This summer, I was asked by a reporter to comment on a terrible case in the District of Columbia. Twenty-month old Kemy Washington died of starvation and dehydration, after her mother had had overdosed on a mix of MDMA, cocaine, ethanol and the animal sedative xylazine. An older sibling had been removed from Kemy’s mother due to her neglect and that child’s guardianship with a relative had been ratified only days before Kemy was born. Yet, Kemy was never on the radar screen of the Child and Family Services Agency until her grandmother made two calls, which were apparently screened out as not involving child abuse or neglect. When I read the more than 600 comments on the article, I was struck that over and over again, commenters asked the same question. How is it that a mother who had a previous child removed from her due to neglect could give birth to another child without triggering an investigation, close monitoring, or even removal of the child? The reporter asked me the same question and I explained that such a policy, though clearly logical to members of the community, would never be accepted by the current child welfare establishment, where it would be viewed as an unacceptable infringement on parents’ rights.
I have often remarked on situations where child welfare policy or practice departs from general community norms. Whether it is the continued screening out of calls on the same family, even if a child was previously removed; the refusal to consider policies that would trigger investigations when a new child is born to a parent who committed severe abuse or neglect; the push to “reunify” children with parents who have proved over and over again that they cannot keep them safe or even stop harming them, it seems that policymakers and practitioners of child welfare are operating from a different set of norms than the public. What would be clear to a grandparent, a neighbor, or a random layperson do not seem so evident for those who are charged with protecting our children. This was made very clear in a devastating report on child fatalities in Minnesota. As the authors put it,
Members of the public often express dismay and outrage to us over stories such as those recounted in this report. We infer from this that the professional norms currently guiding child protection and foster care are out of alignment with those of the broader community.
Examples of this divergence abound, and I am sharing just a few here.
“B.B.” was born in the State of Washington in 2022 and died of fentanyl poisoning in March, 2023. Starting in 2014, the Department of Children, Youth and Families (DCYF) had received 30 reports about B.B.’s family for the use of heroin, marijuana and alcohol in the home; lack of supervision of the children; domestic violence; an unsafe adult living with the family; an unsafe and unclean physical environment; unsecured guns in the home, “out-of-control” behaviors by B.B.’s older siblings at school to which the mother was unresponsive, seeming “out of it;” concerns about the children’s hygiene; and the mother driving under the influence of marijuana. A few days before B.B.’s death, a caseworker told B.B.’s mother that the agency was closing a voluntary services case that had been open for about half a year. But the family was already under investigation again at the time B.B. died.
There have been multiple cases around the country of child protection workers disregarding reports of hungry children eating food from the floor or the garbage, until a child finally died or escaped from the torturers. School staff in Utah reported making at least four calls in the 2022-2023 school year (confirmed by a timeline released by DCFS) to CPS alleging that Gavin Peterson was always hungry and eating food from the trash. School staff were buying his lunch but had to stop after his father and stepmother forbade it. One school staffer “said Gavin’s father and stepmother justified Gavin’s small frame and constant desire for food as side effects from his medication, but she didn’t buy it.” Why did CPS? That summer, Gavin was withdrawn from school. A year later he was dead after years of starvation and beatings.
Seven-month-old Emmanuel Haro is missing and presumed dead. Investigators believe that he was abused for an extended period of time before he was killed. But his suffering and death could have been avoided. His father had been arrested for abusing a child from a previous marriage in 2018–abuse so serious that the child is now bedridden. A simple “birth match” policy could have prevented the death of Emmanuel Haro. If birth records were linked to criminal and CPS records, Emmanuel’s birth could have triggered a mandatory investigation and monitoring because the father had been convicted of child abuse–the kind of policy that commenters in the Kemy Washington case were asking for. It is hard to think of a more common-sense idea than birth match. Yet, only five states had such a policy in 2022, according to my report on birth match for the American Enterprise Institute. And most of these programs are very limited both in terms of which parents are covered and of the state response.
