. In Colin Gray’s custody, Colt never attended eighth grade and was not even registered for school until February 2 of that year. That Christmas, Colin Gray gave Colt his own AR-15 style rifle, in an attempt to “toughen him up,” as relatives told the New York Post. By his fourteenth birthday in January, Colt’s grandmother reported that he was searching the internet for what was wrong with him; she offered to pay for therapy and take him there but his father never signed him up. In July of 2023, Marcee returned from rehab and Colin allowed her to move back in. Colt’s mental health deteriorated even further after his mother’s return, and he talked of hurting himself or others. He registered for high school two weeks late and rarely attended. “Colt was like the thrown-away child,” said his grandmother, who tried in vain to get his father and the school to help him. Five days after his father failed to take him to a crisis mental health center despite his grandmother’s plea, Colt brought his rifle to school and took four lives.
Also charged as an adult was 15-year-old Maylia Sotelo of Green Bay, Wisconsin, the subject of a devastating article by Lizzie Presser of Pro Publica. Maylia’s home had been a “hangout for users and dealers.” Her three older sisters had all been kicked out or left due to their mother’s violence. Maylia’s had been referred to child protective services 20 times before she was finally removed from her home at the age of 14. In a pattern typical of chronic maltreatment, the reports concerned multiple types of neglect, sexual abuse, and physical abuse. Before Maylia turned one, CPS documents show that her mother overdosed on cocaine and Adderall with seven children in her home. When she was five years old, a caller reported that her mother was “high as a kite” and her boyfriend was violent. The next year, another report indicated that there was no food in the home and that the mother was using heroin in front of her children.
When Malia was seven, CPS substantiated a report that a man “opened his pants, pulled out his penis and masturbated” in front of one of Maylia’s sisters. That same year, a woman overdosed on crack in the house and Maylia’s mother “would not call rescue or the police because [she] did not want her children removed,” according to a social worker’s notes. And a school employee reported that Maylia missed half the school year. When Maylia was 14 and her mother became psychotic, Maylia and her sister were finally removed from the home and placed with relatives. But they were given no counseling or assistance with school, according to Pro Publica. Maylia had been smoking weed since fifth grade, then began selling it. By the beginning of tenth grade, she was selling “blues,” pills that were billed as percocet but actually contained filler and fentanyl. She sold a pill to an 18-year-old named Jack McDonough. When he died of an overdose, Maylia was arrested for first-degree reckless homicide.
It is obvious that both Colt Gray and Maylia Sotelo were chronically maltreated children who suffered from multiple types of maltreatment over a period of years. It is also obvious that the systems designed to protect them failed both of these young people. Both families clearly required intervention that did not come when it was needed, though we do not have enough details to make an informed critique of the system’s response. When the child welfare system finally intervened in Malia’s case, it may have been hard to change her trajectory, and it appears that she was left with relatives and received monitoring or services to address her traumatic history. In Colt’s case, the intervention may have also come too late to prevent serious psychological damage. And once they became involved, caseworkers appeared to be focused on his mother and ended the case with the placement of all three children with their father, a parent who had been equally neglectful and failed to take action to protect the children from his wife’s abuse.
Perhaps more intensive in-home services provided earlier could have helped Colt’s and Maylia’s parents address the issues that led them to abuse or neglect their children. If not, perhaps Maylia’s earlier removal from her toxic home, and Colin’s removal to a better environment than either of his parents could provide might have saved these children from the sad fate that awaited them. The approach that is currently in fashion – exemplified by the much touted Family First Prevention Services Act (FFPSA) of 2018 – prescribes the avoidance of foster care at almost any cost. It does, however, promise that parents receive support in parenting their children, whether it is mental health, drug treatment, or parenting training. Child welfare systems have long been providing such support to families in the form of in-home services, and FFPSA was supposed to provide the resources to improve these services. Unfortunately, FFPSA did not acknowledge or support the crucial role of frequent home visits to ensure the children are safe and that they can be removed into foster care if the parents do not cooperate with their plans for addressing their issues and improving their parenting.
Sadly, there is no evidence that increases in family support or child safety monitoring are forthcoming. States are proudly citing drops in their foster care caseloads, with no reporting on what is happening to the children left at home. States are not required to release data on the number of cases opened for in-home services, so we have no idea whether the abused and neglected children who are not being removed are getting any supervision or their parents receiving services. But as I have written, data from the states with the largest and third largest foster care caseloads indicates that the number of children receiving in-home services has not increased to make up for the drop in children removed to foster care; instead it has decreased along with foster care placements, resulting in a decline in the number of children being served overall.
Studies have documented the connection between child maltreatment and crime.1 Failing to intervene with at-risk children before they resort to crime and subsequently incarcerating them results in unnecessary human suffering, not to mention greater financial costs, than intervening early. If we do not want to remove more children, we must provide intensive services to parents and close monitoring of their children’s safety–and be ready to remove the children as soon as it becomes clear that parents are not going to change before the children are irreparably harmed. Such monitoring is key, because we really do not know what, if anything, works in preventing future maltreatment among parents who have maltreated their children.
This is not the first time that the failure of CPS has been noted in the wake of a heinous crime. I previously wrote about Lisa Montgomery, who was executed on January 12, 2021. She murdered a pregnant woman, cut out the baby, and took it home. It turned out that Lisa Montgomery had a long and horrific history of physical and sexual abuse throughout her childhood, including beatings and bizarre punishments by her mother, rape by her stepfather, and prostitution by both. Sadly, it seems that we have not made much progress since Lisa’s childhood, and current ideological trends run the risk of leaving even more children unprotected in the future.
The MacArthur Foundation has announced its new class of Fellows, the recipients of what are commonly called the “Genius Awards.” Among the recipients is Dorothy Roberts, the self-styled popularizer of the term “racial disproportionality” and creator of the term “the family policing system.” According to the Director of the Program, “The 2024 MacArthur Fellows pursue rigorous inquiry with aspiration and purpose. They expose biases built into emerging technologies and social systems….” It’s hard to understand how this term can be applied to an author who wrote that the “family-policing system terrorizes Black families because that’s what it is designed to do ” despite also stating that child welfare systems excluded Black children from their inception until the second half of the twentieth century. The choice of Roberts only exposes the bias and lack of rigor–or alternatively the sheer ignorance– of the MacArthur Foundation. As an illustration, I am reposting my 2022 review of Roberts’ most recent book, Torn Apart: How the Child Welfare System Destroys Black Families–and How Abolition Can Build a Safer World.
In her 2009 book, Shattered Bonds: The Color of Child Welfare, Dorothy Roberts drew attention to the disproportional representation of Black children in foster care and child welfare in general and helped make “racial disproportionality” a buzzword in the child welfare world. In her new book, Torn Apart: How the Child Welfare System Destroys Black Families–And How Abolition Can Build a Safer World, Roberts revisits the issues addressed in Shattered Bonds and creates a new buzzword, renaming child welfare as the “family policing system.” Those who liked Shattered Bonds will likely love Torn Apart. But those who value accuracy in history or in data will find it to be sadly misguided, although it does make some valid points about flaws in the U.S. child welfare system.
Roberts starts with a horrific anecdote about a mother, Vanessa Peoples, who was doing everything right–she was married, going to nursing school, about to rent a townhouse and was even a cancer patient. But Peoples attracted the attention of both the police and child welfare and ended up hogtied and carted off to jail by police, placed on the child abuse registry, and subjected to months of monitoring by CPS after she lost sight of her toddler at a family picnic when a cousin was supposed to be watching him. But citing these extreme anecdotes as typical is very misleading. This particular story has been covered in numerous media outlets since it occurred in 2017 and continues to be cited regularly. One can counter every one of these horrific anecdotes with a story of a Black child who would have been saved if social workers had not believed and deferred to the parents. (See my commentary on the abuse homicides of Rashid Bryant and Julissia Batties, for example).
Roberts’ book restates many of the old myths that have been plaguing child welfare discussions as of late and that seem to have a life of their own, impervious to the facts. Perhaps the most common and pernicious is the myth that poverty is synonymous with neglect. Roberts embraces this misconception, suggesting that most neglect findings reflect parents who are too poor to provide adequate housing, clothing and food to their children. But parents who are found to have neglected their children typically have serious, chronic mental illness or substance use disorders that severely affect their parenting, and have refused or are unable to comply with a treatment plan. Many are chronically neglectful, resulting in children with cognitive and social deficits, attachment disorders, and emotional regulation problems. Commentator Dee Wilson argues based on his decades of experience in child welfare that “a large percentage of neglect cases which receive post-investigation services, or which result in foster placement, involve a combination of economic deprivation and psychological affliction…., which often lead to substance abuse as a method of self-medication.” Perhaps the strongest argument against the myth that poverty and neglect are one and the same is that most poor parents do not neglect their children. They find a way to provide safe and consistent care, even without the resources they desperately need and deserve.
Roberts endorses another common myth–that children are worse off in foster care than they would be if they remained in their original homes. She argues that foster care is a “toxic state intervention that inflicts immediate and long-lasting damage on children, producing adverse outcomes for their health, education, income, housing, and relationships.” It is certainly true that foster youth tend to have bad outcomes in multiple domains, including education, health, mental health, education, housing and incarceration. But we also know that child abuse and neglect are associated with similar poor outcomes. Unfortunately, the research is not very helpful for resolving the question of whether these outcomes are caused by the original child maltreatment or by placement in foster care. We cannot, of course, ethically perform a controlled study in which we remove some children and leave a similar set of children at home. We must rely on studies that use various methodologies to disentangle these influences, but all of them have flaws. Roberts cites the study published in 2007 by Joseph Doyle, which compared children who were placed in foster care with children in similar situations who were not. Doyle found that children placed in foster care fared worse on every outcome than children who remained at home. [Update added October 2024: A newer study, reflecting current foster care policy and the more typical state of Michigan, found the opposite result.] But focusing on marginal cases* leaves out the children suffering the most severe and obvious maltreatment. In a recent paper, Doyle, along with Anthony Bald and other co-authors, states that both positive and negative effects have been found for different contexts, subgroups, and study designs.
