Proposed federal budget cuts to child welfare services might hurt New Jersey’s recent progress in child welfare, the Commissioner of New Jersey’s Department of Children and Families told state legislators last month. The anticipated reduction of more than $100 million would force the department to “revert to its most basic role — that of child protection — not prevention, not support or empowerment, just surveillance and foster care,” DCF Commissioner Christine Norbut-Beyer told members of the state Senate’s Budget Appropriations Committee. The relegation of child protection–or “surveillance and foster care”–to the “most basic” version of child welfare is telling. DCF’s Commissioner, like many other progressive child welfare administrators, no longer views child protection as the primary purpose of child welfare services.
For those who regularly read this blog, the devaluation of child protection and foster care by a high-level administrator over child welfare will not be a surprise. There has been a sea-change in child welfare over the past decade. The mainstream view of the purpose of child welfare has shifted from responding to child abuse and neglect to “upstream prevention.” And why not? Why wait until children are abused and neglected if we can prevent the maltreatment altogether?
There is no denying that ideally, it is better to prevent maltreatment than to respond to it. But the services that are discussed as prevention are mainly in the province of other agencies. In seeking to broaden child welfare services through the Family First Act, Congress added mental health, drug treatment, and parenting training. While the latter can be seen as a function of child welfare, drug treatment and mental health are separate systems. There has been increased emphasis on cash and housing and other antipoverty benefits as child maltreatment prevention; we have large programs to address these problems–much larger than the child welfare system. Even some of the “prevention services” that DCF and other state agencies have adopted, like “Family Success Centers,” provide a wide array of place-based services, most of which do not fall into the traditional orbit of child welfare and would be most appropriately funded jointly with other agencies.
If “prevention” could abolish the need for child protection, then there would be no need for child protection agencies. But we know that no amount of “prevention” (at least as envisioned by today’s child welfare establishment) will eliminate child abuse and neglect. We are often talking about patterns of mental illness, drug abuse, family violence, and poverty that have persisted over generations. And then there are families that are not poor or characterized by generations of dysfunction but where a parent’s mental illness or disordered personality makes them incapable of safely raising children. As Jedd Meddefield describes in his brilliant essay called A Watershed Perspective for Child Welfare, “As critical as it is to fully consider upstream factors, it would be wrong not to do all we can to help children who lack safe families today.
But the fact is that many of today’s child welfare leaders like Norbut-Beyer appear not to be interested in child protection and foster care. They often disparage the “reactive” role of child protective services in contrast to the “proactive” nature of prevention. Many agencies have reactive missions–police, firefighters, emergency rooms–and one could argue these are the most important services of all because they save lives. The analogy with the police is revealing. Police react to allegations of crime just as child welfare agencies react to allegations of child abuse and neglect. To prevent crime, we must not rely on the police, who are overburdened already and not trained and equipped to provide the services needed. Instead we must turn to a whole host of agencies dealing with education, public health, mental health, housing, income security and more–the same agencies that we must mobilize if we want to prevent child abuse and neglect. Nobody is saying that the police need to address the underlying causes of crime.
Norbert-Beyer’s use of the word “surveillance” as a synonym for child protection is telling indeed. She clearly doesn’t see CPS investigators as heroes who go out in sometimes dangerous and certainly uncomfortable circumstances to protect children–and maybe even to save them. It’s not surprising because we have all been told that saving children is not what child welfare is about.1 And foster care? Norbert-Beyer boasts that New Jersey has the lowest rate of child removal in the country, and children who are removed more often than not go to relatives. She’s not very interested in the quality of care these vulnerable young people receive or in all the things her agency could do it improve it, like establishing foster care communities (like Together California) to house large sibling groups or investing in cutting-edge models of high-quality residential care.
When the person who is in charge of child protective services in a state that is acknowledged as a leader in the field calls it “surveillance,” and relegates it along with foster care to “basic” functions that hardly deserve mentioning, it’s hard to have faith that the crucial mission of child protection will be implemented with the passion it deserves. Norbert-Beyer’s comments illustrate the prevalent thinking that leads to the diversion of resources from crucially needed child protective services and foster care to “prevention services” that are and should be provided by other agencies.
See for example this statement from Casey Family Programs, which includes the words “We must continue to evolve from an approach that seeks to “rescue” children from their families to one that invests in supporting families before abuse and neglect occur.” One of the first messages I was given as a CPS trainee is that my job was not to save children. ↩︎
Family resource centers, also called family support centers or family success centers, are becoming the prevention program of choice for child welfare agencies around the country. These neighborhood-based centers are being touted as America’s best hope for preventing child maltreatment before it occurs. But the proponents of these centers have been a little too eager in their claims that these programs are supported by research. Two studies recently released to great fanfare do not stand up to close examination. The sites chosen appear to have been chosen for their potential to support the desired conclusion, the evaluations do not convincingly adjust for confounding factors (a major misstatement was made in one of the studies regarding the implementation date of a possibly confounding policy), and the studies are rife with methodological problems related to the measure of success and the attribution of outcomes to the programs.
According to the Child Welfare Information Gateway, family resource centers are “community-based or school-based, flexible, family-focused, and culturally sensitive hubs of support and resources that provide programs and targeted services based on the needs and interests of families.” These centers are known by different names around the country, including Family Centers, Family Success Centers, Family Support Centers, and Parent Child Centers. Services provided often include parenting support, access to resources, child development activities, and parent leadership development.
Family resource centers (FRC’s) are being heavily promoted by child welfare agency leaders, as well as influential private actors such as Casey Family Programs as “less punitive, more open-ended, flexible and voluntary venues where vulnerable families can connect to services, particularly in the communities sending the most children to foster care,” as a recent article in The Imprint put it. FRC’s are gaining increased support around the country. New York City recently announced that it would expand from three to thirty Family Enrichment Centers. In October 2021, the District of Columbia opened ten new Family Success Centers in 2021, under its “Families First DC” initiative. Texas has recently announced that it is investing $1 million to create an unspecified number of Family Resource Centers, and has announced the first five grantees. Many other jurisdictions, such as New Jersey, Vermont, and Allegheny County Pennsylvania, have been operating FRC’s for years. A national membership organization called the National Family Support Network (NFSN) represents and promotes these centers.
Two recent studies have drawn press attention with reports that two family resource centers have been very successful preventing child maltreatment and as a result are saving money for taxpayers. The studies were carried out by a Denver nonprofit called the OMNI Institute, “in partnership with” the NFSN and Casey Family Programs. The researchers report that they identified the two programs by contacting NFSN members and reviewing existing evaluations of FRCs “to identify potential opportunities that could serve as return on investment case studies.”
One of the two programs studied was the Community Partnership Family Resource Center (CPFRP) in Teller County, Colorado, a rural county in central Colorado with a population of approximately 25,000 that is almost all White. As described in their report, the researchers wanted to explore the impact of two new programs that the center implemented in 2014 and 2016, that they hypothesized might have the effect of preventing child abuse and neglect in the county. One of these programs was Colorado Community Response, a voluntary program for parents who were reported for abuse or neglect but were either screened out at the hotline level or investigated but received no child welfare services. A second program, Family Development Services, was a voluntary primary prevention program helping struggling families set goals and connect to resources. The researchers claim that the creation of Colorado Community Response and increased funding for Family Development Services offered “a potential opportunity to examine the Return on Investment for CPFRC to the child welfare system, by comparing child maltreatment outcomes prior to and after the establishment of these new practices.” They decided to use the number of maltreatment allegations that were “substantiated” (or found to be true upon investigation) as their outcome of interest.