Even a birth match policy would not help in cases where a parent’s violent history is known but disregarded. Four-year-old Rykelan Brown died from a beating by his father, Joshua Emmons, in May 2024, two months after he was removed from a loving foster home to be placed with Emmons. The foster parents had repeatedly reported that Rykelan came home from visits with his father bruised and saying his father hit him and he never wanted to go there again. The local Department of Social Services knew that in 2019 Emmons had beat his then-girlfriend’s three-year-old son so severely that he damaged the child’s liver, which must now be checked regularly. But the social services commissioner told an interviewer that the event occurred too long ago to be considered. Really? Even when paired with Rykelan’s bruises and reports of beatings?
As the above examples show, some things that are intuitive to ordinary people – -like that a child going to school hungry (and not because of poverty) – is a sign that something is deeply wrong at home–seemed to be missed by people engaged in child welfare practice, administration and policymaking. Much of the problem stems from a dominant ideology that preaches that abused and neglected children are almost always better off with their own families. The same viewpoint holds that what child welfare calls neglect is just poverty, as if all poor parents neglect their children, and that child welfare is a a racist system that was created to destroy Black and Brown families.1 Social work schools have adopted and promulgated these positions and agencies have incorporated them in the training for new social workers. Deep-pocketed groups like Casey Family Programs have used their money to foster this ideology through training and technical assistance to state and local agencies. The entire child welfare community in many states has found itself endorsing policies and practices that defy common sense thinking.
We must bring child welfare policy and practice back into alignment with community norms. But that is easier said than done. The public pays little attention to child welfare until there is a tragic fatality or egregious incident that is covered in the media. But many of these cases are never known to the media and therefore to the public. And even when they are, child welfare agencies often refuse to release information about their past involvement with the family, in violation of federal law. So the press, the public and legislators cannot identify what went wrong and what would be needed to prevent future tragedies in the future.
A small but useful first step to align child welfare systems with community norms would be to make the public aware of decisions that clearly violated these norms and harmed children. The federal government should enforce the requirements of the Child Abuse Prevention and Treatment Act (CAPTA), which as interpreted in the federal Child Welfare Policy Manual, requires states to issue specific information and findings on all child maltreatment fatalities and near fatalities caused by maltreatment. That includes information about past dealings between the children’s families and the child welfare agency. Ultimately, the requirement must be expanded to cover all “egregious incidents” where maltreatment is suspected.2 Increased public awareness how child welfare agencies knowingly and routinely leave children in harm’s way may help elevate child welfare into a major issue, not a backwater that gets addressed only when there is a tragedy.
Three family members are awaiting trial for murdering 11-year-old Arabella McCormick in August 2022 and torturing her sisters. A kindergarten aide in Arabella’s class told a reporter that she got a disturbing note from Arabella’s foster mother, who went on to adopt her and then allegedly participate in her murder. “In the envelope, it said, ‘Arabella is,’ and it was line items such as ‘a terrible child,’” she said. “‘She’s a liar. You can’t believe anything she says. She’s a thief. She steals everything. Don’t trust her.’ It was just one thing after another of horrible things that you would never say about a 6-year-old.” The teacher’s aide told the grand jury that she contacted child protective services (CPS) after Arabella arrived at school school in the same dirty clothes on several occasions. She also told CPS that Arabella wasn’t allowed to eat fruit, accept rewards or participate in recess with other children. “And the lady from CPS said to me on the phone — after I told her everything, she said, ‘Well, it could be worse,’” the teacher’s aide told the grand jury. Really? I don’t think most members of the public would agree.
Notes
In fact, child welfare systems initially involved White children only. Black children were originally excluded from public child welfare systems. ↩︎
Both Colorado and Wisconsin release information on cases meeting this description. ↩︎
The Texas Department of Family and Protective Services has reported a dramatic decline in child maltreatment fatalities from 199 in FY 2021 to 99 in FY in 2024. Perhaps most surprising about the purported decline in fatalities is that it occurred alongside a massive drop in the number of children placed in foster care from 16,028 in Fiscal Year 2021 to 9,623 in Fiscal Year 2022, with similar numbers of children placed in 2023 and 2024.