There is one myth that Roberts does not endorse: the myth that disproportional representation of Black children in child welfare is due to racial bias in the child welfare system, rather than different levels of maltreatment in the two populations. After an extensive review of the debate on this issue, Roberts concludes that it focused on the wrong question. In her current opinion, it doesn’t matter if Black children are more likely to be taken into foster care because they are more often maltreated. “It isn’t enough,” she states, “to argue that Black children are in greater need of help. We should be asking why the government addresses their needs in such a violent way, (referring to the child removal). Roberts was clever to abandon the side that believes in bias rather than different need as the source of disparities. The evidence has become quite clear that Black-White disparities in maltreatment are sufficient to explain the disparity of their involvement in child welfare; for example Black children are three times as likely to die from abuse or neglect as White children. As Roberts suggests and as commentators widely agree, these disparities in abuse and neglect can be explained by the disparities in the rates of poverty and other maltreatment risk factors stemming from our country’s history of slavery and racism. Unfortunately, Roberts’ continued focus on these disparities in child welfare involvement will continue to be used by the many professionals who are working inside and outside child welfare systems all over the country to implement various bias reduction strategies, from implicit bias training to “blind removals.”
In Part III, entitled “Design,” Roberts attempts to trace the current child welfare system to the sale of enslaved children and a system of forced “apprenticeship” of formerly enslaved Black children under Jim Crow, whereby white planters seized custody of Black children from their parents as a source of forced labor.** As she puts it, “[t]hroughout its history US family policy has revolved around the racist belief that Black parents are unfit to raise their children. Beginning with chattel slavery and continuing through the Jim Crow, civil rights, and neoliberal eras, the white power structure has wielded this lie as a rationale to control Black communities, exploit Black labor, and quell Black rebellion by assaulting Black families.” In other passages she adds other groups to the list of victims, adding “Indigenous, immigrant and poor people to the list of communities that are being controlled by the “family policing system.” But most of her statements refer to Black victims only.
Roberts’ attempt to connect slavery and Jim Crow practices with child welfare systems highlights a major flaw of the book. She herself explains that due to racism the child welfare system served only White children when it emerged in the nineteenth century with the creation of child protection charities and the passage of state laws allowing maltreated children to be removed from their homes and placed in orphanages. Foster care was established in the middle of the century and also excluded Black children. The system did not begin serving Black children until after World War II, so it is difficult to understand how it could stem from slavery and Jim Crow practices. It seems much more plausible that the child welfare system arose from basically benevolent concerns about children being maltreated, and that with the rise of the civil rights movement, these concerns were eventually extended to Black children as well.
While Black children’s representation as a share of foster care and child welfare caseloads rose rapidly starting in the 1960’s, and Black children are much more likely to be touched by the system than White children, the system still involves more White than Black children. According to the latest figures, there were 175,870 White non-Hispanic children in foster care (or 44 percent of children in foster care) and 92,237 Black (non-Hispanic) children in foster care, or 23 percent of children in foster care. Moreover, the disparity between Black and White participation in child welfare and foster care as a percentage of the population seems to be decreasing.*** So the idea that this whole system exists to oppress the Black community and maintain white supremacy seems farfetched.
Roberts’ attempt to make Black children the focus of the book results in some awkward juxtapositions, like when she admits that though the Senate investigation of abuses by a for-profit foster care agency called MENTOR “highlighted cases involving white children, we should remember that Black children are more likely to experience these horrors in foster care—not only because Black children are thrown in foster care at higher rates, but also because government officials have historically cared less about their well-being.” A page later she states that the “child welfare system’s treatment of children in its custody is appalling but should come as no surprise. It is the predictable consequence of a system aimed at oppressing Black communities, not protecting Black children.” It is hard to understand how White children being maltreated in bad placements supports this narrative.
Fundamental to Roberts’ critique is her system is “not broken.” “Those in power have no interest in fundamentally changing a system that is benefiting them financially and politically, one that continues to serve their interests in disempowering Black communities, reinforcing a white supremacist power structure, and stifling calls for radical social change.” Even if one believes there is a white supremacist power structure, it is hard to see the direct connection between the abuses Roberts is highlighting and the disempowerment of Black communities; it seems more likely that the more abusive the system, the more protests it would generate. And at a time when the federal government and some of the wealthiest foundations and nongovernmental organizations are echoing much of Robert’s rhetoric, her reasoning seems particularly off-target.
Roberts makes some valid criticisms of the child welfare system. Her outrage at the terrible inadequacies of our foster care system is well-deserved. She is right that “The government should be able to show that foster care puts Black children [I’d say “all children”] on a different trajectory away from poverty, homelessness, juvenile detention, and prison and toward a brighter future.” Any society that removes children from their parents needs to be responsible for providing a nurturing environment that is much, much better than what they are removed from. And we are not doing that. As Roberts states, “The state forces children suffering from painful separations from their families into the hands of substitute caretakers…..who often have unstable connections, lack oversight and may be motivated strictly by the monetary rewards reaped from the arrangement.” As a foster care social worker in the District of Columbia, I was driven to despair at my inability to get my superiors to revoke the licenses of such foster parents; the need for “beds” was too great to exclude anyone was not actually guilty of abuse or severe neglect. Roberts is also right to be concerned the outsourcing of foster care to private for-profit organizations that may be more concerned with making money than protecting children, sometimes resulting in scandals like the one involving MENTOR Inc., which was found to hire unqualified foster parents and fail to remove them even after egregious violations like sexual assault.
Roberts also raises valid concerns about children being sent to residential facilities, often out of state, that resemble prisons rather than therapeutic facilities. But she ignores the need for more high-quality congregate care options for those children who have been so damaged by years of maltreatment that they cannot function in a foster home, no matter how nurturing. Instead, she repeats the usual litany of scandals involving deaths, injuries, fights and restraints, without noting the undersupply of truly therapeutic residential settings, resulting in children sleeping in office, cars, and hotels or remaining in hospital wards after they are ready for discharge. Ironically, she supports defunding the system, even if that would mean even worse situations for these children.
Roberts decries the fact that parents sometimes relinquish custody of their children in order to get needed residential care, arguing that “rather than providing mental health care directly to families, child welfare authorities require families to relinquish custody of children so they can be locked in residential treatment centers run by state and business partnerships.” That statement is completely backwards. The child welfare system does not provide mental health services but, like parents, it often struggles to secure them for its clients. Some parents are forced to turn to the child welfare system because their insurance will not pay for residential care for their children. That is not the fault of child welfare systems, which clearly do not want to take custody of these children. The underlying problem is the lack of adequate mental health care (including both outpatient and residential programs), which has destructive consequences for the foster care system. This is exacerbated by the lack of parity for mental health in health insurance programs. It’s hard to believe Robert is unaware of these well-known facts.
Roberts is correct that parents as well as children are shortchanged by inadequacies in our child welfare program, such as the “cookie cutter” service plans which often contain conflicting obligations that are difficult for struggling parents to meet. But she is wrong when she says that parents need only material support, not therapeutic services. But this error flows logically from her concept of neglect as simply a reflection of poverty. In fact, many of these parents need high-quality behavioral health services and drug treatment, which are often not available because of our nation’s mental health crisis, as well as the unwillingness of taxpayers and governments at all levels to adequately fund these services.
In her final chapter, Roberts concludes that, like the prison system, the child welfare system cannot be repaired because it exists to oppress Black people. “The only way to end the destruction caused by the child welfare system is to dismantle it while at the same time building a safer and more caring society that has no need to tear families apart.” In place of family policing, Roberts favors policies that improve children’s well-being, such as “a living wage and income support for parents, high-quality housing, nutrition, education, child care, health care; freedom from state and private violence; and a clean environment.” I agree with Roberts that aid to children must be expanded. The US is benighted when compared to many other Western countries that invest much more heavily in their children through income support, early childhood and K-12 education, healthcare, and housing. But family dysfunction occurs even if a family’s material needs are met. That is why every other developed nation has a child welfare system with the authority to investigate maltreatment allegations and assume custody of children when there are no other options. Moreover, some of the countries with the strongest safety nets for children also have higher percentages of children living in foster care than the United States.****
Torn Apart is a skewed portrait of the child welfare system. In it Roberts restates the common but easily discredited myths that poverty is synonymous with neglect and that foster care makes children worse off than they would have been if left at home. The underlying flaw in her account is the idea that this system exists to repress the Black community, even though it was established solely for the protection of White children. Roberts makes some valid criticisms of child welfare systems and how they shortchange the children and families they are supposed to help. But when she talks of dismantling child protection, she is proposing the abandonment of abused and neglected Black children in homes that are toxic to them, an abandonment that will perpetuate an intergenerational cycle of abuse and neglect. These children are our future; abandoning their well-being to prioritize that of their parents is a bad bargain with history.
*Doyle’s study included only those cases that would have resulted in foster placement by some investigators and not by others, leaving out the cases in which children were in such danger that all investigative social workers would agree that they should be placed.
**In various places, she also attributes it to different combinations of slavery and apprenticeship of Black children with the transfer of Native American children to boarding schools, the exclusion of Black children from charitable aid and the servitude of impoverished White children.
***A recent paper reports that disparities between Black and White children began to decrease in the twenty-first century in nearly every state, closing entirely in several Southern states.
****Unicef’s report, Children in Alternative Care, shows that Denmark has 982 children in “alternative care” per 100,000 and Sweden has 872 per 100,000, compared to 500 per 100,000 for the United States.
A new report by the Senate Finance Committee concludes that children in residential treatment facilities routinely suffer harms like sexual and physical abuse, unsafe and unsanitary conditions, and lack of needed therapy. Further, it concludes that these harms are endemic to residential care itself. While the fact that some residential care facilities are substandard and cause harm to children is undisputed, the SFC’s study is poorly designed and should not be used as the basis of policy. It is based on facilities run by only four companies and cannot be used to make generalizations about residential care as a whole. Both the study design and the findings of the SFC report appear to stem from a preconceived conclusion and not on a desire to describe the actual landscape of residential care for America’s youth who need intensive behavioral health care.
On June 12, 2024, the Senate Finance Committee (SFC) released a report called Warehouses of Neglect: How Taxpayers are Funding Systemic Abuse in Youth Residential Treatment Centers. The report was based on an investigation of what it calls residential treatment facilities (RTF’s) operated by four large companies, “each owning facilities with a history of public abuse and neglect allegations and a substantial facility footprint.” It does not define RTF’s, but the term clearly refers to facilities that provide behavioral health services in a residential context to children with funding from programs under SFC jurisdiction, mainly Medicaid and foster care funds under Title IV-E of the Social Security Act. The four companies include three profit making corporations (United Health Services, Acadia Healthcare, and Vivant Behavioral Healthcare), and one nonprofit, Devereux Advanced Behavioral Health.
