“Child Maltreatment Victims Have Decreased for the Past Five Years to a New Low,” proclaimed the Administration for Children and Families (ACF) as it released Child Maltreatment 2022, its long-awaited annual compendium of child maltreatment data shared by the states. Contrary to the headline, the report says nothing about the actual incidence of child abuse and neglect. It does show that in Federal Fiscal Year 2022, calls to child protective services hotlines almost rebounded to pre-pandemic levels. But the number of investigations and assessments that CPS undertook in response to these calls did not bounce back as much as calls, and states are confirming even fewer allegations of maltreatment as they did in FFY 2021 and 2022. Moreover, child fatalities are up for the fifth year in a row. Some of the most striking and interesting results are discussed below, though this is not an exhaustive summary of the report’s contents.
Referrals and Reports
The annual Child Maltreatment reports, produced by the Children’s Bureau of ACF are based on data that states submit to the National Child Abuse and Neglect (NCANDS) data system, and this latest report concerns Federal Fiscal Year (FFY) 2022, which ended on September 30, 2022. NCANDS uses the term “referrals” to connote contacts to child protective services (CPS) hotlines. In 2020, the number of referrals dropped sharply as schools closed and children vanished into their homes. In FY 2021, with some opening of schools and society, the referral rate rose slightly but was still much less than in FFY 2019. But in FFY 2022, the referral rate bounced back to 58.6 per 1,000 children, bringing it close to the rate of 59.7 per 1,000 in FFY 2019. Some states mentioned in their commentaries that the pandemic continued to suppress referrals somewhat in FFY 2022, which began in October 2021. That fall and winter in particular, there were still temporary school building closures and increases in absenteeism due to big waves of infection. This continued pandemic effect may help explain the failure of referrals to reach their 2019 level.

As usual, the state-by-state tables document huge differences in referral rates, from 21.1 per 1,000 children in Hawaii to 180.7 per 1,000 in Vermont. Vermont reports in its commentary that its very high referral rate reflects that the state counts all calls to the hotline as referrals, suggesting that most states do not do so. And indeed, Connecticut and Alabama report that none of the calls that are assigned to alternative response are included in NCANDS, resulting in a far lower number of calls than the number they actually receive. Louisiana reports that some referrals are neither screened out nor accepted; these are calls related to open investigations or in-home or out-of-home service cases; it appears that these are not counted as referrals at all. These inconsistencies between states make it difficult to interpret state-by-state differences in referral rates.
Once a state agency receives a referral, it will be screened in or out by hotline staff. In general, referrals are screened out if they are deemed not to contain an allegation of child abuse or neglect, contain too little information to act on, are more appropriately assigned to another agency, or for some other reason do not fall under the mandate of the child welfare agency. In NCANDS, a referral becomes a “report” once it is screened in, and it then is assigned for an investigation or alternative response. The 47 jurisdictions that reported both screened-in and screened-out referrals collectively reported screening in 49.5 percent of referrals and screening out 50.5 percent. The national screened-in referral rate was 29.0 per 1,000 children, an increase of one percentage point from the rate in FFY 2021. In that year, as shown in Child Maltreatment 2021, the 46 states reporting screened in 51.5 percent of referrals and screened out 48.5 percent. So as the number of referrals increased, it appears that the states screened in a lower percentage of them.
State by state differences in the percentage of referrals that are screened in were vast; ranging from 16.9 percent of referrals to 98.7 percent in Alabama. But as discussed above, differences in which calls are reported in NCANDS will affect these percentages, making the data hard to interpret. Some of the very high rates reported, such as the 98.7 percent for Alabama, and Texas’s reported 84.5 percent, are hard to understand.