In designing their study, the researchers sought to identify other changes that might also affect levels of child maltreatment in order to avoid confounding effects. They learned that Colorado had implemented a “differential response” model in 2013, which was a two-track model for addressing allegations of abuse or neglect. Allegations that are viewed as less serious are assigned to the alternative response track and usually do not receive a substantiation, or finding of abuse or neglect. Obviously, the change to differential response might dramatically affect the number of substantiations. The researchers identified several other policy changes and events that might have affected substantiations, such as the establishment of a statewide child abuse hotline and the inception of the COVID-19 pandemic. According to the report, they decided to use 2015 is the baseline year because “neither Colorado Community Response nor Family Development Services programming were available to the whole CPFRC population, but the statewide child abuse hotline and differential response models were in place.” They chose 2018 as the comparison year because it was the only year that both Colorado Community Response (CCR) and Family Development Services were fully implemented with no other major system-wide changes in place, and before a change in CCR eligibility requirements and the onset of the COVID-19 pandemic.
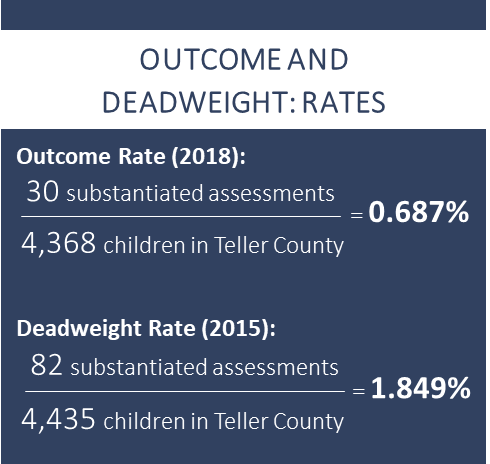
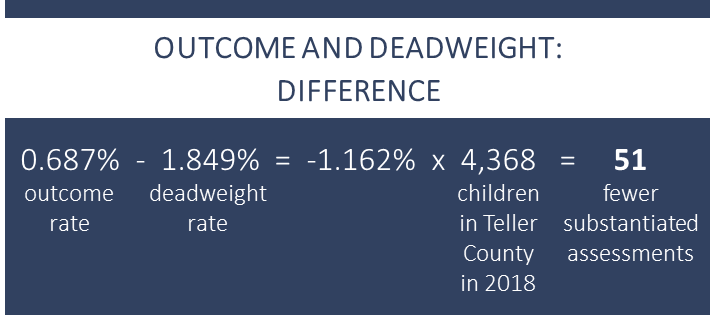
Using data provided by the state on its online dashboard, the OMNI researchers found that there were 82 substantiated assessments in 2015 and only 30 in 2018. To adjust for population changes they divided each number by the number of children in the County at the time, producing what they called an “outcome weight” for 2015 and a “deadweight rate” for 2018, as described in the first graphic below. Subtracting the deadweight rate from the outcome weight and multiplying by the child population in 2018, the researchers came up with a reduction of 51 fewer substantiated assessments in 2018, as illustrated in the second graphic. (The adjustment made little difference; simply subtracting the 30 from 82 resulted in a reduction of 52 substantiated assessments.) This impressive drop in substantiated cases translates to a “62.84 percent reduction in substantiated assessments from 2015 to 2018.”
The researchers used the estimated number of children served by CPFRC during 2018 (1,444) relative to the estimated number of children at risk for maltreatment based on income-to-needs (ITN) ratio (1,479)* and age (1,272), to decide how much of the change in substantiations to attribute to the program. The result was an “attribution estimate of 98 percent based on the ITN ratio and 114 percent based on age. Combining these estimates, the researchers decided to attribute the entire reduction in substantiated cases to CPFRC.
Finally, the researchers calculated a return on investment using total child welfare expenditures in 2018 divided by the number of substantiated assessments in that year, resulting in a total cost of $49,026 per substantiated investment. Multiplying that figure by 51, they concluded that the reduction of 51 substantiated assessments, (of which 100 percent were attributed to the program) saved the Teller County child welfare system $2,500,326 in 2018 compared to 2015. Dividing this total by $856,194, they came up with a “Return on Investment” of $2.92 for every dollar spent on the program.
There are many serious problems with this analysis. The choice of substantiations as an indicator of victimization is problematic because of the large body of literature illustrating the difficulty of determining if a child has been maltreated and the absence of differences in future outcomes between children with substantiated vs. unsubstantiated allegations. Allegations (or referrals) seem to be a more meaningful measure of abuse or neglect. Using data from two years without looking at the numbers for the years in-between is also problematic, as the researchers themselves admit. In their discussion of the weaknesses of the study, they acknowledge that using only two years, without the years in between, is not ideal because it provides a less robust understanding of changes in child maltreatment as well as making its estimates more susceptible to influence by other system-level factors.
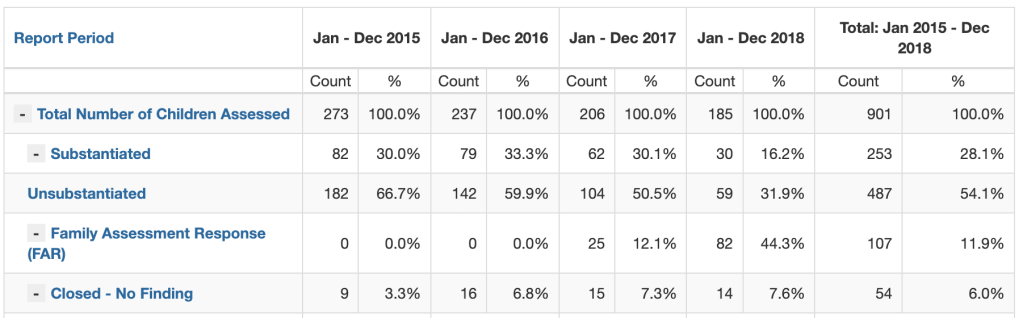
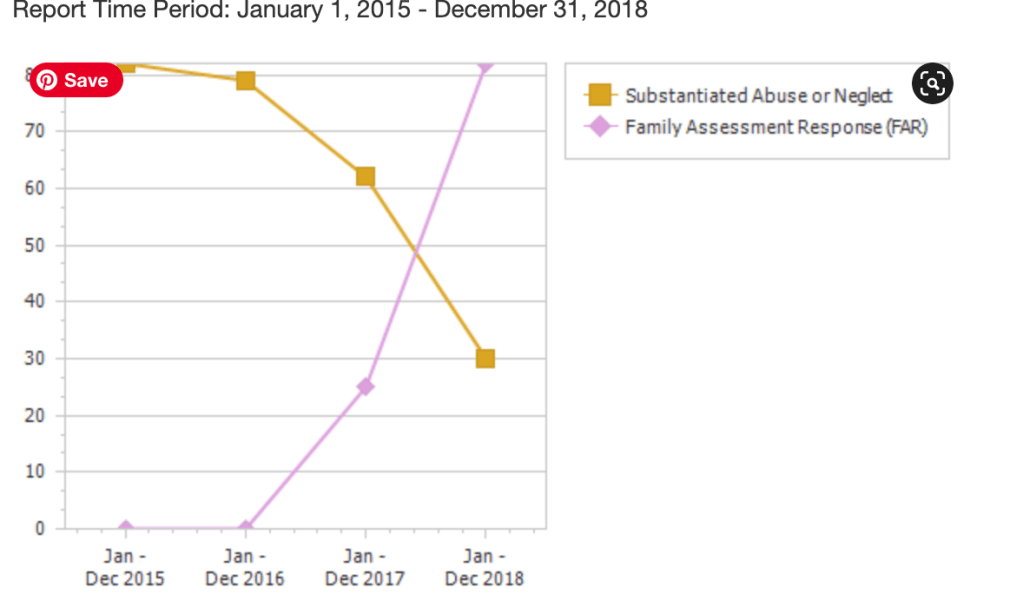
But there is a much worse –indeed fatal–problem with the two years chosen. The researchers claim that they chose 2015 because Differential Response was already in effect in in that year, having been implemented in 2013. But going to Colorado’s “Community Performance Center” (data dashboard) as helpfully directed by a footnote, one quickly learns that no children were assigned to Family Assessment Response (the option that does not result in substantiation) in Teller County in 2015, as shown in Table One below. In 2018, 82 children, or 44.3 percent of all children assessed, were assigned to Family Assessment Response. So an unknown part of the decrease in the number of children substantiated could have been due to the rollout of Differential Response.