The report describes a pattern of poor conditions and abusive practices that the SFC staff observed by reviewing media articles and company documents, supplemented by interviews with senior leaders in the four companies and visits to several facilities not operated by these companies.1 These conditions and practices include sexual and physical abuse by staff; the inappropriate and often abusive use of restraints and seclusion; staff who are unqualified and inadequately trained staff or who routinely fail to discharge their duties, leading sometimes to tragic results; “non-homelike,” unsanitary and unsafe conditions; failure to provide the treatment that children need and that states are paying for; failure to maintain connections between children and their communities and to make adequate discharge plans; use of technology to monitor children that is more appropriate to detention facilities than therapeutic settings; and the absence of adequate oversight by state and federal authorities.
The report raises valid concerns about private businesses being involved in services to the most fragile young people. Several details stand out, all of them involving the company called Vivant and its CEO, John “Jay” Ripley. Ripley is the former CEO of Precision Tune Auto Care and and cofounder of BGR the Burger Joint. Ripley previously founded Sequel Youth and Family Services, which became known for the death of 16-year-old Cornelius Frederick while being restrained at a Michigan facility in 2020 and allegations of abuse and neglect at other Sequel facilities. In 2021, according to the report, Sequel closed half of its facilities and sold the other half, including 13 facilities that it sold to Vivant, Ripley’s new company. VIvant in turn hired many former Sequel executives and staff. In a video made by the University of Baltimore’s Merrick School of Business, Ripley explained that “you can make money in this business if you control staffing.” Ripley does not seem like the kind of person who should be running facilities dedicated to healing the most vulnerable young people.
The SFC report might have been a valuable document had it not tried to apply its findings to residential care in general. “Children suffer routine harm inside RTF’s,” the authors write. “These harms include sexual, physical, and emotional abuse, unsafe and unsanitary conditions, and inadequate provision of behavioral health treatment.” Leaving aside the ambiguity of the word “routine” (does that mean every resident or the majority of residents are harmed in such a way?), such a conclusion cannot be drawn from an investigation of treatment centers operated by four large companies. We have no idea what proportion of young people receiving publicly funded RTF care are in facilities operated by these four companies. Around the country, there are residential treatment facilities operated by many providers, including many freestanding facilities that are not part of large chains. Even within the companies reviewed, the report provides no data to document whether the problems exist only at certain facilities or throughout the chains. A facility’s functioning to a large extent reflects its leadership, and there may be well-run facilities among those operated by these companies.
Going even further, the SFC concludes that “the risk of harm to children in RTF’s is endemic to the operating model. The harms children in RTFs experienced are the direct, causal result of an operating model that incentivizes providers to optimize revenues and operating and profit margin. RTF providers offer minimal therapeutic treatment in deficient physical settings with lean staff composed of non-professionals, which maximizes per diem margins…” The report goes on to say that “[a]t its core, the RTF model typically optimizes profit over the wellbeing and safety of children.” But there is no “RTF operating model.” The understaffing and lack of professionals that are common among publicly funded residential providers more likely stem from the low reimbursement rates that that these programs receive, which in turn means that staff receive low pay as well, forcing the facilities to rely on poorly educated and trained staff.
Even more extremely, the report states that “In the best of circumstances, children at RTFs receive care from under-trained and overburdened staff, are given infrequent therapy, sometimes by non-professionals, and are exposed to unsanitary, unsafe, and non-homelike environments.” It is hard to understand how the SFC is capable of describing the best residential programs when its entire methodology consisted of seeking abuses in an extremely limited universe of residential programs.
In suggesting that residential treatment is a flawed model that should not exist, the SFC report ignores the important role of residential treatment facilities in the continuum of care for young people with mental illness. The Committee’s own invited witness, Elizabeth Manley of the University of Connecticut School of Social Work, testified about the need for these programs.
Residential treatment facilities have an important role in the provision of care for young people with complex behavioral health care needs when they have a clinical or behavioral health treatment need that cannot be met in a family and community setting due to the intensity of their treatment and supervision needs. In those instances, we need the care to be delivered in trauma-responsive environments that embrace parent and caregiver engagement throughout the treatment intervention and continually focus on best practice. These residential treatment facilities can have a significant benefit to the young person and their family.
The Child Welfare League (CWLA), in written testimony submitted to the SFC, added that residential services are “a small but important part of the full array of services” that must be available to meet children’s mental health needs.” CWLA went on to explain that there “are many providers and programs providing or striving to provide trauma-responsive, time-limited, effective residential care. They are informed by the emerging literature highlighting promising practices in residential interventions..” CWLA cited the Building Bridges Initiative, which is a national initiative working to identify and promote best practice and policy in residential interventions for youth. The initiative has produced a guide called Building Effective Short-Term Residential Interventions. According to this report, a new literature has developed in the last ten years or so which documents promising practices in residential intervention which are associated with positive benefits. These include “actively engaging youth and families, ensuring active school and community connection, and keeping residential intervention as short as possible.” The authors explain that “[c]utting-edge effective residential intervention now means providers are creatively working with youth and families in the home, in the community, and as briefly as possible – often for three months or less.” The guide was developed to help organizations make the transition to the new approach, with case histories of 12 programs that are making or have made this transition.
Ignoring this new literature, the SFC claims that “studies show that home and community-based approaches produce better treatment outcomes than placing children in RTFs, and are more cost-effective than RTF placements.” In the footnote to that sentence, the writers list only one study, which concerns only one type of facility, Psychiatric Residential Treatment Facilities, a particular model the provides the equivalent of in-patient psychiatric services outside a hospital setting to young people under 21 through an agreement with a State Medicaid agency. Moreover, that study does not conclude that community-based approaches produce better treatment programs. Instead, it concludes that “evidence is insufficient to assess which interventions are effective.” It is almost impossible to conduct a meaningful study comparing residential treatment to community-based approaches, since the children who are sent to RTF’s are generally much more troubled or impaired than the children who are not, and it would be hard to control for such differences without doing a randomized controlled trial. That’s why there are few if any studies that shed light on this issue.
It is hard to avoid the conclusion that both the study design and the findings of the SFC reflect the Committee’s desire to show that residential care is harmful to young people. The SFC’s anti-residential bias is displayed in numerous passages throughout the report. One particularly inaccurate statement claims that “In some cases….., child welfare agencies place children in state custody without diagnoses in RTFs because they have nowhere else to place them.” As evidence, the report cites a 2013 report that showed 28.8 percent of children in “congregate care” had no clinical diagnoses. But congregate care (a term used to designate any placement that is not a foster home) is a more general term than RTF’s. The earlier report included many other types of facilities including cottage-style homes (often on the site of former orphanages and often providing high-quality family-style care) that are not intended for children with serious behavioral health needs, as well as emergency shelters that some states operate to house children before they are placed in a foster home. Given the relatively high cost of RTF’s, it would be very strange if states placed children in them for lack of another option.
Much more common is the opposite scenario: agencies placing children in foster homes unprepared to care for them, resulting in placement instability, or even letting them sleep in hotels or offices, for lack of residential treatment facilities. Articles about this problem appear frequently, including a recent report from the Midwest Newsroom (a collaboration between NPR and Midwest member stations) on the insufficient capacity of residential care for girls in Missouri and Iowa. The article starts with the story of a young woman who was placed in a residential treatment program called Missouri Girls Town after a traumatic childhood, placement in foster care and a disrupted adoption by a parent who could not handle her rebellious adolescence. This young woman credits Missouri Girls Town with completely changing the trajectory of her life. Sadly, this nonprofit program, which relies on private donations to supplement what it gets from government agencies, was designed to accommodate up to 50 girls but can only take 12 because of “staffing and funding challenges.” Stories like this have been appearing from around the country for years. There is not enough residential treatment for the young people in foster care who need it. Facilities have been shutting down due to failure of state reimbursement rates to keep up with operating costs, as well as the increasing unpopularity of residential care among state officials and legislators.
Despite the major flaws in the SFC’s analysis, there is little to object to in its recommendations. It’s hard to argue against recommendations that Congress act to improve conditions in congregate care facilities, that the companies reviewed raise their standards, and that states invest in community-based services for children with behavioral health needs and improve oversight over RTF’s. The need to invest in community-based services is particularly important because it might enable some children to be helped before their problems become so severe that they need residential care. It might even prevent some placements in foster care that occur when parents can no longer care for behaviorally challenging their children at home. But the findings of the report remain dangerous even if the recommendations are benign; they can be used to support attempts to defund residential care entirely, which would be disastrous for our most vulnerable young people and their families.
The SFC report confounds a group of residential treatment facilities poorly run by four large corporations with the entire field of residential treatment for youth with serious behavioral health care needs. The report presents a distorted picture of a field that already contains excellent, life-changing programs and where passionate and dedicated leaders are already providing or working toward trauma-informed, short-term, and effective residential services for these most vulnerable young people.
Visits to five facilities that were not operated by the four providers being investigated were used to document physical conditions in the facilities, as well as their efforts to provide education to the residents. The finding of “non-homelike,” unsanitary and unsafe conditions was based on the visited facilities rather than on the four companies that were investigated. ↩︎
Year after year, states and the federal government continue to release annual data showing a decline in the number of children in foster care, congratulating themselves on keeping families together. They seem to have forgotten that reductions in foster care were supposed to be accompanied by increased services so that children could be safely maintained at home. Unfortunately, there seems to be little to no interest on the part of the federal Children’s Bureau, Members of Congress, advocates, or the media in whether such services are actually being provided.
The newest report from the Adoption and Foster Care Analysis and Reporting System (AFCARS) showed that the number of children in foster care dropped to 368,530 on September in 2022–a drop of 5.8 percent over the previous year 15.6 percent since 2018. “We are encouraged by the continued decrease in the number of children entering foster care and staying in foster care and we will continue working with our state, tribal and territorial partners to ensure an emphasis on family well-being and safe family reunification,” said Jeff Hild, the Principal Deputy Assistant Secretary of the Administration on Children and Families (ACF) in a press release heralding the new numbers. ACF gave credit to the Family First Prevention Services Act (FFPSA), which “helped change the conversation to be about prevention of foster care placements and preservation of families.”
It seems premature to celebrate the shrinkage of the foster care rolls as a triumph without knowing what is happening to the children remaining at home who would have been removed in a different year. How many of these children are living with abuse or neglect that will leave lasting scars or impair their development, if not endanger their lives? Supporters of the Family First Prevention Services Act (FFPSA), which passed in 2018, said that declining foster care counts would result from providing support to parents who needed help to address the problems (like substance abuse, mental illness and poor parenting skills) that led to their maltreatment of their children.