Supporters of recent changes in Texas law regarding child maltreatment were quick to highlight these findings as evidence that foster care can be greatly reduced or eliminated with no adverse effects on child safety.
But these claims do not stand up under careful scrutiny. Changes to policy and practice can result in dramatic year-to-year changes in official counts of child maltreatment fatalities, and Texas has implemented at least three significant policy or practice changes during this period.
First, a Texas law that took effect September 21, 2021 tightened the definition of neglect to require the presence of “blatant disregard” for the consequences of an act or failure to act that results in harm to the child or that creates an immediate danger to the child’s physical health or safety. This new requirement means that deaths that would have been attributed to maltreatment prior to the law change are now not investigated at all or not confirmed as maltreatment. Indeed, DCF cites this changed definition as one cause of the decline in reported fatalities between FY 2021 and FY 2024.
Child fatality numbers were also affected by a practice change implemented by DCF that involves the way the agency handles reports of child fatalities. Previously, DCFS assigned all child death reports it received for a full investigation. But starting in September 2022, reports to the Texas Child Abuse Hotline that involve a child fatality but include no explicit concern for abuse and neglect are treated as “Case Related Special Requests,” requiring field staff to confirm that the reporter or first responders had no concern for abuse or neglect. If there are any concerns for abuse or neglect, the child fatality is then sent for a full investigation, but otherwise there is no further action. DFPS reports that the number of child fatalities it investigated decreased from 997 in FY2022 to 690 in FY2023 and 587 in FY 2024. DFPS attributes this decline in investigations to both this practice change and to the legislature’s change in the definition of neglect.
There is one newer policy change that DFPS announced in its recent report. Investigations that are closed “with a disposition of reason to believe for neglect with a fatal severity code” receive a further level of review. It seems possible that this level of review may be reducing the number of reported cases even further.
Given all these policy and practice changes affecting the count of child maltreatment fatalities, It seems highly likely that Texas did not see an actual reduction in these deaths, but rather reclassified them as not due to child maltreatment. Perhaps it is not surprising that neither DFPS nor the supporters of weaker child protection are interested in exploring what is really happening to vulnerable children in the aftermath of the drastic decline in the use of foster care.
This post was originally published as a guest commentary in the Baltimore Sun.
Last month, the Baltimore Banner reported on an alarming rise in the number of child fatalities due to maltreatment in Maryland, as shown by a federal report. The number of child abuse and neglect deaths reported by Maryland to the federal Children’s Bureau was 83 for Fiscal Year 2023, up from 27 a decade before, a rate higher than any state but Mississippi.
After initially responding with confusion, the Maryland Department of Human Services (DHS) explained that the numbers it reported to the feds were erroneous. Actually, the state was aware of 47 children who died of abuse or neglect in 2023, which was still a 75% increase from 2013. “We continue to discover where data was routinely released without any validation or reconciliation,” a deputy DHS secretary told the Banner.
But members of the legislature were already alarmed and began talking about withholding funds until the agency was able to report accurate data about child fatalities as well as the conditions of children in foster care. Eager to demonstrate its desire for transparency, DHS announced that it was pivoting to support a bill requiring the agency to promptly release information about children in foster care who die from suspected maltreatment.
But this legislation would not apply to children who died while in the custody of their parents or guardians. It would not apply, for instance, to five-year-old Zona Byrd, who starved to death last year after being returned to her parents’ custody; four-year-old Amir James, who arrived at the hospital covered in cuts and bruises and died from skull fractures that caused his brain to bleed, while his twin brother survived similar injuries; 16-month-old Zavier Giron, who had several broken ribs, a dislocated femur and a perforated intestine when he died; and two-year-old Charlee Gamble, who was shot in the head by an unsecured gun that her father purchased illegally and left on a TV stand. The bill would apply only to cases of abuse or neglect in foster care — even though they are a rare occurrence. Indeed, less than 1% of perpetrators of child maltreatment fatalities reported nationwide for Fiscal Year 2023 were foster parents or staff of a group home or residential treatment facility.