Indiana’s commentary provides an example of how a state can purposely reduce its screen-in rate. The state reported that the Department of Children’s Services “partnered with the Capacity Building Center for States as well as ran internal events targeted at reducing our screen-in rate.” Added to the types of allegations to be screened out during FFY 2021 were “sexting concerns among adolescents,” “pre-adolescent children exhibiting potentially sexually maladaptive behaviors,” and “educational neglect.” Some child advocates might be concerned about excluding these types of allegations, as all of them could indicate serious problems in the home, and the exclusion of educational neglect is particularly surprising. Perhaps the changed screening guidelines are one reason the number of Indiana children receiving an investigation or alternative response fell from 139,343 in 2020 to to 123,644 in 2022, a decrease of 11.6 percent.
Screened-in Referrals by Referral Source
Before the pandemic, teachers were the most common source of screened-in referrals, submitting 21 percent of all referrals that were screened in in FFY 2019. They lost that position in FFY 2020 with the pandemic school closures, while legal and law enforcement personnel increased their share of reports. It is not surprising that teachers did not recoup their leading role in 2021, since many students were still attending school virtually for some part of the year. But even in 2022, legal and law enforcement personnel still submitted slightly more screened-in referrals than education personnel–21.2 percent of screened-in referrals compared to 20.7 percent for education personnel. Medical personnel submitted 11.2 percent of referrals and social services personnel 9.8 percent. Because these data are available only for referrals that are screened in, they reflect both the number of referrals each group submits and the extent to which they are screened in. It seems likely that teachers submit more referrals than law enforcement but that their referrals are more likely to be screened out.

Child Disposition Rates: The “Footprint” of CPS
In every state, screened-in reports may receive an investigation, which results in a determination (or disposition) about whether or not maltreatment has taken place. Some states assign some reports (often those deemed to be lower risk) to an alternative track (often called “alternative response” or “family assessment”) that does not result in a formal disposition as to whether maltreatment occurred and who was the perpetrator. ACF calls the proportion of children receiving either an investigation or an alternative response the “child disposition rate.” This is an important indicator, because it can be seen as a measure of the “footprint” of CPS–the number of children it actually touches.
For FFY 2022, an estimated 3,096,101 children, or 42.4 per 1,000 children, received an investigation or alternative response, as shown in Exhibit S-1 of the report, reproduced above. That rate has dropped 12.7 percent since FFY 2018. Not surprisingly, the biggest drop was during the pandemic, but it dropped again in 2021 and rose by only one percentage point from 41.4 in FFY 2022, remaining significantly lower than before the pandemic.
The diversity in child disposition rates across states is striking. Disregarding the 15.0 in Pennsylvania, which excludes most neglect cases from NCANDS,1 this rate ranges from a low of 17.1 per 1,000 children in Maryland to a chilling 131.3 in West Virginia (over one out of 10 children!). The opioid crisis and its catastrophic effects on children in West Virginia has received considerable media attention. It is worth noting that West Virginia’s child disposition rate has decreased from 143.2 in FFY 2018. Below West Virginia, Arkansas and Indiana have similar child disposition rates of 79.9 and 78.8 respectively, far above the next group of states at about 66. The five states with the lowest child welfare “footprint,” (other than Pennsylvania) are Maryland, Hawaii, South Dakota, Connecticut and Louisiana.
Some states or jurisdictions, including Alaska, Arizona, the District of Columbia, Indiana, Kentucky, Maryland, Montana, North Dakota, Rhode Island, and South Carolina, had very large decreases in their disposition rates between FFY 2021 and FFY 2022. These may reflect purposeful policy changes to reduce the role of child welfare (such as Indiana’s addition of categories to be screened out), but it may also affect other factors such as the workforce crisis that is affecting child welfare in most states.