After an allegation of abuse or neglect is substantiated, an agency can place a child in foster care or open a case for in-home services, among other options.1 FFPSA made it possible to use the same federal funds for foster care and in-home services, allowing children to stay at home safely while their parents addressed the issues that put them at risk. A major purpose of FFPSA was to enable states to use federal funds that were formerly available only for foster care to pay for parenting support, mental health, and drug treatment that would enable children to stay safely with their families. The rationale for this change was that allowing foster care funds to be used for such services was necessary to enable states to keep kids out of foster care.
However, FFPSA has not made massive federal resources available for such services. ACF estimates that only 18,400 children in the entire country were served by Title IV-E prevention services programs in FY 2023, at a cost of $167 million. But perhaps states are using their own funds to pay for these services? After all, foster care is more expensive than services provided to families in their homes. Both require case management, but instead of the cost of room and board for foster youth, providing in-home services usually involve referring parents to mental health and drug treatment services often funded by Medicaid or paying for parenting support programs that cost less than foster care. (Of course the supporters of FFPSA ignored this basic fact and claimed the legislation would revolutionize child welfare!). States were already providing these services before FFPSA and they could have increased them without the promised federal funding.
But believe it or not, nobody knows if more children and their families are receiving in-home services as the foster care rolls decline, since the federal government doesn’t ask states for this information. While states were already required to report the number of children entering foster care, leaving it, and in care at a point in time, FFPSA did not add a requirement to provide the same data on services provided to children and families in their homes, now that they were also covered by federal Title IV-E funds.2 Hoping some states might track this data of their own accord, I searched the data publications and dashboards on the websites of the ten states with the largest number of children in foster care according to the most recent AFCARS report,3 but I was able to obtain this data for only California and Texas.
California has by far more children in foster care than any other state, 45,924 children at the end of September, 2022, which was 12.4 percent of the national total. Fortunately, there is extraordinarily good data from the California Child Welfare Indicators Project (CCWIP), a collaboration between University of California at Berkeley and the California Department of Social Services. The CCWIP dashboards include data on the number of entries into foster care and the opening of Family Maintenance cases, as in-home cases are called in California. Entries into foster care declined precipitously from April 2019 to March 2020 and continued declining, though more slowly, through March 2024. Family Maintenance case openings also declined continuously throughout the period. Thus, there was no increase in Family Maintenance case openings to compensate for the decline in removals. Or put in a different way, the total number of cases opened for child welfare services dropped from 46,264 at the beginning of the period to 29,969 at the end–a drop of 35 percent. Rather than a shift from foster care to in-home services, there has been a shrinkage of children reached by child welfare services overall.
Texas has the third largest state foster care caseload, after Florida. The Texas data are a bit more confusing. The number of children entering foster care dropped from 16,028 in 2021 to 9,623 in 2022, an incredible 40 percent, while the number of children entering in-home services declined steeply as well, resulting in a 35.7 percent drop in all case openings. Both drops may well have been related to a new Texas law that took effect on September 1, 2021 and changed the definition of neglect to an action or lack of action that puts a child in “immediate danger” of harm, rather than “substantial risk” of harm as the previous language read. The bill also put restrictions on child removals, requiring that children can be removed only from parents who display “blatant disregard” for their actions, or whose inaction “results in harm to the child or creates an immediate danger to the child’s physical health or safety.” Interestingly, in 2022, foster care entries actually rose slightly in Texas, while family preservation entries sprung back to where they were in FY2021, resulting a substantial increase in total case openings that year. Nevertheless, the overall trend over time was a decrease in foster care entries, family preservation case openings and the total number of children receiving help through open in-home or out-of home cases. That total dropped from 72,181 to 48,619 over five years–a drop of 32.6 percent–almost the same as the drop in California’s child welfare case openings.
Florida, the state with the second largest number of children in foster care, reports on the numbers of children entering foster care but not on the number entering in-home cases. One can, however, compare the number of children in foster care at a point in time with the number of children and young adults receiving in-home services. Both numbers have been decreasing and the number of children receiving in-home services has been consistently about half of the number of children in foster care. But these numbers don’t tell us whether declining entries to foster care have been offset by increasing entries to in-home services. In general, foster care cases last longer than in-home cases. Not knowing the average length of stays in foster care and in-home cases, and how they have changed over time, one cannot tell whether in-home case openings have made up for the reduced number of entries into foster care.
The Florida data show why point-in-time data cannot be used to answer the question of whether the decline in foster care entries has been accompanied by a rise in in-home case openings. Unfortunately, none of the other eight states with the highest caseloads provide this data on their websites. Illinois and Indiana provide point-in-time data on foster care and in-home participants. The other five states with the largest caseloads–Ohio, New York, Pennsylvania, Arizona, and North Carolina–display no data on in-home case participants at all.
If California and Texas are typical, states have not been increasing their provision of in-home services to make up for declines in foster care. Instead, the total number of abused and neglected children being helped by in-home or out-of-home services (or foster care) has declined by as much as a third in five years. But we cannot assume that California and Texas represent the entire nation. It is unfortunate that the writers of FFPSA did not requiring states to include data on in-home case openings and total caseloads, given that the legislation allowed federal funds to be used for this purpose. States have not begun tracking and reporting on this data on their own, and are triumphantly proclaiming the drop in foster care without even reporting on whether in-home services are being provided instead. When Congress considers desperately-needed fixes to FFPSA, a requirement that states report in-home case data analogous to the foster care data in the AFCARS system should be included in the new legislation.
Notes
Other options include referring a family to a community provider or even doing nothing nothing if the abuse or neglect was assumed to be a one-time event unlikely to occur. The family may also refuse in-home services, and the agency would then have to decide whether to file a court petition to require such services ↩︎
States must provide to National Child Abuse and Neglect Data System (NCANDS) information on how many children receive “postresponse services,” meaning services after a child protection investigation. But unfortunately, “postresponse services” includes foster care and provides a duplicated count, counting children every time they are the subject of an investigation, so it is not useful in telling us how many children receive in-home services. ↩︎
State foster care data can be accessed from https://www.acf.hhs.gov/cb/report/trends-foster-care-adoption. According to the latest information, the ten states with the largest number of children in foster care on September 30, 2022 were California, Florida, Texas, Illinois, Ohio, New York, Missouri, Pennsyhlvania, Arizona, and Indiana. ↩︎
I am honored to publish this essay from Christina Faucett. Christina has been a licensed foster parent in the state of Washington for six years and has adopted one child from the foster care system. Prior to becoming a foster parent, she was a CASA for three years. She is currently a member of the DCYF Parental Advisory Group and is passionate about fixing what is broken in our child welfare system to keep Washington kids safe. She lives in the Seattle area with her husband and daughter. You can follow her on X at @DCYFWAtch.
In 2023, the Washington State Department of Children, Youth, and Families (DCYF) completely rewrote their Caregiver Report to Court form. This form is the only voice foster parents have in the dependency process, since they are not parties to the case, and thus are not entitled to receive legal counsel, file motions, read pleadings, or speak in court unless called on by the judge. Given this, one might expect that changes to the caregiver report form would by preceded by extensive communication and feedback from caregivers as part of the editing process. This did not happen.
I first became aware of these changes in the fall of 2023 when I was provided the new form to submit in my foster child’s dependency case. I then reached out to connections I had in DCYF to ask how these changes had come about, and who had participated in the process of editing the form. After being stonewalled by DCYF employees, I submitted a Freedom of Information Act (FOIA) request, the results of which I finally received a couple of weeks ago.
My FOIA response revealed that the committee convened by DCYF to make the changes to the caregiver report to court included only one caregiver. However, it included three representatives of birth parents, including one former birth parent who had a child in foster care, a parent attorney and a social worker from the Office of Public Defense (which represents and provides assistance and advocacy for birth parents in dependency cases), along with other court and DCYF employees, and one CASA representative. At no point were caregivers informed of this committee’s existence, invited to participate on the committee, or asked to give feedback on the committee’s proposed changes.
The only foster parent representative on the committee works with Amara’s Family Connections Program, which encourages foster parents to maintain relationships with biological parents. Although this foster parent is a representative for what is called the “1624 Consultation Team” (named for the bill that created the group), which is a group of elected foster parent representatives who are supposed to raise the questions and concerns of foster parents in meetings with DCYF, no other 1624 representatives appear to have been informed of the pending changes. The Foster Parent Association of Washington also does not appear to have been informed of the pending changes. An August 2, 2023 post to their website states, “This seems to have been a sudden change and not everyone in the system is aware of it.”
Adding to the confusion, DCYF released two different Caregiver Report to Court forms, a long form and a short form. However, the forms have some completely different questions. For example, “Are you maintaining open and viable communication with the child’s biological parent?” is only included in the short form, not the long form. Even after an entire year of work on this by the committee, the reports still have numerous typos and errors. The new report was released with instructions that caregivers could submit it to the child’s CASA, not just their social worker, even though the CASA program in some counties did not want this responsibility and refused to submit the forms to the court on behalf of caregivers.
While not all of the changes to the caregiver report form are bad, a quick look makes it clear that DCYF is trying to limit input from foster parents to information that supports reunification, while simultaneously diminishing their opportunity to highlight their own relationship with the child (whom they may have raised for years, possibly from birth).
Some examples of changes:
A question soliciting caregivers’ thoughts on the Department’s case plan has been replaced with a question asking “Do you have any additional information that may help reunite the child or youth successfully with their biological family?”
A general question about how the child’s visits with parents are going has been replaced with, “What’s working well with family time? Explain.”
Other changes imply that caregivers have obligations they do not have. For example: “How have you included the parents of the child in the medical and dental appointments?” It is the social worker’s responsibility, not the caregiver’s, to inform parents of medical/dental appointments. The communication question mentioned above likewise implies that caregivers have an obligation to communicate directly with biological parents. Caregivers may have many legitimate reasons (including privacy and safety reasons) not to communicate directly with birth parents.
The old form had two questions about the child’s relationship with the caregiver and adjustment to living in the caregiver’s home. On the new long form these questions have been replaced with one question which is relegated to the bottom of the form under “additional information.” The short form doesn’t even ask caregivers about their relationship with the child living in their home; it only asks about the child’s behavior in the home. A question asking caregivers to “Describe child or youth’s interactions with positive adults (i.e., coaches, teachers, church, mentors, other relatives)” is given higher billing on the long form than the questions about their relationship with their primary caregiver.
DCYF has lost around 800 licensed foster homes since 2019, and since their six-month pause on issuing all new foster parent licenses from November 2022, to April 2023, the number of unfilled emergent placement needs has skyrocketed. If DCYF wants to achieve their goal of eliminating short-term stays for foster children and youth in offices and hotel rooms by December 2024, they need to start treating caregivers with the respect they deserve, not trying to further stifle their voices.