The chair of the Maryland House Judiciary Committee conducting a hearing on the bill wondered if the bill was too narrow, but one of the sponsors, Del. Susan McComas, responded, “Whether it’s a little step or a big step, I don’t really care. I think we need to do something. And I think we could start with just this.”
The sentiment to do something is admirable, but in this case it will likely not even make a dent in the lack of public accountability and transparency when children die of maltreatment.
To prevent such tragedies, we need improved data collection, timely notification and greater transparency by agencies that investigate such fatalities and are responsible for protecting children. Maryland should pass a bill that requires prompt notification of any child fatality that has been reported to child protective services. Eleven other states already do this. Without such notifications, legislators and the public may never know about some child abuse deaths, especially those that did not result in criminal charges. In addition, DHS should be required to respond promptly to requests for further information about all suspected child maltreatment fatalities, not just those where the child was in foster care or state custody. It is only by achieving such transparency that DHS can work with the legislature, researchers and child advocates to prevent these tragic events in the future.
The death of Gavin Peterson from starvation last year after years of abuse and multiple calls to child protective services regarding his treatment set off an outcry in Utah and around the country. Media reports appeared throughout the country, legislators expressed their outrage, hearings were held, and concerned citizens rallied. But halfway through the legislative session that followed Gavin’s death, it appears that there will be no policy changes that will prevent more children suffering Gavin’s fate. Instead, his name has been invoked to support bills that would not have saved him, and, ironically, legislation that could increase the risks for children like Gavin who are withdrawn from school seems poised for passage.
As described in an earlier post, Gavin Peterson died of starvation in July 2024 at the age of 12, almost a year after his father and stepmother withdrew him from school, ostensibly to homeschool him. Gavin had been the subject of multiple reports to the Utah Division of Child and Family Services (DCFS), including at least four reports from his school describing him as eating food from the trash and with other signs of neglect and abuse. An investigation found no maltreatment but did result in his father and stepmother withdrawing him from school, a common response of abusive parents to being investigated, and too often a precursor of a child’s death from abuse. Gavin’s withdrawal from school was his death warrant, because there were no more caring adults to report on his suffering.
There are several types of legislation that might have helped prevent future Utah children suffering Gavin’s fate. Perhaps most effective would be to increase the protections for homeschooled children. For example, the Make Homeschool Safe Act developed by the Coalition for Responsible Home Education proposes that no person who has been found to have engaged in child abuse or neglect can operate a home school. It is not clear from the limited information provided by DCFS whether Gavin’s stepmother had been found to have committed abuse or neglect, but given that a case was open on the family for a year, it seems likely that she was. In addition, the bill would allow no person to withdraw a child from school for homeschooling within three years of an investigation of potential abuse or neglect unless there is a risk assessment by a child protective services worker and monthly risk assessments for the first 12 months of the child’s withdrawal from school. Such a law, if implemented faithfully, might well have saved Gavin.
But far from placing controls on homeschooling, Utah legislators are bent on removing them in the wake of Gavin’s death. For the past close to two years, Utah has required parents who homeschool their children to sign an affidavit swearing that they have never been convicted of child abuse. Admittedly, this seems to be a pretty toothless requirement, as compared to requiring a check of police and CPS records. But the homeschooling community has decided that even this weak law is offensive, as the Salt Lake Tribune has reported. Homeschooling families thronged the Capitol on February 25 to demonstrate their support for a bill that would eliminate this requirement. Its sponsor, Representative Noeleen Peck, justified the bill by saying the requirement “didn’t work” and was “confusing.” Some districts misinterpreted it to require a background check, she said. Perhaps that misinterpretation–giving the requirement teeth after all–explains the overwhelming support for this bill among homeschooling parents. The Committee voted unanimously to recommend the bill eliminating the requirement.