If there was any doubt that the advent of Differential Response may be related to the drop in substantiated assessments, one only has to look at Figure One below. It is hard to figure out how the researchers missed this graphic, which is prominently displayed on the relevant page of the data dashboard, and shows how substantiations fell between 2016 and 2018 as the number of children assessed through FAR increased. This is a bizarre error, considering that the researchers specifically cited the prior rollout of differential response as a reason for choosing 2015 as the baseline year for the study.
Another problem is the method the researchers used to attribute all of the “reduction” in cases to the program. First, the authors provide no explanation of the estimate that 1,444 children received services at CPFRC. We assume this includes every child who ever walked into the center, but we just do not know, since the researchers do not define it. We have no idea of the quantity of services received by each child. We don’t even know if this is an unduplicated count. Moreover, this conclusion simply violates common sense. On the face of it, how could one assume that one family support center caused the entire reduction in child maltreatment substantiations in a county? It just beggars belief.
The second study by OMNI focused on the Westminster Family Resource Center (WFRC), which serves a mostly-Latino population in Orange County, California. WFRC provides a variety of services, including information and referral, family support, case management, counseling, after school programs, domestic violence support, parenting classes, and “family reunification family fun activities.” WFRC belongs to a network of 15 Family Resource Centers known as Families and Communities Together (FaCT). The researchers report that In conducting the study OMNI took advantage of a pre-existing evaluation of all the centers in the FaCT network, which was conducted by Casey Family Programs, Orange County Social Services Agency, another nonprofit and a consulting firm. OMNI reports that “After consultation with the evaluation team and a review of the demographic profile of the areas served by FRCs within Orange County as a whole, OMNI identified Westminster Family Resource Center (WFRC) as a strong option for this project.” (The larger study is listed as “forthcoming” from Casey Family Programs in the references to the OMNI report.)
Unlike the Teller County report, the Orange County report compares outcomes across geographic areas rather than two time periods. The researchers defined WFRC’s service area as the census tracts where at least one percent of the population was served by WFRC. They matched 12 census tracts in Los Angeles County to the area served by WFRP based on ten “community level indicators related to child maltreatment,” such as the percentage of families in poverty and the unemployment rate; the other indicators were not listed.
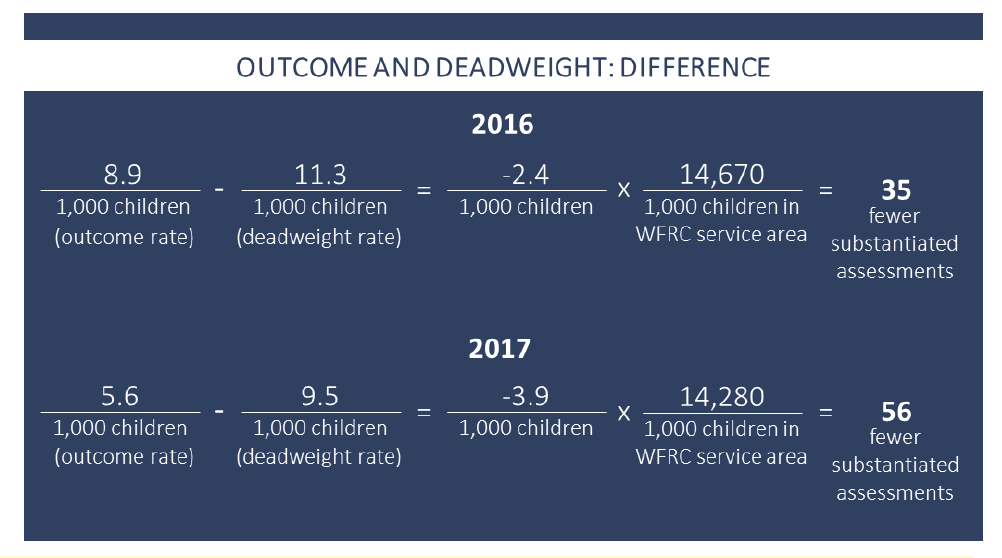
Using data from the pre-existing evaluation, the researchers subtracted the substantiation rate (number of substantiated children per 1000) in the WFRC areas from the substantiation rate in the matched areas for 2016 and 2017, the most recent years for which data were available, and then multiplied the difference by the number of children in the WFRC service area. The calculation is shown in the attached graphic, which incorrectly divides the number of children in the service area by 1,000. This calculation produced an estimate of 35 fewer substantiated assessments in 2016 and 56 fewer substantiated assessments in 2017. Unlike with the Teller County study, a reader cannot check the underlying data because it comes from an as yet unpublished study. Admitting that there are no guidelines for attributing results to a program in a “quasi-experimental evaluation” using community-level indicators, the researchers rather randomly decided to attribute 50 percent of the difference in substantiated assessments to the program.
As in the Teller County study, the researchers went on to calculate a return on investment for WFRC. Although they did not explain their methodology for doing so, it appears they used the same approach of dividing child welfare costs for each year by the number of substantiated assessments for that year to come up with an estimated cost per substantiated assessment in California, adjusting for inflation, and finally subtracting the estimated costs of WFRC. By this method, they arrived at a return on investment of $2.80 in 2016 and $4.51 in 2017, which they averaged to get a total return on investment of $3.65 per dollar spent on the program.
The use of substantiation rates as an indicator of success is as problematic as in the Teller County study. As I have mentioned, substantiation does not equal victimization but instead reflects the agency’s performance in determining whether maltreatment really happened. Using substantiation as an indicator of maltreatment could introduce bias if one of these counties substantiated allegations at a higher proportion of cases than the other, as discussed below.
While there is no mistake as glaring as the Teller County team’s erroneous assumption that differential response had already been implemented in the study’s baseline year, the possibility of significant confounding effects does exist–in this case between places rather than times. California has a county-run child welfare system and the writers do not discuss any policy or practice differences that may exist between Los Angeles County and Orange County and how they might affect the differences in substantiation rate between the two counties. And indeed, data from the Child Welfare Indicators Project at Berkeley shows that Los Angeles County does substantiate a higher proportion of allegations than does Orange County. Of all the children with allegations in 2016 and 2017, 15.7 and 14.7 percent had substantiations in Orange County, versus about 18 percent in Los Angeles County both years. In addition, the fact that the reduction in substantiated assessments, and therefore the estimated cost savings due to the program, varied so much between 2016 and 2017 is already concerning and suggest that the impact found depends upon the year, and could be vastly different if another year were chosen.
The attribution of 50 percent of the difference in substantiations between the two counties to the WFRP has no basis in fact or social science. The researchers did not attempt the kind of calculation reported for Teller County (however problematic) in which they compared the number of children served to the number of children who might be at risk of maltreatment. They indicate that WFP served 1.77 percent of households in its service area as defined by the researchers, and we have no idea how that compares to the number of households where children are at risk of maltreatment.