Greetings to my faithful readers! I’m trying out a different format for Child Welfare Monitor–a monthly newsletter format that highlights events and information that catch my eye. I’m not ruling out a single-issue piece now and then, particularly when there is a major new report or data source to discuss and analyze. Please let me know what you think of the new format. If you can think of a more exciting title than “Child Welfare Update,” let me know. And if you do find this to be a useful resource, please share it with your colleagues.
Adam Montgomery convicted of Harmony Montgomery’s death
In December 2021, Manchester, New Hampshire Police announced the disappearance of Harmony Montgomery, who would have been six years old if she were alive. We learned that Harmony’s noncustodial mother, Crystal Sorey, had called the police a month earlier to say that she had not seen or heard from her daughter since April 2019, two-and-a-half years earlier. The country was rapidly transfixed by the search for Harmony. We soon learned that the little girl, who was blind in one eye, had first been removed from Sorey at the age of two months by the Massachusetts Department of Children and Families (DCF) due to Sorey’s substance abuse. Harmony’s father, Adam Montgomery, was in jail at the time. Harmony was returned to her mother at seven months, and removed again at ten months. At almost three years old, and after two straight years in foster care with the same family that fostered her from the start and wanted to adopt her, Harmony was returned to her mother for the second time. At age three-and-a-half, Harmony was removed from her mother for the third time. Since Harmony was first removed, Adam Montgomery had been released from prison and begun visiting her. In February, 2018, a judge awarded Montgomery immediate custody of Harmony, without waiting for an assessment of his wife or a study of his living situation in New Hampshire.
A shattering report by the Massachusetts Child Advocate revealed the many missteps by all the professionals tasked with keeping Harmony safe. The OCA concluded that “Harmony’s individual needs, wellbeing, and safety were not prioritized or considered on an equal footing with the assertion of her parents’ rights to care for her in any aspect of the decision making by any state entity.”
Two years after the search for Harmony began, Adam Montgomery has been convicted of her death, thanks to the testimony of his wife. She told prosecutors that after Harmony soiled her bed at night he beat her viciously on the head in the morning of December 9, 2019 and again that afternoon in the car when she soiled herself once more. He then injected opioids and ate fast food as Harmony died of her injuries in the back of the car. He concealed Harmony’s body for months until renting a U-Haul and dumping her remains somewhere outside Boston. Her body has never been found. Montgomery is already serving 32 1/2 years in prison for another case and I hope he will never see the light of day, but what about all the professionals who failed to prioritize Harmony’s needs? And what has Massachusetts done to ensure that there will be no more Harmonies? The adoptive parents of Harmony’s brother have been speaking out; I assume Harmony’s foster parents are too devastated to do so, but their hearts must be broken.
Race trumps child welfare I: Black children don’t get attached?
Harmony Montgomery’s case illustrates, among other things, what happens when the importance of attachment for young children is disregarded. Attachment theory, which is widely accepted and taught in classes on psychology, social work and human development, posits that a strong attachment is central to the development of infants and affects their brain development and their ability to form relationships throughout life. The critical role of attachment in human development, which has been confirmed in mammals as well as humans, is the reason that the Adoption and Safe Families Act (ASFA) set a timeline requiring states to file for termination of parental rights after a child had spent 15 of the last 22 months in foster care. That is the deadline that Harmony’s team disregarded when they returned her to her mother after two years in foster care and continued to work with both parents after her return to foster care at the age of three-and-a-half. The continued disruptions were so devastating for Harmony that her foster parents, according to the OCA, could no longer meet her needs when she was placed with them for the third time, and asked that she be transferred to a specialized therapeutic home.
But some lawyers that counsel parents in child protection cases are being told that attachment theory does not apply to Black children. In Race Trumps Child Welfare, Naomi Schaefer Riley calls attention to a paper called “The Weaponization of Whiteness in Child Welfare,” originally published by the National Association of Counsel for Children. The paper calls attachment theory a “tool to justify the separation of families” and a manifestation of “racism in psychology.” The authors take aim at professionals who utilize attachment theory to argue for the adoption of Black children by White foster families who have raised them from infancy rather than returning them to their parents or placing them with kin. They argue that a Black child who has lived with a White foster family for the entire two-and-a-half years of his life should be placed with a relative who has never even seen the child. Black families, they say, belong to a collective culture, which emphasizes the needs of the group as a whole over the needs of an individual. Thus, any suffering to an individual child, they imply, is justified by the gain to the group–though it is hard to understand how Black people as a whole gain from the traumatization of young Black children.
Race Trumps Child Welfare II: ABA “addressing bias in medical mandated reporting” in Michigan
The American Bar Association (ABA) has announced that its Center for Children and the Law is piloting a new initiative in Michigan “to address overreporting by medical professionals of Black, Indigenous and Latino/a children to the child welfare system.” Without a footnote, the ABA reports that “injuries in Black children are 9 times more likely than those in White children to be reported as abuse despite evidence that child abuse and neglect occur at equal rates across races.” (Italics are mine.) Equal across races? I wonder what data they are using. While I am the first to acknowledge that maltreatment substantiation rates may not reflect actual incidence of abuse or neglect, evidence suggests that the two-to-one Blsck-White difference in child maltreatment substantiation rates is likely an understatement, not an overstatement. Moreover, Latino children nationwide are not reported to CPS disproportionately to their share of the population.
The pilots, funded by the Children’s Bureau, will use a “multisystem approach developed by the ABA’s Stop Overreporting Our People (STOP) project” to “address each decision made from the time a medical provider has a concern about maltreatment through child welfare hotline report and investigation to the decision of the judicial officer to remove the child from the home.” In Michigan, according to Child Maltreatment2022, of the 174,000 referrals to the hotline in Federal Fiscal Year 2022, about 68,000 were screened in, about 139,000 children received an investigation or alternative response (down 12 percent from the previous year), and 23,500 were substantiated as victims of abuse or neglect–a whopping 37.7 percent drop over the previous year. Of those “victims,” a total of 2,760 or 11 percent were placed in foster care–along with an additional 956 children who were not substantiated as victims but may have been siblings who were deemed to be equally endangered. Despite the precipitous drops in investigations and substantiations and the very low proportion of children substantiated as victims that were placed in foster care, the ABA isn’t satisfied…or doesn’t bother to look at data. The Michigan pilots will also focus on how doctors are trained to report maltreatment, according to the ABA. Discouraging doctors from reporting the signs that they are uniquely trained to spot may not strike all readers as a good idea.
Where was CPS?
Utah:Abuse in plain sight: Ruby Franke, a parenting influencer who achieved fame by promoting her strict parenting style, was sentenced to up to thirty years after pleading guilty to aggravated child abuse of two of her children. Franke rose to prominence with a youtube channel called 8 Passengers (now taken down) that documented her life with her husband and six children and was criticized for promoting abusive discipline methods. She eventually formed a business partnership with another woman named Jodi Hildebrandt, who encouraged and participated in the abuse of Franke’s children. Both women were arrested in August 2023, after one of Franke’s children escaped the home and ran to a neighbor’s house asking for food and water. The neighbor noticed the child’s open wounds, duct tape around his ankles and wrists and emaciation and called the police. After the arrest, the oldest daughter posted on social media that: “We’ve been trying to tell the police and CPS for years about this, and so glad they finally decided to step up.” “Several of us tried to help,” one neighbor told the Salt Lake Tribune. “I know people left food on doorsteps knowing the kids might not be eating; I know people were making phone calls to DCFS, to the police — people really did try and care. No one was looking the other way.”
New Mexico: $5.5 million settlement reached in eight-year-old girl’s brutal death: The Santa Fe New Mexicanreports that the New Mexico Children Youth and Families Department (CFYD) has agreed to pay $5.5 million to the brother and half-siblings of Samantha Rubino, acknowledging that it placed Samantha and her brother in the care of a man (Juan Lerma) with a history of child abuse and domestic violence, who had been investigated once before for abusing her and had not seen either Samantha or her brother for two years. Samantha died of blunt force trauma to the head, and Lerma placed her body in the trash. This is the latest in a series of big-money settlements by CYFD, funded by the taxpayers. New Mexico’s system is in crisis, with a backlog of 2,000 investigations of abuse and neglect. Is it too much to hope that the legislature will decide it is better to spend money up front to keep children safe than to pay massive settlements to their survivors?
The march continues to remove protections for homeschooled children
The powerful homeschool lobby continues its crusade to eliminate the few regulations that still exist to protect homeschooled children. In Nebraska, LB 1027 would eliminate two of the three minimal documents required for homeschool enrollments. It would bar school districts and Health and Human Services from investigating educational neglect in a homeschool setting. And it would give one parent the power to make homeschooling decisions without input from the other parent. The unicameral legislature’s Education Committee heard testimony from the Nebraska Christian Home Educators Association, the president of a Christian homeschoolers’ co-op, and another homeschooling parent. There was no testimony against the bill. The Education Committee has recommended the bill, and it is headed for a floor vote.
In West Virginia, legislators have tried to bar abusive parents from homeschooling ever since an eight-year-old girl named Raylee Browning died of sepsis, possibly caused by drinking toilet water, in 2018. Teachers had called CPS multiple times because Raylee was constantly hungry and covered in bruises. To avoid further problems, her guardians removed her from school for the ostensible purpose of homeschooling, thus enabling them to torture ber to death without interference. Every year since 2019, legislators have introduced Raylee’s Law, which would prohibit homeschooling if the parent or home educator had a pending investigation for child abuse or neglect or had been convicted of abuse, neglect or domestic violence. This very modest bill, which probably wouldn’t even have saved Raylee because her guardians did not have a pending investigation when they withdrew her from school, nor were they convicted of abuse, has never gotten through the legislature. This year it was voted down in the Education Committee by 15-5 after several legislators outlined their concerns–such as the fear that it would force children to enter public school before an investigation could be completed!
This year, the sponsors of Raylee’s Law managed to get a version of the legislation included in a bill that removes certain testing requirements for homeschooled children, and it passed by a voice vote. Unfortunately the amendment that passed was watered down further from the original bill, which itself was very weak The amendment that passed requires that a parent cannot withdraw a child for homeschooling if there is a pending child abuse or neglect investigation. But if the complaint is not substantiated within 14 days, the superintendent must authorize homeschooling. And the bill to which it was attached (HB 5180) reduces protection of homeschooled children by removing the requirement that parents submit academic assessments for homeschooled children in certain grades, as well as the requirement that the parent or home educator submit evidence that they have a high school or post-secondary degree.