CPS Workforce Data and Child Disposition Rates
Child Maltreatment 2022 also provides interesting data on state child welfare workforces although the quality of the data is impossible to assess. Table 2-4 of the report provides the CPS caseload, which is obtained by dividing the number of intake, screening, investigation and alternative response workers by the number of “completed reports,” meaning reports with a disposition. That is not a very meaningful number, because it leaves out all the alternative response cases, while the workers who handle these cases are included in the numerator. In order to get a better sense of the number of children seen by each worker, I divided the number of children receiving an investigation or alternative response by the number of workers in the 20 states with the highest populations, minus the four states that did not provide workforce numbers–Florida, Georgia, New York and Ohio, as well as Pennsylvania.1
Among the 15 states in the table below, there is a staggering variation in the number of children per worker, which ranged from 21.1 in Wisconsin to 199.4 in Indiana. As child welfare commentator Dee Wilson explains in an unpublished analysis, “Differences of this magnitude develop over time when policymakers do not staff child welfare systems in accordance with workload standards.” We must also keep in mind that we do not know if the data are truly comparable between states.
Children Per Worker, FFY 2022

“Victimization”
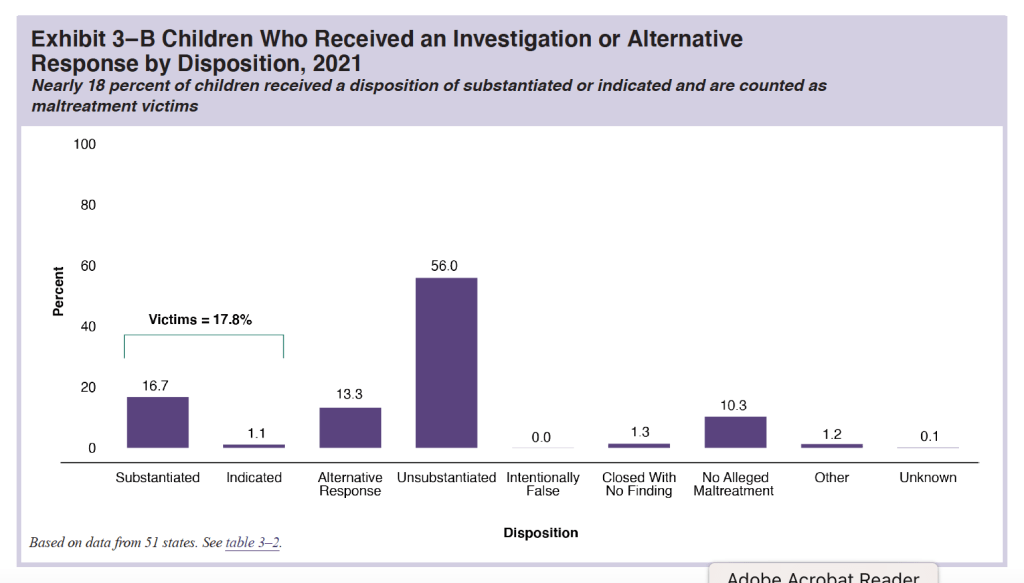
An investigation can result in a variety of dispositions, depending on the state. Most states use the term “substantiated” to indicate that the allegation was verified, but some states use another term, usually “indicated.” In NCANDS, a “victim” is defined as “a child for whom the state determined at least one maltreatment was substantiated or indicated; and a disposition of substantiated or indicated was assigned for a child in a report.” A reader might think the terms “victim” and “victimization” reflect the true number of children who experienced abuse or neglect. But there are many reasons they do not provide such a true count. Many cases of child maltreatment go unreported. Children assigned to alternative response will not be found to be victims unless their case is reassigned to the investigation track. And finally, substantiation is not an accurate reflection of whether maltreatment occurred. Adults can lie, children can lie, perhaps when coached by adults, the youngest children are nonverbal or not sufficiently articulate to explain what happened or didn’t, and making a determination of whether maltreatment occurred is difficult. So it is not surprising that research suggests that substantiation decisions are inaccurate2 and a report to the hotline predicts future maltreatment reports and developmental outcomes almost as well as a substantiated report.3 For all of these reasons, it is widely recognized that the number of children estimated to be victims of maltreatment is likely an underestimate. And over time, events such as the coronavirus pandemic or changes in state policies can be confounded (innocently or cynically) with actual changes in child maltreatment victimization. For that reason I generally put quotes around “victimization” or replace it with “substantiation,” and use the terms “substantiated victims” or “children found to be victims of maltreatment” instead of “victims.”