Looking at the Teller County and Orange County studies together, the choice of these two specific programs out of all the over 3,000 FRC’s represented by NFSN (and the choice of only one out of 15 programs evaluated in Orange County) raises the possibility that the researchers cherry-picked programs to achieve the desired results. In fact, the researchers report that that is exactly what they did! One of the criteria they reported using to select their ultimate sites was that “there were available data demonstrating a plausible connection between FRC services and child welfare system outcomes;” another was that “[t]here were available quantitative data demonstrating that the child welfare system has benefited (e.g., through reductions in the incidence of child abuse/neglect).” The researchers also claim that they were looking for sites representing “demographically different communities,” and I suppose they achieved that with their two sites with mostly White and Latino clientele; but they seem to have been unable to find a suitably promising site with a predominantly Black clientele.
Clearly it is not easy to evaluate programs without random assignment to a treatment and control group, or at least a comparison group that is matched individually to a group of participants. It is also difficult to evaluate a program where each participant gets a different package of services, with some receiving as little as one visit to the center. There is ample reason to doubt that Family Resource Centers will have a large impact on the most serious cases of child abuse and neglect because the parents who use these centers tend to be those who are already open to seeking help, learning new parenting tools, and working toward change. It seems likely that the parents of the most vulnerable children are often the ones who are not willing to seek the kind of help that Family Resource Centers provide. Chronically neglectful parents may lack energy and motivation to go to a Family Resource Center; chronically abusive families are likely to want to avoid letting other adults set eyes on their children. That is why jurisdictions that are really serious about prevention have chosen to adopt more targeted strategies. For example, Allegheny County Pennsylvania, which has a network of 27 Family Resource Centers and was a pioneer in this effort, knew they had to do more for families with more intense needs. They created a three-tier model called Hello Baby, in which families are placed into tiers based on their needs. They are reaching out to all families, and they are referring those in the middle tier to county’s FRC’s. For the families with the greatest needs, a more intensive option is being offered.
A recurrent theme of this blog has been the use of flawed research to promote the programs that the promoters want to support, most recently in my post about race-blind removals. Using flawed research to support programs results in misperceptions by the public and its representatives and in turn to bad policy decisions. One does not have to look beyond Teller County for an example “Child abuse reports have declined dramatically locally due to a partnership between a key Teller government agency and a nonprofit organization,” trumpeted a local paper based on the press release from OMNI. In the article, the DHS Director Kim Mauthe was reported as saying that “the findings of the report are good news for the county. “It’s exciting because the calls we did receive through our child abuse hotline show that we had a decrease of child abuse by 57 percent, which is huge….” It is not clear what would be more disturbing: that Mauthe really believed this program had reduced child maltreatment (not “abuse” as she described it) by 57 percent, knowing that the study period included her county’s adoption of differential response, or that she was cynically misrepresenting the study results to the media. The report was presented at a meeting of county commissioners, who applauded Ms. Mauthe. They now presumably think that child maltreatment is on its way to disappearing, and if anything more is needed it would be to add more funding to the Family Resource Center–not necessarily the best approach if they want to reach the families with the most intense needs.
It is not surprising that this flawed research was funded and promoted by Casey Family Programs, a wealthy and powerful non-profit that has played an outsized role in child welfare in recent decades, funding advocacy-oriented research, providing free consultation to states, and even helping the government hire people who support its views. One of CFP’s goals is to “safely reduce the need for foster care in the United States by 50 percent,” a goal that is incidentally meaningless without a beginning and ending date. Most recently, CFP has publicized the faulty data on race-blind removals that I discussed in a recent post.
Family resource centers can be a great addition to a neighborhood, providing connections to needed programs and services for needy families. But two recent studies that claim to show that these centers reduce child maltreatment and thereby save money to taxpayers are too flawed to provide any meaningful evidence that they indeed have this effect. Any continuing publicity these studies receive may lead unsuspecting public officials to invest in family resource centers at the expense of other programs that may be more promising in preventing child maltreatment.
A growing chorus of voices is calling for a shift of resources away from responding to child abuse and neglect toward preventing its occurrence. Interest is coalescing around a newer idea that would combine universal reach with a response that is targeted based on a family’s risk, sometimes called targeted universalism. Several jurisdictions are already implementing initiatives based on this approach. Governments interested in adopting such a system need to resolve a number of questions concerning the system’s entry point, goals, lead agency, program content, and how to attract and retain the families that are most at risk. But the idea of targeted universalism is worth pursuing as it combines the advantages of both approaches.
The new focus on prevention should not be confused with the changes made by the Family First “Prevention” Services Act of 2018, which allows funds under Title IV-E of the Social Security Act to be be diverted from foster care to services to help keep children with their families. Despite its name, Family First funds can be used only for services to families in which abuse or neglect has already occurred. Such services are generally considered treatment, not prevention, although public health specialists refer to them as “tertiary prevention,” which mean preventing the recurrence of a problem. But this is not the meaning of prevention to the layperson, and the placement of “prevention” in the title of the act continues to cause confusion.
Preventing a problem, if possible, is certainly preferable to addressing it after it appears. As child maltreatment prevention expert Deborah Daro states in an issue of The Future of Children devoted to universal approaches to promoting healthy development, doctors don’t send away patients with precancerous cells and tell them to come back when they have Stage 4 cancer. Yet, that is exactly what we do in child welfare. As Daro points out, “our public response lacks an adequate early assessment when people become parents, and we often offer the appropriate level of assistance only after a parent fails to meet expectations or a child is harmed.” For this reason, many child welfare thought leaders like Daro are calling for a new emphasis on preventing maltreatment before it occurs.
The consensus on prevention still leaves the question of how much to invest in universal approaches (known as primary prevention) as opposed to “secondary prevention” approaches that target families who are deemed to be at risk. Secondary prevention has a lot going for it. Targeting a program to those who need it most can be justified on grounds of efficiency. Why spend money reaching people who do not need help? But investing only in secondary prevention has drawbacks, as described by Kenneth Dodge and Benjamin Goodman in the Future of Children issue referenced above. Even the lowest-risk groups have some risk of child maltreatment. And because they are much larger than the high-risk groups, they may account for most cases of maltreatment. Moreover, interventions with targeted groups rarely reach a high proportion of that population, and thus cannot have a detectable impact on the problem overall. Finally, targeted programs are often stigmatized and not politically popular, leading to lower funding–and less participation by targeted groups.
Dodge and Goodman point out that a debate over universal vs. targeted approaches played out when public schooling was first discussed in the United States. Some advocates argued that middle and upper class families could pay for their children to be educated, and that confining public education to the poor would save taxpayers money. Of course the proponents of universalism won out. Even though affluent families continue to be able to buy a more expensive education through higher property taxes and access to private school, one can only imagine the sorry state of our public education system if at been confined to the poor.
As Dodge and Goodman point out, not all universal programs must provide the same services for everyone, and they cite pediatric care as analogy. All children are seen for well-child visits, during which pediatricians screen them for conditions that might warrant services from specialists, and refer them accordingly. Therefore, they argue that “the best strategy may be to embed targeted interventions in a universal strategy that reaches the entire population while offering intensive interventions for targeted subgroups.” This approach, which they call “targeted universalism,” involves screening all families at a single point in time, such as the birth of a child, identifying the family’s risks and needs, and connecting them with community resources for addressing those risks and needs.
This is the approach that they embedded in the Family Connects Program, starting with a home visit fro a nurse. Nurse home visiting is a popular platform for a universal program, and there is a lot of precedent for a universal nurse home visiting program. Universal nurse home visiting is used by many European countries, where it is part of a comprehensive maternal and child health system, and is also used in other parts of the world. Perhaps the best developed application of this approach in the United States is Family Connects, which Dodge and his team at Duke University initiated in Durham, North Carolina in 2008 as Durham Connects. The model is now being implemented in over two dozen communities around the country, and Oregon is rolling it out statewide. Family Connects aims to reach every family giving birth in a community, assess the parents to determine their risks and needs, and refer them to appropriate services. The program rests on three “pillars:” home visiting, community alignment and data and monitoring, as described by Dodge and Goodman.