Readers who care about the protection of homeschooled children and the drastic disproportion of power between homeschooling parents and advocates for their children should give to one of my favorite organizations, the Coalition for Responsible Home Education. They are doing their best on a shoestring budget, but they can’t afford to go to every state where protective legislation is threatened.
From the “Are you kidding me?” department
“Safe Haven laws” are a way for new parents who are not ready to raise a child to surrender their newborns safely without any questions or legal consequences. The laws exist in all 50 states. The Committee to Eliminate Child Abuse and Neglect Fatalities has endorsed these laws as a way to protect vulnerable infants and recommended that they be amended to extend the age of protected infants to age 1 and to expand the types of safe havens allowed. And it turns out that this option has existed in Europe since Pope Innocent III required churches to install “Foundling Wheels” in 1198!
In New Mexico, mothers are told they can anonymously surrender their infants through “safe haven baby boxes” located around the state. But recent media coverage from local stations KRQE and KOB4 has revealed the state’s Children Youth and Families Department (CYFD) has been investigating these surrenders–because they are required to do so by the state’s safe haven law. CYFD Secretary Teresa Casados told KRQE that “state law requires CYFD to investigate to ensure the mother was not forced to give up her baby, to make sure she is safe, and to inform the father of the child as well.” (She was apparently not asked what would happen if the father had raped or abused the mother.) She also explained that the Indian Child Welfare Act (ICWA) requires CYFD to look into each case and notify “all the tribes and pueblos” to ensure they are following the Act’s requirement that placement with a Native family be preferred. It is not clear that any other state has interpreted ICWA this way. New Mexico legislators rushed to draft legislation to retain the right of mothers to surrender their infants safely and anonymously, but the short session ended before a bill could be passed.
Never underestimate a persistent child advocate
John Hill, the Investigative Editor at Civil Beat, a nonprofit news outlet in Honolulu, Hawaii, has never given up on his quest to find out how a six-year-old girl named Ariel Sellers was placed with Lehua and Isaac Kalua, the adoptive parents who tortured her, culminating in her murder two-and-a-half years ago. The Kaluas have been charged with murder and abuse of both Ariel and her then 12-year-old sister, among other charges. The prosecution alleges that Ariel was kept in a dog cage and denied food, and that Lehua Kalua caused her death by duct-taping her mouth and nose. For more than two years, according to Hill, the Hawaii Department of Human Services has stonewalled in accounting for its actions in the adoption of Ariel, who was renamed “Isabella Kalua” by her adoptive parents. But Hawaii’s Public First Law Center, motivated by a series of columns written by Hill, has filed a motion to receive the foster and adoption records for Ariel and her siblings. Now Hill is asking uncomfortable questions about the January 2024 death of 10-year-old Geanna Bradley, who was also allegedly tortured and starved to death by her adoptive parents.
In a bizarre twist, the Honolulu Star Advertiser has reported that the Kaluas have retained custody over Isabella’s three sisters, who were removed from the home in September 2021. But apparently the state of Hawaii hasn’t moved to terminate the parental rights of the Kaluas. A special master appointed to oversee the interests of Ariel’s sisters is concerned that the failure to terminate the rights of the Kaluas will interfere with efforts to find permanent families and educational opportunities for the girls. (And already has, I would think!)
The guaranteed income craze continues
At its February oversight hearing, the Director of the District of Columbia Child and Family Services Agency announced a forthcoming grant from the Doris Duke Foundation to a guaranteed income for some low-income families. The announcement was greeted with congratulations from the Council Chair who referenced the great results from the recent Strong Families, Strong Futures pilot, which provided 132 new and expecting mothers with $10,800 in the course of a year. I don’t know where she got her information. An article in the Washington Post reported on interviews with three of the mothers participating in the pilot. One of the mothers took the money as a lump sum. Setting aside about $5,000 for essential expenses, she used the remaining money on a $6,000 trip to Miami preceded by the purchase of new clothes, shoes, gadgets and toys for all of her three children and a $180 hair and nails treatment for herself. Another mother decided to spend $525 on a birthday party for her one-year-old, who clearly couldn’t appreciate it. Program coordinators said that the mothers reported spending most of their funds on needs such as housing, food and transportation. But I’m not sure how I feel as a DC taxpayer to see my money spent in ways that I personally find wasteful, nor am I sure that allowing such spending provides appropriate training in how to budget scarce resources. Such no-strings-attached money giveaways might not be the best use of taxpayer money, even if foundations choose to support it.
And the prize for cynical use of data goes to….
Kentucky! The State’s Cabinet for Health and Family Services (CHFS) is crowing about Kentucky’s drop from the highest rate of child maltreatment “victimization” to number 13 among the 50 states and the District of Columbia. In a statement reported by Spectrum News1, CHFS said this improvement “demonstrates the efforts made by the Department for Community Based Services and its many partners to increase the provision of child welfare prevention services and reduce child abuse and neglect within the Commonwealth.” But child advocates and family court judges are not convinced, citing a longstanding problem with hotline workers screening out cases that should be investigated–exacerbated by the adoption of an actuarial screening tool at the hotline in April 2022. The report quotes two family court judges and a CASA program director who linked child deaths to the failure to investigate prior reports involving the same families. According to one judge, “The alarm has to be sounded because I’m not joking when I say children are perishing in the state of Kentucky because of this ‘Structured Decision Making’ tool….'” The judges are right. One has only to look at Kentucky’s commentary in the Children’s Bureau’s report, Child Maltreatment 2022.
An overall decrease for child victims was observed between FFY 2021 and FFY 2022. Kentucky has worked diligently over the past several years to implement a safety model which includes the implementation of SDM® Intake Assessment Tool and a thorough review and modification of the state’s acceptance criteria to ensure a focus upon children and families with true safety threats versus risk factors. This shift in the approach to the work may have contributed to the decrease in child victims this year.
Children’s Bureau, Child Maltreatment 2022, p. 13
In other words, they changed the screening criteria to screen out more cases and voilà! Fewer child victims! Amazing! The percentage of referrals that was screened in decreased from 45.5 percent in 2021 to 39.9 percent in 2022, and the maltreatment substantiation rate decreased from 14.9 to 12.3 per thousand children during the same period. But both of these rates have been decreasing since FFY 2018, so more factors than the new screening tool are likely responsible. It’s unlikely that a decrease in actual maltreatment is among them.
The placement and workforce crises continue
Every month brings another crop of articles on the intertwined placement and workforce shortages plaguing child welfare. February’s news on the placement crisis included a story from Texas Public Radio reporting on the release of hundreds of incident reports about “Children Without Placements” in the state from 2021 to 2023. They include stories of children squaring off to fight each other in the hallway of a Houston hotel that resulted in the hospitalization of one youth. These incidents, occurring at a rate of about two a day, often involved injured staff, injured youth, and calls to police.
In a state that requires some social workers to supervise youths in hotels and other unlicensed placements, its not surprising that about one in four caseworkers left the job in January, according to the head of the Department of Family and Protective Services (DFPS). And even workers who don’t have to supervise unruly youths are dealing with untenable caseloads and terrible working conditions. Some states are taking action to attract and retain workers. The Governor of Maine announced a series of three one-time lump-sum payments of $1,000 to recruit and retain child welfare workers. Let us hope it is enough to reduce the state’s high caseloads.
And now for some good news: efforts to keep siblings together
It’s always nice to read about people who see a need and create a program to meet it. February brought news of two new “foster care villages” to house larger sibling groups, an idea I have promoted in the past. In California, the actor Christian Bale achieved a dream he has nurtured for 16 years–breaking ground on Together California, a new foster home community in Palmdale, Los Angeles County. The project will include a dozen foster homes built to accommodate up to six siblings and staffed by full time, professional foster parents. A 7,000-square foot community center will offer academic, therapeutic, social, and recreational activities for young people in the foster homes and the surrounding community, which is very short on such resources.
In South Carolina, a new foster care “village” called Thornwell is transforming old houses built about 100 years ago to house foster families and large sibling groups. Two homes are in use, a third is under renovation and more homes await renovation provided the funds and parents can be found. Foster parents will pay one dollar of rent per month and receive free utilities. Children will be eligible for Thornwell’s early learning center, charter school, and recreational facilities. Here’s hoping for more programs like Together California and Thornwell!
By Antonio R. Garcia, Jill Duerr Berrick, Melissa Jonson-Reid, Richard P. Barth, John R. Gyourko, Patricia Kohl, Johanna K.P. Greeson, Brett Drake, and Victoria Cook
A note from Child Welfare Monitor (CWM): CWM welcomes submissions from authors who represent points of view that are more evidence-based and child-centered than what is typically presented by leading media outlets and other child welfare publications. We are privileged to share this commentary from an illustrious group of child welfare scholars from schools of social work and social policy around the country. While this essay does not mirror the views of CWM in every detail, we share the authors’ basic premise regarding the need to reform, rather than abolish, the child welfare system.
Over the past couple of years, while teaching classes, presenting lectures, or offering invited talks and workshops, students and participants have inquired about the need to abolish the child welfare system. Some have questioned whether they should continue their pursuit of a career in this field. They are aware of the growing calls by abolition advocates, particularly UpEND and JMac for Families, to completely eradicate child welfare services, despite offering no evidence as to its likely impact on child safety or permanency.
Abolition advocates have successfully convinced a few scholars, an unknown number of students, and a surprising number of community members and decision-makers that child protective services must be eliminated. Acting on briefs supplied only by activist groups, the United Nations has even called for all major child welfare laws in the United States to be repealed or replaced.
Why? The narrative built by the abolitionists includes two major parts: First, classist and racist bias largely determines who has contact with the child welfare system, with poor children as well as Black and Native American children being routinely and unnecessarily harassed. The resounding narrative–largely offered by lawyers, not child welfare scientists–is that the interventions and intentions of child welfare services and its staff are inherently racist (e.g., Roberts, 2022). Some child maltreatment scholars (e.g., Briggs et al., 2023) have even gone so far as to reiterate Roberts’ claim that the modern child welfare system (CWS) was intentionally designed as a mechanism of racial oppression. This conclusion flies in the face of history as documented child welfare historians (e.g., Myers, 2004). Purveyors of this narrative ignore efforts like those of pioneering African American women pursuing the development of child welfare facilities for African American children who were routinely insufficiently served by family and community (Peebles-Wilkins, 1996); they fail to mention the work of the Children’s Defense Fund, and a diverse coalition of policymakers, who helped to shape the modern CWS through their work to expand family preservation and support services. Nor do they acknowledge that the Title IVE program was, in part, explicitly developed to extend equal protections to Black children (Hutchinson & Sudia, 2002).