The 2022 report provides an estimate of 558,899 substantiated victims of maltreatment, or 7.7 per 1,000 children, down from 8.2 in FFY 2021. States differed greatly in the “victimization rates” that they found in FFY 2022. Of course these differences can stem from the factors mentioned above, as well as from actual maltreatment. The number of substantiated victims per 1,000 children ranged from 1.6 in New Jersey to 16.5 in Massachusetts. We know that New Jersey has been intent on reducing CPS involvement in the lives of families, no doubt encouraged by its effort to exit a class action suit monitored by the Center for the Study of Social Policy, one of the founders of the upEND movement to abolish child welfare. So its low victimization rate is not surprising (An article by Sarah Font and Naomi Schaefer Riley discusses the New Jersey experience in more detail.) New Jersey’s “victimization” rate has dropped by more than half since FFY 2018.
The number of children found to be victims of maltreatment has declined every year since FFY 2018. The change in state “victimization rates” between FFY 2018 and FFY 2022 ranged from a 48 percent decrease in Kentucky to a 14.5 percent increase in Nevada over those five years. Many things could explain these changes other than an actual change in maltreatment, including policy changes made by state legislatures or agencies. Two of the largest states made it more difficult to substantiate maltreatment in FFY 2022, and both found a decline in the number of maltreatment victims. In Texas, the legislature narrowed the definition of neglect, requiring the existence of both “blatant disregard” for the consequences of a parent’s action or inaction and either a “resulting harm or immediate danger.” Perhaps this helps account for the drop in the number of substantiated victims from 65,253 to 54,207. In New York, the level of evidence required to substantiate an allegation of abuse or neglect was changed from “some credible evidence” to “a fair preponderance of the evidence.” The number of victims found in New York dropped from 56,760 to 50,056. States reported other reasons for changes in their rates of “victimization,” including changes in the use of alternative response, new screening and intake tools, reduction in investigation backlogs, and the continued effects of the pandemic.
It is instructive to look at the changes in the number of referrals, screened-in referrals, child disposition rates, and child “victimization rates” between FFY 2021 and FFY 2022, as the nation came out of the pandemic. Thinking about the process as a funnel starting with referrals and ending with victims, we can see that the effect of the increased referrals is further attenuated at each stage. While the number of referrals increased from 4,010,000 to 4,276,000, an increase of 6.6 percent, the number of screened in referrals increased only 3.3 percent. The number of children receiving an investigation or alternative response increased by only 2.0 percent. And the number of children substantiated as victims decreased by a whopping 7.2 percent. It’s just another way of describing what we have already seen–that the child welfare system’s response is not keeping up with the public’s renewed reporting activity.

Demographics and “Victimization”
Younger children are more likely to be substantiated as maltreatment victims. The likelihood of being a substantiated victim of maltreatment is is more than twice as high for an infant younger than one than for a two-year-old, and drops a bit with every one-year increase in age. Girls are more likely to be substantiated as victims than boys, with a rate of 8.2 per 1,000 children, compared to 7.1 for boys. This is probably related to sexual abuse; girls are the overwhelming majority of victims of substantiated sexual abuse, as shown in Exhibit 7-F of the report.
In terms of race and ethnicity, American Indiana and Alaska Native children had the highest rate of substantiation as a victims, at 14.3 per 100,000 children, followed by Black or African-American children with a rate of 12.1 per 100,000 children. The rate for Hispanic children was 7.0 per 100,000 and for White children it was 6.6 per 100,000. Again, the number of substantiated victims is not equal to the number of actual victims. These rates reflect the extent to which these children are reported to CPS, the referrals are screened in, and they are substantiated. If, as many assert, there is systematic bias affecting referral, screening, and investigation, then the total number substantiated will also reflect that bias.