The first pillar is home visiting by a trained public health nurse who visits the family in the hospital to welcome the baby and offer a free home visit when the baby is about three weeks old. During the home visit, the nurse uses a structured clinical interview to assess risk in 12 key domains that predict adverse outcomes among children. At the end of the interview, the nurse works with the family to develop a plan of action which may include follow-up visits, phone calls, or contact with external agencies. With parental consent, this plan is shared with the baby’s pediatrician and the mother’s primary care provider. Four weeks later, a program staff member calls the family to check on their progress and determine if the referrals were successful. If the family has not succeeded in making the connection, the program either helps the family try again or makes another referral.
The second pillar, called community alignment, is a compilation of community resources available to families at birth, including targeted home visiting programs, early care and education, and mental health. This directory is available in electronic for for nurses to use on their visits. The third pillar is an electronic data system that documents each family’s assessment, referrals, and connections with community agencies. These records, scrubbed of identifying information, are aggregated to provide information about each agency and on a community level to identify gaps between needs and services. To contain costs, Family Connects is limited to seven contacts (phone calls and visits) over the course of 12 weeks. Dodge and Goodman report that the cost of Family Connects ranges from $500 to $700 per family.
Family Connects has been evaluated with two randomized controlled trials (RCT’s) in Durham, NC and one field study in four rural counties in the state. Eighty percent of the intervention families in the first trial scheduled a visit and 86 percent completed it, for a total “completion rate” of 69 percent. In the second trial, the percentages were 77 percent scheduled and 84 percent completed for a total of 64 percent. The first and second RCT’s found 49 and 52 percent of families respectively to have moderate needs, 46 and 42 percent to have serious needs requiring referral to a community resource, and one percent with a crisis needing immediate intervention. Of the families referred to a community agency, 79 percent and 83 percent reported they had followed through and made the connection. In the first RCT, researchers found that intervention infants had 39 percent fewer referrals to Child Protective Services (CPS) than did the control infants by the age of 60 months, controlling for demographic risk factors, as well as a 33 percent decrease in emergency room use.
Nurse home visiting is not the only possible platform on which to base a targeted universal program, Other options for locating a universal service include pediatric practices. There are two different models based in pediatrician’s offices that have shown promise for preventing child maltreatment–SEEK and Healthy Steps. SEEK trains pediatric primary care providers (PCP’s) to use a questionnaire to assess for a specific set of risk factors. The PCP initially addresses identified risk factors and refers the parent to community resources, ideally with the help of a behavioral health professional. Healthy Steps, as described by Valado and coauthors in The Future of Children, functions as a targeted universal model with three tiers. All families receive screenings and access to a child development support line. Second-tier families receive short-term consultations, along with referrals, additional guidance and resources. Families classified in the highest-risk tier receive “a series of team-based well child visits incorporating a Healthy Steps specialist.”
Models based in pediatric practices have had some promising results. A study testing SEEK with a high-risk sample of patients from a pediatric primary clinic in Baltimore found a “striking” 31 percent reduction in CPS reports. The other SEEK study focused on a low-risk population and there were not enough cases of maltreatment to find impacts on abuse and neglect; however, the study found a lower rate of physical punishment and psychological maltreatment reported by participating mothers. A multisite evaluation of Healthy Steps, as described by Velado et al, showed similar effects, such as a 33 percent reduction in the use of severe physical discipline in the intervention group vs the comparison group when the child was 30-33 months of age. The philanthropic partnership Blue Meridian Partners has chosen Healthy Steps as one of five models to receive large grants to help bring them to a national scale as a potential solution to poverty and lack of economic mobility.
Neither of these primary care-based models has been used universally throughout a jurisdiction. Moreover, pediatric care based models have less reach than models based on the birth hospital. Almost all babies are born in hospitals, but fewer infants attend their regularly scheduled well-baby visits. But according to the National Survey of Children’s Health for 2019, only an estimated 89 percent of children aged 0 to five had experienced one or more preventive care visit in the past year. While hopefully the percentage is greater for infants, it is probably less than the nearly 100% who are born in hospitals.
Many questions must be answered in developing a “targeted universal” child maltreatment prevention system.
What should the entry point be, and should there be more than one? Having all families enter the program through the same portal (be it the GYN practice, birth hospital, or pediatrician’s office) would avoid overlap and inefficiency. Choosing the system that meets parents earliest–the OB-GYN office–would allow programs to make a difference at a crucial time but would also miss the children who get little or no prenatal care. The founders of Family Connects chose to use the birthing hospital because it covers the most families, even though they are missing the chance to address problems that begin prenatally. Combining two or more portals may increase a program’s reach and the opportunity to coordinate and extend services. In Guildford County, NC, Healthy Steps is being integrated with Family Connects. Michael Wald, in a forthcoming article in the Handbook of Child Maltreatment, proposes a prevention system that starts with OB-GYN’s and WIC programs in the prenatal stage and continues with universal services at birth through pediatricians, home visitors and family resource centers. All of these entry points in turn would refer families to targeted services. Using more than one portal requires linkages and procedures for hand-off or collaboration, adding complexity to the system, but increases potential coverage.
What should the goals of the system be? A basic question is whether the system would be framed as a child maltreatment prevention system or something broader. It is hard to separate the goal of preventing maltreatment from that of promoting healthy child development, and indeed most of the programs discussed above have broader goals. The mission of Family Connects is “to increase child well-being by bridging the gap between parent needs and community resources.” Healthy Steps has the goal of “promoting the health, well-being and school readiness of babies and toddlers.” Clearly it is hard to separate the goals of child maltreatment prevention and the promotion of child well-being and healthy development.
What should the lead agency be? A key question about universal prevention is which system should take the lead. Child welfare leaders like Jerry Milner, head of the Children’s Bureau under the Trump Administration, have expressed the desire to expand the role of child welfare to include primary prevention. But if the goal is the broader enhancement of child development, and if the main providers of universal services are health professionals rather than social workers, another agency like public health may be a more appropriate home. Moreover, the child welfare system is already overburdened and underfunded. The work of investigating existing abuse and neglect (which will never be totally eliminated), helping parents and children heal, and making sure children have a safe environment to thrive either temporarily or permanently, is work enough for this beleaguered system. It is interesting that many modern child welfare leaders are so discontented with their primary mission that they are crying out to take on prevention. Perhaps the answer lies in the current political climate, which disparages child protective services and foster care, rather than recognizing the crucial role these services play in protecting children from harm,
What should the targeted services be? Michael Wald raises the question of whether a limited set of evidence-based models should be supported as part of a prevention system or whether jurisdictions should be given free rein in program selection. There are arguments for both, but it may be more practical to allow local jurisdictions to choose their own programs, especially since most “evidence-based” programs have only modest effects. But there are many reasons to advocate that every family found to be high-risk receive early care and education (ECE) interventions such as Early Head Start and Educare, which reduce child maltreatment risks in so many different ways, as I argued in an earlier post. The proposed Child Care for Working Families Act should help make such quality programs more available around the country.