One bill (HB83) that did get introduced in Gavin’s name would not have protected him, despite being a good bill. It would make it easier for police or social workers to obtain a warrant to view a child and a home for the purposes of investigating a report of child abuse or neglect. This bill addresses a real problem in Utah which gained attention through another horrific abuse case in the same year. Parenting influencer Ruby Franke was starving and torturing her two youngest children. Police tried to check on them, but Franke would not respond to the door and a judge would not issue a warrant to allow them to enter the home. HB83 presumably would have enabled police to obtain a warrant to enter the Franke home and perhaps discover the children’s plight.
The sponsor of HB83, state Rep. Christine Watkins, told the House Judiciary Committee that this bill was in direct response to the cases of Gavin Peterson and the children of Ruby Franke. But the case history that was released by DCFS describes no instance of police or DCFS being denied access to Gavin’s home. DCFS visited the home twice in March, 2023 and interviewed Gavin outside the presence of his parents. But he did not disclose the abuse, probably for fear of retaliation by the abusers. Certainly the difficulty of accessing children at home is a problem worth correcting, but it was not apparently related to Gavin’s death. In any case, the bill did not make it out of its first committee hearing and does not seem likely to advance.
Sadly, it appears that the most consequential bill that will be passed in response to Gavin’s death is a measure that would eliminate the cost of reduced-price school lunches. The bill’s sponsor, House Rep. Tyler Clancy, told KJZZ that Gavin Peterson’s death helped build support for the bill. “It shakes you to your core when you read a story about a young person like Gavin Peterson starving to death,” Clancy said. Clancy’s compassion is commendable, but this bill would not have helped Gavin, who died almost a year after he was removed from school. There is something disturbing about using Gavin’s name to support a bill, however beneficial, that wouldn’t have helped him.
It is hard to understand how well-intentioned legislators, in the aftermath of a tragedy like Gavin Peterson’s death, can use his name to support legislation (no matter how worthwhile) that would not have prevented the tragedy in the first place. Whether it is the lack of bandwidth among legislators and staff or the dominance of preconceived notions about what constitutes the problem. It’s even harder to understand legislators voting to reduce protections for children who are withdrawn from school less than a year after Gavin’s death. The Utah Legislature is not unique in its failure to produce meaningful reforms after tragic failures in child protection. But it is the children trapped in their houses of horror that must pay the price.
“New Federal Report Demonstrates Reduction in Child Maltreatment Victims and Underscores Need for Continued Action,” the Administration on Children and Families (ACF) of the US Department of Health and Human Services proclaimed in releasing the latest annual report on the government response to child abuse and neglect. As in the past several years, ACF’s language suggested that child abuse and neglect are decreasing. But with states around the country changing law, policy and practice to reduce child welfare agencies’ footprint, the number of “child maltreatment victims” cited by ACF is likely more a reflection of policy and practice than an indicator of actual maltreatment.
The annual Child Maltreatment reports, produced by the Children’s Bureau of ACF, are based on data that states submit to the National Child Abuse and Neglect (NCANDS) data system. The new report, Child Maltreatment 2023 (CM2023), provides data for Federal Fiscal Year (FFY) 2023, which ended on September 30, 2024. The report documents the funnel-like operations child welfare protective services (CPS), which at each stage select only a fraction of the cases or children to proceed to the next stage. Exhibit S-2 summarizes the findings of the newest report. Child welfare agencies received 4.399 million “referrals” alleging maltreatment in Federal Fiscal Year (FFY) 2023 and “screened in” 2.1 million of them as “reports” for “disposition” through an investigation or alternative response. The investigation or assessment of those reports resulted in a total of 546,159 children determined to be victims of child abuse and neglect. (The final stage of the funnel involves services and is not covered in this post.) State and local policies and practice affect every stage of this process, as explained in detail below.