Victimization Rate per 1,000 children by Race and Ethnicity, FFY 2022
- American Indian/Alaska Native: 14.3
- Asian: 1.3
- Black or African-American:12.1
- Hispanic: 7.0
- Native Hawaiian/Pacific Islander: 9.3
- Two or more races: 9.4
- White: 6.6
The claim that these rates are biased has resulted in a movement to eliminate racial disproportionality in child welfare or even to eliminate child welfare itself, as promulgated by the upEND Movement. However, evidence confirms that the Black-White difference in substantiation rates is actually less than the disparities in other indicators of child risk and adversity. A group of prominent child welfare researchers led by Brett Drake estimated the “expected rate” of being reported to CPS, using several categories of risk and harm that are known to be highly correlated with the risk of child abuse and neglect, such as poverty, single-parent families, teen birth rate, very low birth weight, and homicide. Drake et al. reported that the disparity in all the measures of risk, and in all of the measures of harm except accidental deaths, were greater than the disparity for CPS reports, as measured by NCANDS. In other words, there was a greater disparity in risk and harm to Black children compared with White children than there was in CPS reporting. Thus, given their likelihood of being abused or neglected, Black children appear to be reported to CPS less than White children, not more. And even when adjusted to account for confounding factors, Black children are less likely to be substantiated (and placed in foster care) than White children. So if anything, the “victimization rates” provided in CM 2022 may underestimate the true disparities in child maltreatment substantiation of Black and White children.
CM 2022 also provides information on the number of substantiated victims with different maltreatment types. Three-quarters of the substantiated victims, or 74.3 percent, were found to have experienced neglect, 17 percent physical abuse, 10.6 percent sexual abuse, 0.2 percent sex trafficking, and another 3.4 percent another type of maltreatment. (These percentages add up to more than 100 because some children were found to be victims of more than one type of maltreatment during the year.) As shown in Table 3-9 of the report, some states diverged from the pattern that substantiated allegations are for neglect–and instead found more (or almost as many) children to be physically abused than neglected. These states include West Virginia, where 76.2 percent of substantiated victims were found to have suffered physical abuse; Vermont, (58.6 percent); Tennessee (51.8 percent), Alabama (53.5 percent), South Carolina (47.5 percent), and Ohio, with 46.6 percent.5 Corporal punishment often opens the door to physical abuse, some of these states are in regions where corporal punishment is known to be more prevalent. But the absence of Mississippi on this list (with only 16.0 percent of victims substantiated for abuse) and the presence of Vermont are surprising. Perhaps liberal Vermont is simply reluctant to find neglect in cases associated with poverty; only three percent of its victims were found to be neglected. And perhaps in Mississippi, a state that allows corporal punishment in the schools, the standard for finding abuse is may be high.
Substantiation by Reporting Source
Chapter 7 of CM 2022 contains an interesting table plotting the number of substantiations for each reporting source. We have seen that legal and law enforcement personnel made only slightly more screened-in reports than education personnel in FFY 2022: Table 7-3 of the report shows that each group made approximately 21 percent of the reports that were screened in. Yet the reports made by law enforcement personnel accounted for 38 percent of the substantiated victims, and the reports of educators accounted for only 11 percent of the substantiated victims. So reports from law enforcement personnel were over three times more likely to be substantiated than reports from teachers. Medical personnel did better but not quite as well as the police: they made 11 percent of screened-in reports, which accounted for 13 percent of substantiated victims. An analysis by The Imprint shows that social services personnel have a slightly higher share of substantiated reports than of total reports, while nonprofessionals have a substantially lower share. The data align with increasing criticisms of teachers as making too many reports that do not rise to the level or abuse or neglect. Whether that is true, or whether reports from teachers are automatically devalued because of their source, cannot be ascertained from this information.