How can we engage the highest-risk families? This is perhaps the thorniest question of all. All of the existing and proposed programs discussed above are voluntary, and voluntary programs never succeed in involving all eligible families. Moreover, it is often hardestto enroll and retain the highest-risk families in parenting support programs. We have already seen that Durham Connects provided a home visit to only 69% and 64% of eligible families in its two RCT’s. And considering that only 79 percent and 83 percent accessed the recommended services, the actual completion rate goes down further. In a study of Durham Connects, the researchers found that parents with a higher risk based on demographic factors like age and income were more likely to agree to a home visit but less likely to follow through. They also found that infant health risk, as measured by low birth rate, birth complications, and medical diagnoses, was associated with lower levels of both initial engagement and follow-through. An HHS issue brief suggests many ways to improve a program’s performance in enrolling and engaging families in home visiting programs. Not listed is the idea of including a peer mentor in the program model, which is embedded in some newer initiatives like Hello Baby and the Detroit Prevention Project. But the fact remains that a voluntary program will leave some children unprotected until they are actually harmed by abuse or neglect. Yet, it is clear that a mandatory child abuse prevention program will not be accepted in the U.S–just look at the debate over the COVID vaccine. We can hope that If a universal, voluntary prevention program is adopted, it will gradually gain in acceptance by high-risk and low-risk parents alike as a valuable benefit. In case that does not occur, we must record identifying information about the parents who do not accept the initial offer to participate and and follow up on future outcomes for their children in order to assess the efficacy of the program at preventing maltreatment among the highest-risk groups. Moreover, CPS must have access to this information when they receive a new report on a family.
Can the system be funded by cutting child welfare budgets? Congress has an unfortunate history of cutting funds to unpopular programs prematurely with the hope of achieving savings by a new approach, rather than waiting for a new approach to yield savings. One could mention mental health deinstitutionalization but a closer analogy might be the Family First Act’s moving money away from congregate care toward family preservation services, before states have the foster homes to replace these facilities, thereby simply shifting the cost of such facilities to states. We hope that establishing a robust system of prevention may well eventually result in a reduction of calls to Child Protective Services and in the need for foster care and in-home services. But we cannot reduce funding for traditional child welfare unless and until this effect has occurred, as Brett Drake argued in in a webinar recently conducted by the American Academy of Political and Social Science (AAPSS) in conjunction with their 2020 volume on child maltreatment. Even then it may make sense to retain current funding as the system is currently stretched thin.
What about anti-poverty programs? Adopting a system of targeted universalism to prevent child maltreatment does not directly address poverty, a prime risk factor for abuse and neglect, as discussed in my last post. Targeted universal programs will not change the level of welfare benefits or housing availability. However, it is important to remember that most poor families do not neglect their children, as University of Maryland’s Brenda Jones-Harden mentioned in the AAPSS webinar. Those families that are functioning well will find a way to get the resources they need to care for their children, and the supportive services provided through targeted universalism may help the others do the same. But at the same time, prevention advocates should fight to improve economic supports so that no child is deprived of what he or she needs to grow up into a healthy and functioning adult. Some of the new programs already passed or under discussion under the Biden Administration and the new Congress, such as the expanded child tax credit and the Child Care for Working Families Act, will help make targeted interventions more effective by addressing some of the poverty-related risk factors that cannot be addressed by targeted programs.
There is a growing consensus in the child welfare world that we must focus on prevention of abuse and neglect, and there is an increasing interest in using the approach of targeted universalism. The current historic expansions of the safety net will provide the perfect backdrop for such an initiative by addressing the economic risk factors for child abuse and neglect. With the motivation to build a better society in the wake of the pandemic, the time may be right to develop a universal, targeted system to prevent child maltreatment and allow every child the conditions for optimal development.
April is Child Abuse Prevention Month, the blue pinwheels are on view around the country, and the obligatory emails and tweets are urging people to recognize the month with Facebook frames and Zoom backgrounds. And in the past year or so, prevention has become the word of the day in child welfare. This year, the House of Representatives has passed the Stronger CAPTA Act, which would raise the authorization for prevention services to match that of treatment services. CAPTA provides funds to state child welfare agencies for child abuse prevention, investigation and treatment programs. However when it comes to prevention, child welfare agencies are only a small part of the answer. Preventing child maltreatment requires the involvement of many other sectors of the government and society. It is important for prevention advocates to understand this and to work with other child advocates to support these programs.
In searching for guidance in how to view child abuse and neglect prevention, I came across an excellent 2016 publication from the Centers for Disease Control (CDC). Preventing Child Abuse and Neglect: A Technical Package for Policy, Norm, and Programmatic Activities provides “a select list of strategies ….based upon what we know about risk and protective factors as well as empirical evidence on whether they have been shown to affect child abuse and neglect.” The CDC cites a number of risk factors researchers have found to be associated with the perpetration of child abuse or neglect, including young parental age, single parenthood, large number of dependent children, low parental income, parental substance abuse, parental mental health issues, parental history of abuse or neglect, social isolation, family disorganization, parenting stress, intimate partner violence, poor parent-child relationships, community violence, and concentrated neighborhood disadvantage. In addition, children who are younger and have special needs are more at risk of suffering maltreatment. Protective factors include supportive family environments and social networks, and probably other factors like parental employment, adequate housing, and access to health and social services.
Considering risk and protective factors leads to a broader conception of child abuse prevention than the one promoted by federal, state and local child welfare agencies. The CDC report lays out five strategies, all of which contain approaches that have demonstrated success in preventing child maltreatment. I have added a new strategy to CDC’s list and made some other smaller changes which are explained in notes. My modified list of strategies and approaches is summarized in the table below.
Preventing Child Abuse and Neglect
Strategy
Approach
Strengthen economic supports to families
-Strengthening household financial security -Family-friendly work policies
Encourage pregnancy planning, spacing and prevention*
-Increased availability of long acting contraceptives -Public engagement and education campaigns
Change social norms to support parents and positive parenting
-Public engagement and education campaigns -Legislative approaches to reduce corporal punishment
Provide quality care and education early in life
-Preschool enrichment with family engagement -Improved quality through licensing and accreditation
Provide parenting support to at-risk parents**
-Early childhood home visitation -Other parenting skills and relationship interventions -Enhanced case management plus peer engagement*** -Enhanced primary care to address maltreatment risks****
Intervene in maltreating families to lessen harms and prevent future risk
-Behavioral parent training programs -Treatment to lessen harms of abuse and neglect exposure -Treatment to prevent problem behavior and violence
**Strategy and approach titles modified by Child Welfare Monitor
***Approach added by Child Welfare Monitor
****Approach moved from following strategy by Child Welfare Monitor
As the CDC points out, the strategies address different levels, from the individual to the societal. The first four operate on the community or societal level and the CDC hypothesizes that they are most likely to have a “broad public health impact on child abuse and neglect.” The last two strategies operate on the family and individual level and would have a narrower impact focusing on targeted populations.
Strengthen Economic Support to Families: Low parental income is one of the major risk factors for child maltreatment, as documented by multiple studies cited by the CDC. Economic insecurity leads to maltreatment, presumably by making it more difficult to meet children’s needs and provide quality childcare and by increasing parental stress and depression, both risk factors for child abuse and neglect. Approaches to strengthening economic support for families could include both improving economic assistance to low-income families and intervening to support family-friendly work policies like livable wages, paid leave, and flexible and consistent scheduling. The CDC cites studies of several economic support programs for which research has demonstrated a direct effect on child abuse and neglect or associated risk factors. Perhaps the expanded 2021 child tax credit will have such an effect.
Encourage Pregnancy Planning, Spacing and Prevention: The CDC report identified young parental age and large number of dependent children as risk factors for abuse and neglect, but it did not propose a strategy to address those risk factors. But as I have written before, there are strategies to address these risk factors and they should be considered. One approach would be to expand access to long acting removable contraceptives (LARC’s). A statewide campaign to increase availability of LARC’s in Colorado resulted in a halving of the teen birth rate in five years. Another approach would be public information campaigns to inform people of the dangers of early and closely spaced childbearing and the advantages to both parents and children of pregnancy planning and spacing. Research indicate that such campaigns can change people’s health-related behavior, as in the case of smoking cessation and HIV prevention.