Second, those who denigrate child welfare services argue that CWS interventions do more net harm than good, and for that reason should be abolished. Child welfare services are said to sever familial connections (Roberts, 2022), and unjustifiably surveil children and families (Gruber, 2023). To that end, they argue that the best way to protect children and families is to abolish the current system and replace it with family and community-based responses (Kelly, 2021). This proposed alternative to CPS is remarkable for the degree to which it is vague and undefined. Nothing approaching a concrete plan for such a system has ever been suggested to our knowledge. Given the historical lessons of relegating unwanted or abused children to orphanages, orphan trains, indenture, or detention centers, it is difficult to point to an example of American communities fully embracing the care of children whose parents are unable to care for them.
The abolition movement sidelines any past record of successful reforms of child welfare or hope for future evidence-based or incremental change. Anxious, perhaps, that reforms have been uneven or too slow, the proponents of abolition do not suggest improving the complex and intricate web of local, state, and national child welfare policies that have been developed over the last 40 years. Critically, their proposals have no evidence base. Instead, they rely on ideology that disregards the best available evidence (Barth et al., 2020).
The degree to which the abolition narrative is taken seriously is troubling. Child safety is contingent upon training qualified professionals to respond to signs of abuse and neglect – and ensuring institutions have the resources to recruit and support them. Tuition is covered for many social work students if they agree to “repay” their time by working for the state’s child welfare system after graduation. The premise is to promote and retain a highly educated, culturally responsive child welfare workforce and prepare them to rely upon critical thinking skills and the best available evidence to promote child safety and permanency. With many states facing unheard-of staff shortages following the pandemic, the additional decrease in interest in the field is distressing.
1) receiving and responding to community signals about risk or harm to children;
(2) assessment of need coupled with a proportionate response;
(3) rights protections to ensure fairness and equity when placement outside the family is required; and
(4) procedures for accountability and quality improvement.
Without these key elements, we contend that children will be left in peril. Many community members will not know how to respond to signs of risk and harm to children. The progress we have made in the last few decades toward developing, implementing, and evaluating prevention and early intervention services to address trauma and promote healing will be disrupted. Supports for foster parents, kin, and child welfare staff will be disbanded. The elimination of court oversight will eliminate rights protections for parents, children, and extended family. Racial inequities in economic hardship will make it more challenging for communities of colorto develop responses, which will likely yield an even larger gap in unmet needs for children of color.
Still, many in our field are challenged by having to choose between abolition and reform. At the core of this debate, we are contending with the interplay of science, practice, ideological beliefs, and conflicting values. What types of evidence are or should be used to guide our decision-making? How do we best balance the support of families with a child’s need for safety without defending the status quo? Said another way, we see no reasonable likelihood that abolishing child welfare services would result in a world where families are better supported to provide care that is not injurious to their children and children are better protected from the harsh realities of child abuse, including fatalities.
The debate offers an opportunity to examine current practice and whether it advances the needs of vulnerable children and families. We underscore in our paper that current services and funding are inadequate. To that end, we delineate alternative pathways to abolition providing some practical, evidence-informed recommendations, including but not limited to the following:
Create a robust family support and prevention infrastructure outside of Child Protective Services (CPS);
Reduce poverty and financial hardships through universal basic income supports and targeted economic supports for families in great need;
Resume the child welfare waivers program to expand and test innovations in case finding and response to family needs; and
Continue to improve alternative systems for reporting less serious concerns and connecting families to existing resources to reduce the number of families who are subject to unwarranted CPS investigations.
As discussed in our paper, we believe implementing these recommendations offers a holistic roadmap for (1) improving outcomes for all children and families and (2) mitigating racial inequities in exposure to economic hardship and access to services and programs.
Although many jurisdictions have a long way to go in fully aligning practices with our valued principles, the child welfare system, on the whole, has made much headway. We have made progress toward reducing foster care entries, enhancing permanency, supporting youth who must emancipate from care, and developing alternative response paths for less severe cases. The number of children in foster care is now lower by more than 175,000 children than it was in 1991, despite population growth (US DHHS, 2022; US DHHS, 2000).
We have made advances in the development and implementation of evidence-based, and culturally appropriate parenting programs, and there are innovative approaches to screening and collaboration with other systems such as family drug courts and other models that are being adopted around the country. Research indicates that families are better served by caring and competent child welfare staff. At a minimum, this means we need trained child welfare professionals to determine if abuse or neglect are occurring and how best to provide services to mitigate risk factors. If removal to foster care is required, trained social work and legal professionals need to be engaged in reunification services and the determination if it’s safe for children to go home.
Finally, it is critical that these efforts are continuously evaluated. Abolition would end the now-routine national reporting of the number of victims of child maltreatment, and their characteristics (i.e., NCANDS; Children’s Bureau, 2023). We would not know if new family- and community-based approaches were helpful or harmful, particularly for the families of color for whom both reformists and abolitionists are concerned. State-level systems that track the provision of services and outcomes would also end, meaning that trends in family needs and gaps in response systems would likely go undetected. We would also lack data to influence policy to end harmful practices and expand funding for effective prevention and intervention services.
As we note, “it is difficult to imagine how eradicating the only structures that exist to address this issue [child maltreatment] would result in any outcome other than jeopardizing the safety and well-being of children as well as reducing accountability to the families that CWS [the child welfare system] serves.”
This is a contentious moment in the journey to create opportunities and healing for all children and families. We hope our message conveys a sense of urgency to engage in critical, evidence-informed practice and policy – and to reflect upon how values, biases, and morals can impact decision-making. The famous words of Nelson Mandela may be instructive: “There can be no keener revelation of a society’s soul than the way in which it treats its children.” In efforts to enhance practice and policy, we need child welfare professionals to gain the skills, cultural humility, self-efficacy, and motivation to ensure children live lives free of violence and abuse. Policymakers need to stay grounded in the pathway that has led to significant improvements in child welfare services and rely on research-based reforms. Our children deserve nothing less.
References
Barth, R. P., Jonson-Reid, M., Greeson, J. K. P., Drake, B., Berrick, J. D., Garcia, A. R., Shaw, T., & Gyourko, J. R. (2020). Outcomes following child welfare services: What are they and do they differ for Black children?. Journal of Public Child Welfare, 14(5), 477-499. https://doi.org/10.1080/15548732.2020.1814541
Briggs, E., Hanson, R., Klika, J. B., LeBlanc, S., Maddux, J., Merritt, D., … & Barboza, G. (2023). Addressing systemic racism in the American Professional Society on the Abuse of Children publications. Child maltreatment, 28(4), 550-555.
Children’s Bureau. (2023). National Child Abuse and Neglect Data System (NCANDS). U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families. https://www.acf.hhs.gov/cb/data-research/ncands
Gruber, T. (2023). Beyond mandated reporting: Debunking assumptions to support children and families. Abolitionist Perspectives in Social Work, 1(1). https://doi.org/10.52713/apsw.v1i1.12
Hutchinson, J.R. (2002). Failed child welfare policy: Family preservation and the orphaning of child welfare. Washington DC: Child Welfare League of America.
Kelly, L. (2021). Abolition or reform: Confronting the symbiotic relationship between ‘child welfare’ and the carceral state. Stanford Journal of Civil Rights & Civil Liberties, 17(2), 255–320. https://heinonline.org/HOL/P?h=hein.journals/stjcrcl17&i=271
Peebles-Wilkins, W. (1996). Janie Porter Barrett and the Virginia Industrial School for Colored Girls: Community response to the needs of African American children. In E Smith and L Merkel-Holguin (Eds.), A history of child welfare. Washington, DC: Child Welfare League of America.
Roberts, D. (2022). Torn apart: How the child welfare system destroys Black families, and how abolition can build a safer world. Basic Books.
U.S. DHHS. (2022). The AFCARS Report. Washington, D.C.: Administration for Children and Families.
U.S. DHHS. (2000). The AFCARS Report. Washington D.C.: Administration for Children and Families.
A note from Child Welfare Monitor: It is a privilege to publish this important essay by Judith Schagrin. Judith earned an undergraduate degree from the University of Pennsylvania and a master’s degree in social work (MSW) from the University of Maryland School of Social Work. She unexpectedly found her passion in public child welfare, and more specifically, foster care after helping start an independent living preparation program for young people in care. After a decade as a foster care social worker specializing in adolescence in a large Maryland county department of social services, she supervised two different units before becoming the county’s director of foster care and adoptions, serving in this position for twenty years. She also worked part-time for the Agency’s after-hours crisis response for a decade. For almost 10 years, she served as a respite foster parent for a private foster care agency, and since 2008, has mentored a young person who aged out of care in California and came east for college. In 2001,with a little help from her friends, Judith founded Camp Connect, a weeklong sleepaway camp to reunify brothers and sisters living apart in foster care and provide memorable experiences siblings can share for a lifetime. For the past 23 years – one year virtual – she has spent the week at Camp Connect immersed in the care of Maryland’s foster children and youth.
The closing of children’s mental hospitals in the 1980s, the subsequent closure of detention centers leaving foster care to take up the slack, the movement to shutter all group homes and residential treatment programs and the prohibition of out-of-state placements have created a slow-motion train wreck whose results could have been predicted easily at every new chain in the sequence. Those results include children and youth staying in psychiatric hospitals long after being ready for discharge, “boarding” in emergency rooms and “placed” in hotels at a cost of $30,000 to $60,000 per child per month. From my 35-year vantage point as a caseworker, supervisor, and then running foster care and adoptions in a large Maryland county, I’ve had a front row seat to the evolution of this crisis and the failure to come up with real solutions.
Deinstitutionalization
The first in a series of events that created this crisis occurred in the 1980s, when the deinstitutionalization that began for adults in the 1960’s with the civil rights movement expanded to include children. Until then, youth remained in state hospital facilities for as long as a year or even more. The closure of those state facilities led to the expansion of Medicaid-funded residential treatment centers (RTC’s), that stepped in to provide the longer term care once provided in the state hospitals. In turn, group homes proliferated to meet the needs of youth discharged from RTC’s. The advent of Medicaid was instrumental in expanding prIvate psychiatric treatment options, including hospitals. But over time, Medicaid stopped funding even 30 days of treatment, limiting payment to only a few days of crisis intervention.