Fatalities Continued to Increase
CM 2022 reports an estimated increase in child maltreatment fatalities for the fifth consecutive year. The report provides a national estimate of 1,990 children who died of abuse or neglect in FFY 2022 at a rate of 2.73 per 100,000 children in the population. That number has increased every year since 2018, and the 2022 estimate is a 12.7 percent increase over the estimate from 2018. The increase in child fatalities started before 2018; Child Maltreatment 2017 reported an 11 percent increase in child fatalities from 1,550 in FFY 2013 to 1,720 in FFY 2017. That amounts to a 28 percent increase between FFY 2013 and FFY 2022.

There are many caveats to be made about year-to-year comparisons of child fatalities. First, there is nearly universal agreement among experts that the annual estimates of child fatalities from NCANDS dramatically undercount the true number of deaths that are due to child maltreatment. As CM 2022 states, some child deaths may not come to the attention of CPS at all. That can happen if nobody makes a report, perhaps because there are no surviving children in the family, or if the family is not already involved with CPS. For this reason the Child and Family Services Improvement and Innovation Act (P.L. 112-34) requires states to describe in their state plans all the sources used to compile information on child maltreatment deaths, and to the extent that information from state vital statistics departments, child death review teams, law enforcement agencies and medical examiners or coroners is not included in that description, to explain why that information is not included and how it will be included. Most states that comment on fatalities report using at least some of these sources, but the extent to which they are capturing actual fatalities is unclear. Only Virginia reports that it does not collect child fatality data from external sources.
Second, the fatalities reported in the 2022 report did not all occur in 2022. The report explains that child fatalities reported in CM 2022 are generally those that were determined to be due to maltreatment in 2022, not those that actually occurred during 2022. That is because It may take more than a year to find out about a fatality, gather the evidence (such as autopsy results and police investigations) to determine whether it was due to maltreatment, and then make the detrmination. Some states report that the deaths they reported may have occurred as long as five years before 2022. However, each state has its own way of determining which fatalities to report. California, for example, explains that the fatalities reported in the 2022 report were actually fatalities that occurred in FFY 2021 and were known to the state by December 2021, meaning that the estimate is truncated.
The meaning of the increasing fatalities is not obvious. Just like “victimization,” the classification of a death as a maltreatment fatality depends upon whether the fatality was even reported to the child welfare agency as well as whether the correct decision was made to substantiate the fatality as due to maltreatment. As mentioned above, states are supposed to gather the information about fatalities from other sources like medical examiners, but the extent to which they are receiving this information, and the extent to which these other sources are identifying maltreatment, is unclear.6
From the explanations that some states provided in their commentaries, it appears that annual maltreatment fatality counts can reflect a variety of factors. Year-to-year changes are often attributed to random fluctuations due to small numbers or timing issues. In their commentaries, states often explained a year-to-year jump by explaining that many children in one family died, or or that a large group of fatalities that occurred the previous year were reported in the current year.
Some states reported on societal issues that have contributed to increasing child fatalities over time. For example, Washington’s commentary suggests that the opioid crisis has contributed to its increase in fatalities from 19 in FFY 2021 to 31 in FFY 2022. The state reports that between FFY 2021 and FFY 202 the percentage of child fatalities in the state that were due to opioid ingestion or overdose rose from less than one percent to 23 percent of child fatalities. Of the deaths and near-fatalities that qualified for a review because they occurred in families touched by the system in the previous year, that percentage jumped from 28 to 44 percent. Ohio reported that it attributes the increase in child fatalities to an increase in the overall death rate due to violence. Other states commented on the type of deaths that have increased, such as unsafe sleep coexisting with substance abuse.
Changes in how maltreatment fatalities are defined can also affect fatality counts, and in the case of Texas, the change resulted in a decrease in child fatalities from 206 in FFY 2021 to 176 in FFY 2022. Specifically, Texas attributes this decrease to the new law that makes the definition of neglect more stringent. Considering that the new law requires both “reckless disregard” of the consequences of parental action or inaction and actual harm, and given that death is certainly harm, this suggests that those investigating the deaths did not consider that the parents or caregivers exhibited such reckless disregard. Texas reports that deaths from unsafe sleep, drowning, and vehicle-related fatalities declined in FFY 2022 under the new definition of neglect.