Change social norms to support positive parenting. As the CDC points out, norms about how we discipline our children are especially important to child abuse prevention. An analysis of 50 years of research found that spanking leads to more defiance, and increased antisocial behavior, aggression, mental health problems and cognitive difficulties. A recent study found that the percentage of parents who reported spanking a child in the previous year dropped from 50 percent in 1993 to 35 percent in 2017. Yet corporal punishment remains popular in some communities. While corporal punishment is not necessarily child abuse, it can lead to physical abuse when the parent loses control or goes too far. The CDC recommends both public education campaigns and legislative strategies to reduce the use of corporal punishment. The report cites successful public education campaigns regarding other parenting behaviors, such as emotional abuse. It also cites international studies indicating that bans on corporal punishment were successful at decreasing overall rates of corporal punishment.
Provide quality care and education early in life. Early care and education (ECE) is a particularly appealing child maltreatment prevention strategy because there are so many pathways by which it can operate to reduce child maltreatment. Quality ECE reduces parental stress, exposes the child to mandatory reporters, and reduces the time spent in an abusive or neglectful home or with an unrelated adult–often the perpetrator of severe or fatal child abuse. ECE approaches with a family engagement component may prevent maltreatment by training parents in positive discipline approaches. Approaches to providing ECE could include expanding government support to programs that combine childcare with educational enrichment and parent involvement and improving standards to increase quality. Studies suggest that childcare programs that include parent involvement are effective in preventing child maltreatment. A 15-year follow up of Child Parent Centers found that children who participated for one to two years had a 52 percent reduction in substantiated child abuse and neglect.
Provide parenting support to at-risk parents. Intervening directly with a targeted population of parents to address risk factors for child maltreatment is perhaps the most popular approach to child maltreatment prevention because it has a clear connection with child maltreatment and often falls under the jurisdiction of child welfare agencies. Such approaches include home visiting programs as well as interventions based in doctor’s offices, preschools, school or mental health clinics. These programs vary in their models and the risk factors they address. Many of these programs focus parent education and training, based upon the assumption that poor parenting skills and ineffective discipline practices can lead to maltreatment. Some interventions focus on the parent-child relationship since poor parent-child relationships are a risk factor for child maltreatment. Many of the home visiting programs include a case management component to help parents set goals for their own lives and access needed services, thus addressing risk factors like substance abuse, mental illness, and parental stress. Home visiting interventions like Nurse Family Partnership, SafeCare and Child First and parent training programs like Incredible Years and Triple P have been found to have small to moderate effects on maltreatment and related risk factors. Another approach is to use the pediatrician’s office to identify families at risk of abuse or neglect, address these risk factors at regular visits, and provide information and referrals. Both SEEK and Healthy Steps are examples of this approach that have had some promising results but needs more evaluation. A new generation of programs, as yet unproven, is connecting at risk families with both a case manager and a family engagement specialist who provides peer support. Examples of that approach include the intensive tier of Allegheny County PA’s Hello Baby program and the Detroit Prevention Project.
Intervene in maltreating families to lessen harms and prevent future risk. In this category, CDC places therapeutic programs that seek to limit the damage caused by prior maltreatment. Such programs are often known as tertiary prevention and aim at preventing further abuse and neglect or healing victims so that they do not proceed to abuse the next generation. The CDC divides these programs into three approaches. One approach is “behavioral parent training programs,” like Parent Child Interaction Therapy. Also included in this approach are SafeCare and Incredible Years, which are also in the secondary prevention category. Another approach is treatment for children and families to lessen the harms caused by abuse or neglect, such as Trauma-Focused Cognitive Behavioral Therapy. And the final approach suggested is treatment to prevent problem behavior and later involvement in violence, which includes programs such as Multisystemic Therapy. All of these programs have shown some impact on maltreatment or associated risk factors.
Of the six strategies discussed above, only the last two generally fall under jurisdiction of child welfare agencies–and and even those are often delivered by public health or behavioral health agencies or pediatricians’ offices. But the other four strategies are often not mentioned in discussions of child maltreatment prevention simply because the latter is considered to be the province of child welfare agencies. It is not surprising that the responsibility for preventing child maltreatment is often attributed to the agencies responsible for identifying and treating it. But as described above, the range of risk and protective factors is much larger than what child welfare agencies have the capacity or mandate to address. CDC suggests that public health agencies are well-suited to take the lead in developing community-wide prevention strategies that bring in the other systems that need to be involved.
It took a public health agency to articulate the broad scope of risk factors that lead to child abuse and neglect and the need for a broad spectrum of approaches to address it. Let us hope that public health agencies on the national, state and local levels can take the lead in pushing for a full spectrum of strategies that deserves the name of child maltreatment prevention.
The current mainstream discourse in child welfare is all about prevention: reaching families before maltreatment occurs instead of intervening afterwards. Many jurisdictions pay lip service to this mantra by making services available to high-risk communities but not targeting these services to the families who need them most. The Detroit Prevention Project, launched by the Michigan Department of Health and Human Services (DHHS) in conjunction with an innovative organization called Brilliant Detroit, is different. It reaches out to families at risk of child maltreatment with an intensive case management and peer mentorship intervention aimed at preventing child abuse and neglect.
“One of the top priorities of the new administration when it comes to the child welfare system is to connect with families and provide them with support and resources before there is a need for Children’s Protective Services to file court petitions,” said JooYeun Chang, who served previously as the head of the Children’s Bureau and Managing Director of Casey Family Programs and came to Michigan in 2019. “We believe children are better off when they are with their families as long as we can work with families to make sure the children are safe.”
Interest in preventing child maltreatment before it occurs has been increasing in child welfare. But the drop in CPS reports under virtual schooling, which deprives the current system of its main trigger for action, has led to even more interest in prevention. In Michigan, DHHS had already begun to formulate plans for shifting toward a more proactive approach but COVID-19 accelerated those efforts, according to a recent article from Second Wave Media.
The new program, called the Detroit Prevention Project, pairs families at risk for child maltreatment with two workers, each performing a different function. Peer mentors, also known as “parent partners,” are community members who have experience in navigating the child welfare system in Detroit. They receive training in mental health peer support and how to work within MDHHS systems. Benefits navigators connect families to community resources such as food, housing assistance, education, and employment. The use of peer mentors or counselors is a newer approach in child welfare that has been shown to produce positive effects on outcomes associated with reduced child maltreatment. While many other programs use either peer mentors or benefits navigators, combining the two is an innovative approach.
DHHS decided to pilot its new approach in two of the zip codes with the highest rates of referrals of child abuse and neglect in the state. They chose to work with Brilliant Detroit, an organization founded in 2015 to “provide a radically new approach to kindergarten readiness in neighborhoods,” according to its website. The program has created family centers in neighborhoods which attempt to provide families of children aged 0 to 8 with all the services (emphasizing health, family support and education) needed to ensure school readiness and provided needed family support. Co-Founder and CEO Cindy Eggleton was awarded a 2021 Purpose Prize from AARP for her work in founding and directing Brilliant Detroit.
Families are also given access to a variety of programs already offered by Brilliant Detroit. These range from anger management and GED classes to nutrition workshops and fitness activities. Also offered are community based playgroups, intensive tutoring for the kids, family literacy programs, “parent cafes” to help parents connect, workforce and financial literacy training, free sports for children, and more.
The program is strictly voluntary and is being offered to a group of families drawn from two sources. DHHS is referring families that were the subject of a child protective services investigation in the past year based on their score on its Structured Decision Making (SDM) Tool. SDM is an actuarial assessment system, used by many states, to assess risk and make decisions about how to handle a case. Families that had an investigation closed with a score of III (evidence of abuse or neglect but a low or moderate level of risk to the child) or IV (insufficient evidence to show that abuse occurred but future risk of harm to the child) are normally referred to community services. These families will be invited to participate in the Detroit Prevention Project. Brilliant Detroit is also offering the program to families that it already knows from its neighborhood work.