Referrals
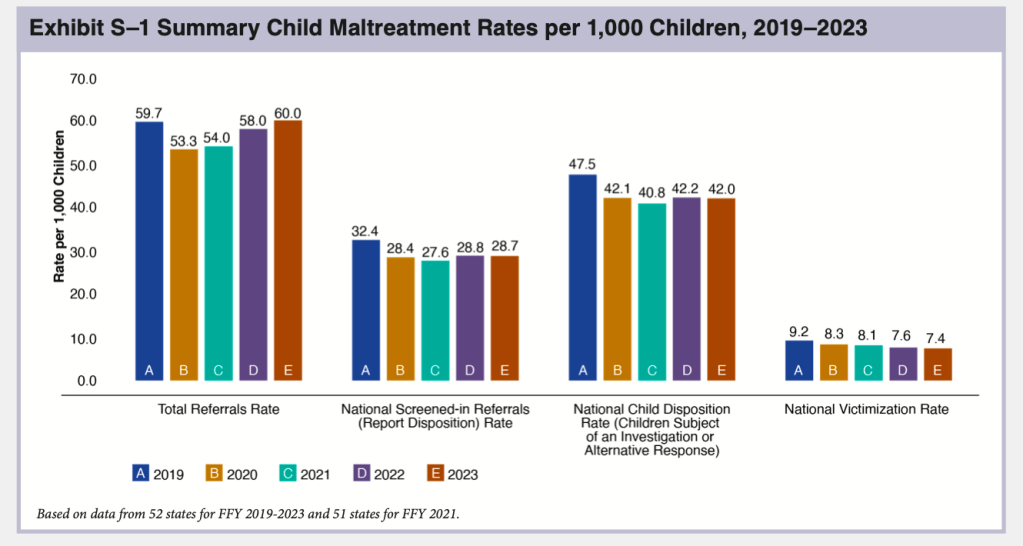
NCANDS uses the term “referrals” to mean reports to child welfare agencies alleging maltreatment. Agencies received an estimated total of 4,399,000 referrals through their child abuse hotlines or central registries in FFY 2023, according to CM 2023. This is a very slight increase over the previous year and represents about 7.8 million children, or 60 per 1,000 children. As shown in Exhibit S-1, the total number of referrals has been increasing since 2020, when the COVID-19 pandemic resulted in a large drop in referrals. In FFY 2023, the number of referrals surpassed the pre-Covid 2019 total for the first time as the lingering effects of the pandemic, which acted to suppress reports, finally dissipated.
As in past years, the state-by-state tables document large differences in referral rates, from 19.9 per 1,000 children in Hawaii to 171.2 per 1,000 in Vermont–also the top and bottom states in 2022. These differences reflect not just different numbers of calls to child abuse hotlines but also state policy and practice. Vermont reports that it counts all calls to the hotline as referrals, while other states do not do so. For example, Connecticut reported in CM2022 that none of the calls that are assigned to alternative response are included in NCANDS, resulting in a far lower number of calls than the number they actually receive. Referral rates may also affected by a state’s policy on who is required to report and what must be reported. Such policies are disseminated to mandatory reporters through training and agency communications. New York reported implementing in FFY 2023 a new training for mandated reporters that helps them identify when concerns do not rise to a level legally requiring a report be made.” The training also focuses on implicit bias in order to “reduce the number of SCR reports influenced by bias about race or poverty.” The number of referrals in New York dropped by a very small fraction in FFY 2023. Missouri reported in CM2022 that it stopped accepting educational neglect referrals in 2021 as the COVID emergency ended, resulting in a decreased number of referrals received the following year.
Reports
Once a state agency receives a referral, it will be screened in or out by agency staff. In general, referrals are screened out if they are deemed not to contain an allegation of child abuse or neglect, contain too little information to act on, are more appropriately assigned to another agency, or for some other reason do not fall under the mandate of the child welfare agency. In the language used by NCANDS, a referral becomes a “report” once it is screened in. “Reports” are assigned for an investigation or “alternative response.” State data indicates that child welfare agencies screened in 2.1 million referrals, about 47.5 percent of referrals for an investigation or alternative response, and “screened out” the other 52.5 percent as not warranting a response. The number of screened-in referrals was 11.6 percent less than in FFY 2019 and slightly less than in FFY 2022.