Some states attribute increases in reported fatalities to improvements in the accuracy with which they report child fatalities. Commentaries from states that experienced an increase in child maltreatment fatalities in recent CM reports include accounts of their improvements in their ability to identify such deaths. These included several states that reported an increased awareness of unsafe sleep practices and hot car deaths resulting in more reports involving these cases, the creation of a Special Investigation Unit that investigates child fatalities to determine whether they are due to maltreatment (Mississippi); requiring mandated reporters participating on child fatality review boards to report suspected maltreatment fatalities to the local child welfare agency (Ohio); the development of capability to track fatalities at report, during investigation, or in care (Maine); ensuring that documentation of deaths is included in the states CCWIS system (Maryland); increased training of staff and partners on reporting child fatalities (Texas); and implementation of death review panels (Arkansas). Therefore, it is not possible to determine the extent to which the increase in reported child maltreatment fatalities reflects better identification, more maltreatment deaths, or a combination of the two.
Demographics and child maltreatment fatalities
Infants under a year old are more than three times more likely to die of maltreatment than one-year-olds, and the fatality rate generally decreases with age. In contrast to the different rates of substantiated abuse or neglect, boys have a higher maltreatment fatality rate (3.26 per 100,000 boys) than girls (2.25 per 100,000). Black children have by far the highest fatality rate of all the groups for whom information was available; 6.37 per 100,000 black children died of substantiated maltreatment, compared to 3.37 for American Indian or Native American children, 1.99 for White children, and 1.68 for Hispanic children. The maltreatment fatality rate for Black children is over three times as high than the rate for White children, a difference that is even more stark than the difference in the “victimization rate,: which is twice as high for Black children than for White children.

The question of bias has to be addressed again when talking about fatalities from maltreatment. It is theoretically possible that racial bias could play a role in whether a fatality is substantiated as maltreatment. But it is likely that there is less opportunity for bias when it comes to fatalities, as the fact that harm was done cannot be disputed even if the parent’s role may be unclear. Drake et al. found that in 2019 indicators of risk and harm for Black children are usually between two and three times greater than those for White children, while the Black-White homicide disparity was four times as great as that for White children. So while we cannot rule out any role for bias, it is unlikely to be the main cause of the disparities in child maltreatment fatalities.
The data showed that most of the perpetrators of child fatalities were caregivers; more than 80 percent of child fatalities involved “one or more parents acting alone, together, or with other individuals.” NCANDS does not collect the official cause of death, but it does ask for the type of maltreatment that was substantiated in each fatality. Thus, one child can be found to have suffered more than one type of maltreatment, though it is not clear that each maltreatment type that was substantiated must have contributed to the fatality. Over three quarters (76.4 percent) of the children who died were found to have suffered from neglect, and 42.1 percent were found to have endured physical abuse.
It is worth noting that CM 2022 was originally released on or about January 8 without a press release and then disappeared from the internet for about three weeks. It is hard to avoid speculating about the reasons for the removal of CM 2022 and then its publication several weeks later. Could it be that officials were trying to figure out how to spin the five years of increase in fatalities? When the press release finally appeared along with the restored report, ACF had elected to basically recycle last years headline, New Child Maltreatment Report Finds Child Abuse and Neglect Decreased to a Five-Year Low. Once again, the press release failed to explain that victimization is not actual maltreatment. It did mention the increase in child maltreatment fatalities and, surprisingly, did not raise the possibility that better measurement contributed to this increase, which might have helped their case.