The goals of the program are as follows, according to the document provided by Brilliant Detroit:
Reduce the number of at-risk families in zip codes 48205 and 48288 that are reported from child abuse and neglect;
Align existing MDHHS programs with Brilliant Detroit’s network of partners to create a comprehensive continuum of services.
Provide data on the efficacy of the model
Construct a model that can be scaled up through additional funding and community based partnerships.
The Detroit Prevention Project was jointly developed with leadership from the Skillman Foundation and Casey Family Programs. Skillman suggested that MDHHS talk to some of their partners on the ground, including Brilliant Detroit, to flesh out the ideas, which led to the partnership. The funding is being provided by MDHHS, Casey and Skillman. When it reaches full scale, the program will serve 400 families.
The Detroit Prevention Project embodies the prevailing sentiment in child welfare in favor of preventing abuse and neglect before they occur. This push has been led from the top by the Children’s Bureau, where Chang’s successor Jerry Milner has been a forceful advocate for this approach. Many states have responded with enthusiasm and new programs. However, some states have created new programs (like the Family Success Centers recently opened by the District of Columbia based on New Jersey’s model) without targeting them to children that are at risk of child abuse or neglect. Without a systematic effort to reach out to the families who need these services most, there is no assurance that these families will receive the services.
DHHS might want to consider using the Detroit Prevention Model to reach further upstream, following the example of Allegheny County, Pennsylvania. Allegheny County’s Hello Baby program reaches out to parents of new babies to offer them a tiered set of services. Families with the most complex needs based on a predictive risk model are offered the most intensive approach which, similar to the Detroit Prevention Program, matches each family with a peer counselor and a case manager. Given Brilliant Detroit’s mission of focusing on children from zero to eight and DHHS’s focus on prevention, this would be a natural step for both partners.
Participation in the Detroit Prevention Program is strictly voluntary, which means that some of the most troubled families will refuse to participate. Research indicates that it is difficult to engage the highest-risk families in voluntary services. We hope that the program will collect and report on the number of families refusing to participate and track their future maltreatment reports, in order to assess the extent of this problem. If it is extensive, leaders may need to consider using a family’s refusal to participate as the trigger to initiate an investigation.
Michigan DHHS should be commended for the implementation of the Detroit Prevention Program. We hope that child welfare leaders in other states are watching this initiative carefully. We also hope that DHHS will subject this program to intensive evaluation so that we can learn from this experiment experiment.
April is child abuse prevention month, and many organizations are offering recommendations on how to prevent child maltreatment. Typically these recommendations do not include one approach that may promise the most success–prevention of teenage, unplanned and closely spaced pregnancies.
Sarah Brown, founder of the National Campaign to Prevent Teen and Unplanned Pregnancy (now Power to Decide) gave a lecture in December 2015 that brought home this unfortunate omission. She reported being struck by “the total absence of pregnancy planning, spacing and prevention in virtually all discussions of how to improve overall child and family well being.” As she put it, many groups concentrate on services after the child is born, but “rarely do they mention the time when decisions are made about when with whom and under what circumstances to become pregnant or cause a pregnancy.”
There is no lack of research on the connection between pregnancy timing and child maltreatment. There is a strong association between child maltreatment and the mother’s age at the birth of the child. California researchers Emily Putnam-Hornstein and Barbara Needell found that babies born to mothers who were under 20 were twice as likely to be reported to child protective services (CPS) by the child’s fifth birthday as those born to mothers 30 or older. Among children referred to CPS by age five, almost 18 percent were born to a teenage mother and 50 percent were born to a mother younger than 25. Among children with no CPS contact, only 8 percent were teen births and 30 percent were born to a mother under 25.
There is also strong evidence that family size and child spacing are correlated with child maltreatment. Putnam-Hornstein and Needell found that children who fell third or higher in the birth order were more than twice as likely to be the subject of a report as first children. Moreover, a large study published in 2013 found that women who gave birth to another child within 24 months of the previous child were 80 percent more likely to have a substantiated CPS report.
And research suggest that the interaction between birth order and maternal age creates the highest risk for a child maltreatment fatality. A study using linked birth and death certificates for all births in the U.S. between 1983 and 1991 found that the most important risk factors for infant homicide were a second or subsequent infant born to a mother less than 17 years old. These infants had 11 times the risk of being killed compared with a first infant born to a mother 25 years old or older. A second or subsequent infant born to 17 to 19-year-old mother had nine times the homicide risk of the first infant born to the older mother.
And setting the research aside for a moment, anyone who has worked for or with CPS, or in foster care, knows the prevalence of larger families with closely-spaced children in the system, often with a mother that started childbearing as a teen. The same pattern has been observed among families that experience a child fatality.1
It is truly unfortunate that the number of children in families that are involved in child welfare is not among the data required to be reported to the federal government by states. It is highly plausible that if these data were collected we would see a big difference.
If it is not the lack of research, why do supporters of child maltreatment prevention fail to include family planning and contraception in their suggestions? In part, Sarah Brown says of child advocates in general, it may be that they simply don’t think of it. But in large part, says Brown, it is because they fear getting in trouble and becoming mired in controversy about abortion or sex outside marriage. In addition to the issues raised by Brown, it is likely that others avoid this topic because of the shameful legacy of past attempts to control the population of minority groups.
But people who care about the future of African American children should not allow this racist history to prevent thinking clearly about what is best going forward. There are few if any policies that could be more helpful to the future of black children and the elimination of racial disproportionality in foster care placement than ensuring that black women have access to the most effective methods of contraception so that they can determine their own futures.
Family planning and contraception need to be included in the discussion about child maltreatment prevention. We have made great progress in teen pregnancy prevention. The teen birth rate has fallen dramatically from 59.9 per thousand in 1990 to 24.2 per thousand in 2014. While research suggests that reality TV shows and the last economic recession contributed to the decline in teenage pregnancy, better information about preventing pregnancy and the availability of more effective methods have doubtless contributed to the drastic decline.
The Colorado Family Planning Initiative, initiated with the help of a private funder, improved access to highly effective methods of contraception by training public health providers, supporting family planning clinics and removing the barriers to obtaining Long Acting Reversible Contraceptives (LARC’s). As a result of this initiative, the state’s teen birth and abortion rates were cut in half in just five years, with big financial savings to the state. Because younger mothers are so much more likely to abuse or neglect their children, this initiative should yield lower maltreatment rates now and into the future.
Upstream USA, a nonprofit organization, hopes to expand the Colorado program nationwide, starting with Delaware. Delaware’s Contraceptive Access Now (CAN) is a partnership between Upstream and the State of Delaware to decrease the incidence of unintended pregnancy. CAN works to ensure that all women get same-day access to all methods of birth control, free or at a nominal cost. They are also working to eliminate administrative and reimbursement barriers so that women can access LARC’s immediately after giving birth, taking advantage of a crucial opportunity to provide this critically important service.
Imagine if these initiatives could be expanded nationwide, combined with a public information campaign to explain the benefits of planning, spacing and timing pregnancy for both children and their parents.
Few child welfare experts have noted the link between family planning and child welfare. One of the few is Judge Patricia Martin of Illinois, a member of the Commission to Eliminate Child Abuse and Neglect Fatalities (CECANF). Martin included teen pregnancy prevention, especially in high-poverty neighborhoods and among youth in foster care, as one of the recommendations in her dissenting report.
Family planning experts also rarely if ever mention the potential of their programs to reduce child maltreatment. The more immediate benefits of increased opportunities for women and reduction in taxpayer funding for cash assistance and other services are more than enough to justify spending on helping women plan their childbearing.
The link between child abuse prevention and family planning is clear. I hope that the word will spread and that child welfare advocates and family planning advocates can work together for increased resources to help young people plan their childbearing based on their readiness to be parents.