Today, many youth, especially older youth, are entering foster care not because of what we traditionally think of as maltreatment, but due to parental incapacity or unwillingness to care for them due to acutely problematic behavior, and behavioral health and/or developmental needs. Services to meet these needs are often missing or inadequate, and parents of children with high-intensity needs cannot find residential treatment except through the child welfare system. Medicaid doesn’t pay for treatment and care in a group home of any kind; access in Maryland requires the child welfare system’s physical or legal custody.
New approach to juvenile justice
In the early 2000’s, a series of Supreme Court decisions brought welcome changes to juvenile justice and shifted the country from the ‘get tough’ approach of the ‘80’s and 90’s to the ‘kids are different’ era. Moving from punishment to rehabilitation and minimizing detention in favor of community services makes sense on both humanitarian and neuroscience grounds. But it meant that youth who once fell under the purview of Juvenile Services now required child welfare intervention when parents or other caregivers were unwilling or unable to continue to provide care. The mother evicted from four apartments because of her son’s property damage; the grandmother who stepped in years ago and is no longer able to cope with her granddaughter after the third vehicular misuse charge and chronic episodes of running away; or a parent with younger children afraid that an older sibling known to have rages and episodes of violence will harm his siblings, are examples of desperate caregivers I have come across.
In Maryland, the first alarm that child welfare was ill-equipped to care for these youth was sounded in 2002 by local department directors in a memo to the head of the Department of Human Services. Closing detention centers was a good thing, but alternatives weren’t developed for those youth unable to live at home, and no resources were provided to help child welfare accommodate its new clients. As the closure of state psychiatric facilities and detention beds was widely celebrated, the belief that every youth had a family eager and able to provide a home was more than a touch naive, as would soon become clear.
Group home closures
Another domino fell in the early 2000’s, when group homes, many poorly administered with little oversight, became a scandal in Maryland. A series of articles in the Baltimore Sun exposed the flaws of many group care programs, and some were forced to close. With the scandals around bad group homes, the timing was perfect for state leadership, encouraged by a national advocacy group with deep pockets and the laudable dream of a family for every child, to lead a movement to shutter congregate care placements. Funding constraints, too, forced some providers out of business. Reimbursement rates did not keep up with costs, and some programs closed their doors due to inadequate reimbursement. The state lost roughly 450 beds in five or six years, including entire residential treatment center programs. Rate-setting ‘reform’, which began in October of 2021, will not be completed until July of 2026 if it stays on schedule.
At the same time group homes were being closed in Maryland, state agency leadership began to frown on out-of-state placements for youth with highly specialized needs when no placement in Maryland to meet those needs was available. Public officials with little understanding of placement resources pronounced these out-of-state placements to be evil incarnate, and an overwhelming number of bureaucratic obstacles made them nearly impossible.
With the loss of group homes as an option, we were urged to ‘re-imagine’ care for children, yet discouraged from developing individualized plans of care because insufficient flexible funding was allowed to make that happen. We’re fond of slogans in child welfare, as if words will change outcomes, but too many initiatives are about clever slogans and not about substance. If only we would review every child in group care, we were told, we would realize how many had other options. With consultation from the national advocacy group, we spent hours seriously poring over the needs of our children in congregate care and attempting to find matches with kin or foster families. Not at all surprising to our staff, “low hanging fruit” didn’t exist.
We also initiated a rigorous “Family Finding” practice, in hopes of finding kin willing to become providers with services and supports. What we learned is that youth in congregate care had already exhausted family and “kin of the heart” resources. Today it’s not clear that public officials and child welfare leaders grasp that children and youth wouldn’t be in hotels if there were any kin – fictive or otherwise – willing and able to provide care, or if parents could and would be a safe resource.
Youth with intensive, complex needs
As other doors closed, the child welfare system became increasingly tasked with providing residential behavioral health care for children and youth with high-intensity and complex needs for supervision and treatment. The differences between those involved with the juvenile justice system (and may have gone to detention centers in the past) and those who are not are often hard to discern. Both groups tend to engage in behaviors that pose a serious safety hazard to themselves or others. These behaviors may include physical violence; property damage; compulsive self-harm such as cutting or swallowing objects; chronic truancy; frequent runaway episodes; sexual victimization of siblings; aberrant sexual behaviors such as public masturbation; molesting younger siblings; participating in petty crimes; harming family pets; and generally oppositional and dysregulated behavior.
Contrary to the popular notion that the public child welfare system is tearing families apart, these are children whose families are typically frustrated, exhausted, and often eager to place their child. Some even view foster care as a much-needed punishment, imagining that when the youth is ready to “behave,” they can return home. Of course these young people have many strengths to be nurtured, but they need intensive supervision and therapeutic intervention by professionals trained to evaluate and address their special needs and work with families.
The gist of the matter is that we are serving two different out-of-home placement populations with very different needs. One is a younger population in foster care primarily due to maltreatment stemming largely from parental substance abuse and/or untreated mental illness. The other is older youth with complicated behaviors, and behavioral health needs and/or developmental disabilities. The parents and kin of the older group are asking for placement, not objecting to it, and are typically worn out and adamantly opposed to more in-home services. In spite of the stark differences in these two populations, our policymakers and those upon whom they rely have failed to recognize their needs are not the same.
In Maryland and other states, treatment, or ‘therapeutic,’ foster care stepped in to accommodate this new population of older, harder to serve foster youth. To some extent this approach has been effective as an alternative to congregate care, but it’s not the panacea some would like to believe. The desperate need for foster families willing to care for these youth means there’s a certain amount of pressure to lower expectations and even turn a blind eye to foster parents that do a less than stellar job. Tales of locked refrigerators and youth left sitting on the stoop at the end of the school day until the caregiver came home soon proliferated. However, we were told by representatives of a national advocacy group that, “Youth are better off moving from shabby foster home to shabby foster home than in the very best congregate care.” In my own experience, instability begets instability and there’s little more soul-sucking than being rejected from family after family.
Setting aside the question of quality, foster care, whether treatment or not, has great challenges recruiting homes for youth with weapons charges, those with a history of drug dealing, or whose parents have refused to pick them up from the police after another runaway episode. “Cutters” and “swallowers” need 24/7 supervision to keep them safe and in general, kin have already tried to provide care long before the child’s entry into state custody. With the closure of group homes and residential treatment centers in Maryland and the prohibition on out-of-state placements, finding placements willing to accept youth with high-intensity needs became literally impossible. As a result, for years now children have been left in psychiatric hospitals (sometimes for months) after “ready” for discharge, and others are ‘boarding’ in emergency rooms for weeks or months.
A failure to recognize reality
Instead of recognizing the lack of capacity to serve those youth with nowhere to go after being hospitalized, hospital representatives, public officials, and legislators blamed caseworkers for not ‘picking children up’, as though they were simply lazy and incompetent. “Advocates” proposed legislation imposing more caseworker accountability as the solution, as though if caseworkers worked harder and filled out more forms, placements that didn’t exist would magically appear. Fortunately, none of the legislation passed, but being a lonely voice trying to explain the source of the problem wasn’t lazy caseworkers or enough forms was painful. Public officials, leaders and advocates also clamored for more “prevention” services, not recognizing the acute needs of older youth developed over many years and that new services authorized today are not going to keep them safely at home.
During my 20 years as the director for my county’s foster care and adoptions program, I can’t count the nail-biting times we came close to not finding a placement for a child – but we were always able to pull something together. The state made funding available for a 1:1 staff person (or sometimes 2:1) we could offer existing providers, allowing us to use that as a bargaining chip. Of course, increasing reimbursement rates and staff salaries would have been far less expensive than millions for extra staff to support ill-equipped placements, but that change in fiscal allocation has yet to happen.
Five years have now passed since I retired, and hotel placements have become not a rarity but a regular necessity. At the rate of $30,000 to $60,000 per child each month (not including damages to hotels) to warehouse children in hotel rooms supervised by an untrained aide – one can only imagine what that kind of money could be doing productively for children. Caseworkers are overseeing the most precarious and risky “placements,” and being ‘hotel reservation clerks’ isn’t the reason competent social workers choose to do the work. We’ve all heard the tales of youth stealing their 1:1’s car; or youth locking themselves in their rooms doing what we don’t know; a youth who overdosed on his medication; parties taking place with the acquiescence of the 1:1; youth harassing guests; and the youth who leaped over the reservation desk to try to steal cash.
Over the years there have been many, many meetings among high ranking state officials and others; ironically, these meetings didn’t include the experienced and knowledgeable child welfare staff responsible for the children. Lots of strategies, goals, and plans too – a personal favorite was the goal of instructing local department staff on hospital discharge planning, as if they weren’t already experts. Despite all the meetings and all the hand-wringing, progress meeting the needs of the children in our care, or soon to be in our care when parents abandon them at the hospital or elsewhere, has been negligible. Years that could have been spent on developing and promoting new model programs have been wasted. In the meantime, Congress saw fit based on testimony from well-heeled advocacy groups to pass the Family First Prevention Services Act, which limited congregate care even more by restricting funding to approvable options based on criteria seemingly pulled out of a hat.
Today, the deepening and pervasive placement crisis is affecting nearly every state and attracting media attention around the country. Given the financial resources dedicated to keeping children in hotels, finances clearly aren’t the issue. And it certainly isn’t about quality of care, since hotel rooms, overstays in hospitals, and boarding in emergency rooms rank far below a quality congregate care program as a suitable home for a child.
What is to be done?
In the short run, Maryland and other states need respite programs for young people awaiting placements in hospitals, emergency rooms, and hotels. In the long run, we must acknowledge child welfare’s responsibility not only for maltreated children, but also those with high-intensity needs for supervision and treatment once served by other child-serving organizations. We need to bring the finest minds together to reimagine how residential care is provided, and its role in the continuum of child welfare resources to meet the needs of older youth entering foster care because of needs related to behavioral health and/or developmental disabilities. That process should include some of the scholars who have been studying the use of congregate care in other countries where it is more highly valued as a treatment and a professional field. Exploring the development of real alternatives to congregate care is also a worthy investment. Finally, the unintended consequences of the Family First Prevention Services Act that disincentivized needed placements without a credible replacement must be remedied.
How many more years until we wake up? And how many children will have to be harmed? A colleague had a quote in her office that stays with me always, “when we are doing something with somebody else’s child we wouldn’t do with our own, we need to stop and ask ourselves why.” Who among us would consent to our own children boarding in emergency rooms, on overstay at hospitals, or ‘placed’ in hotel rooms? If that’s not okay for our own children, it shouldn’t be okay for the children in our state’s custody either.