In the press release, Children’s Bureau Associate Commissioner Aysha Schomberg is quoted as encouraging “agencies to pay particular attention to data in this report that is disaggregated by race.” There is something perplexing about this suggestion. Paying attention to race means observing the stark disparities in child maltreatment “victimization” and fatal child maltreatment, between White children and Black and Native American children. ACF and its allies at Casey Family Programs, the Center for the Study of Social Policy and other like-minded organizations typically argue that these disparities are not due to different rates of maltreatment but to racial bias built into the system. But ACF’s press release accepts these “victimization” rates as a true indicator of child maltreatment, which suggests that the racial disparities in child maltreatment are real. And if that is indeed the case, as I believe it is, isn’t the right answer to protect Black and Native American children through a stronger and better-functioning CPS, rather than trying to weaken or abolish it?
ACF’s Communications team’s misuse of the term “victimization” to suggest that maltreatment is declining is disappointing in a government agency with a responsibility to inform the public. We will never get an accurate measure of child maltreatment because so much of it occurs behind closed doors. So what is the real meaning of CM 2022? The failure of the child disposition rate to keep up with the increase in reports suggests a decreasing response by child welfare to reports of maltreatment, with the slight uptick after the pandemic disguising a downward secular trend over the entire period. The continuing decline in substantiations despite the increase in referrals, while not indicative of declining maltreatment, shows even more clearly how child welfare systems are seeking to reduce their involvement with families. Could the increase in child fatalities be the consequence of this reduced involvement? It is possible, but the improvement of fatality reporting in some states makes it impossible to answer this question definitively.
Notes
- In Pennsylvania, referrals that involve non-serious injuries or neglect are assigned to General Protective Services (GPS), and information on these cases is not reported in NCANDS.
- Theodore Cross and Cecilia Casanueva, “Caseworker Judgments and Substantiation,” Child Maltreatment, 14, 1 (2009): 38-52; Desmond K. Runyan et al, “Describing Maltreatment: Do child protective services reports and research definitions agree?” Child Abuse and Neglect 29 (2005): 461-477; Brett Drake, “Unraveling ‘Unsubstantiated,'” Child Maltreatment, August 1996; and Amy M. Smith Slep and Richard E. Heyman, “Creating and Field-Testing Child Maltreatment Definitions: Improving the Reliability of Substantiation Determinations,” Child Maltreatment, 11, 3 (August 2006): 217-236.
- Brett Drake, Melissa Jonson-Reid, Ineke Wy and Silke Chung, “Substantiation and Recidivism,” Child Maltreatment 8,4 (2003): 248-260; Jon M. Hussey et al., “Defining maltreatment according to substantiation: Distinction without a difference?” Child Abuse and Neglect 29 (2005): 479-492; Patricia L. Kohl, Melissa Jonson-Reid, and Brett Drake, “Time to Leave Substantiation Behind: Findings from a National Probability Study,” Child Maltreatment, 14 (2009), 17-26; Jeffrey Leiter, Kristen A. Myers, and Matthew T. Zingraff, “Substantiated and unsubstantiated cases of child maltreatment: do their consequences differ?” Social Work Research 18 (1994): 67-82; and Diana J. English et al, “Causes and Consequences of the Substantiation Decision in Washington State Child Protective Services,” Children and Youth Services Review, 24, 11 (2002): 817-851.
- The ideal numerator would be the duplicated count of children who received and investigation or alternative response, because even if one child is investigated five times, each investigation needs to be counted. But CM 2022 does not provide that number, and I am assuming that there won’t be enormous differences in repeat responses by state.
- Pennsylvania also has a high percentage of abuse findings but that reflects the fact that it does not report General Protective Services cases in NCANDS.
- Each state submits both a child and an agency file. The Child File contains case-level data on reports that resulted in a disposition in the reporting year. The Agency File contains data that are not reportable at the child-specific level and often gathered from agencies external to CPS, like medical examiners vital statistics departments and child fatality review teams. Child fatalities can be included in the Child File, which means the entire record of the case from report to disposition is included (as well as any previous cases) or it can be included only as part of the aggregate total in the agency file. States must report as part of the Agency File the total number of victims who were not reported in the Child File, so that those that were reported are not double-counted.