A total of 42 states reported a decrease in the number of screened-in referrals in FFY 2023. In their commentaries, several of these states described policy and practice changes that led to their screening out more referrals. Ohio reported that two of its major metropolitan counties, which had significantly higher screen-in rates than the rest of the state, adjusted their screening procedures to be consistent with the rest of the state, resulting in a lower screen-in rate in those counties and statewide. Mississippi reported an increasing the amount of screening it conducted, especially when a report was received regarding a case that was already open; perhaps this is why its screen-in rate dropped from 41.3 to 36.5 per 1,000 children. Nebraska reported dropping a policy to require accepting all referrals from a medical professional involving children under six. Some states explicitly reported that their screening changes were adopted in order to decrease the number of screened in referrals. Kentucky reported adopting a new SDM® screening tool designed to decrease the number of referrals that are “incorrectly accepted for investigation.” Nevada reported a decrease in screened-in referrals because it established new intake processes to ensure that referrals are screened out when they do not meet criteria for acceptance.
“Victims”
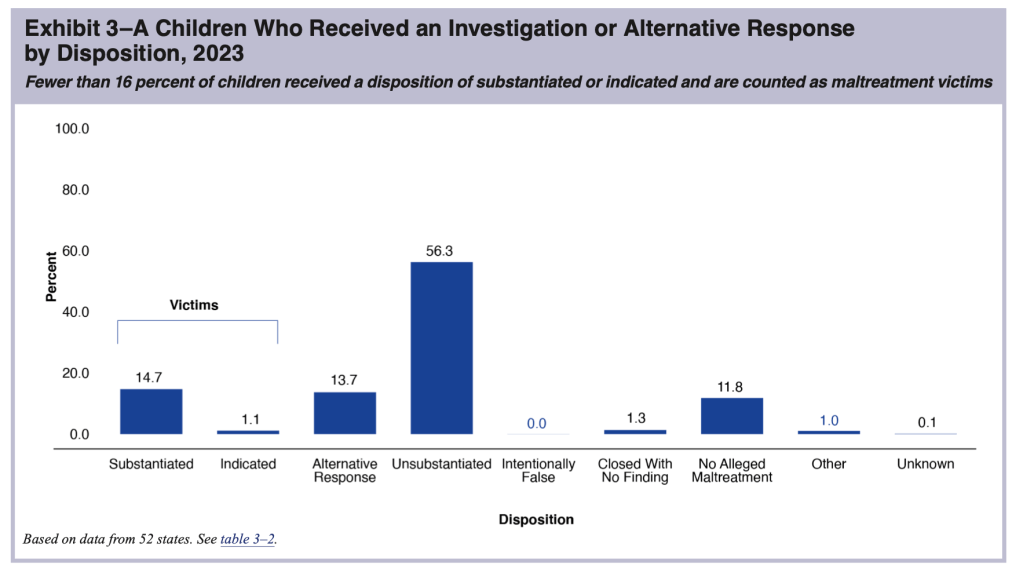
The next phase in the funnel of CPS is the determination of whether abuse or neglect has occurred. At this stage, the level of analysis shifts from the case to the child, and the number of “victims” is the result. In NCANDS, a “victim” is defined as “a child for whom the state determined at least one maltreatment was substantiated or indicated1; and a disposition of substantiated or indicated was assigned for a child in a report.” “Victims” include children who died of abuse or neglect if the maltreatment was verified. Some children receive an “alternative response”2 instead of an investigation; these children are not counted as victims. According to CM2023, states reported a total of 546,159 victims of child abuse and neglect in FY 2023, producing a “victimization rate” of 7.4 per 1,000 children.
The number of “victims” reported by states according to the NCANDS definition does not represent the true number of children who experienced abuse or neglect, which is unknown. Many cases of child maltreatment go unreported. Children assigned to alternative response are not found to be victims unless their case is reassigned to the investigation track. And finally, substantiation may not be an accurate reflection of whether maltreatment occurred. Making a determination of whether maltreatment occurred is difficult. Adults and children do not always tell the truth, the youngest children are nonverbal or not sufficiently articulate to answer the relevant questions. So it is not surprising that research suggests that substantiation decisions are inaccurate3 and a report to the hotline predicts future maltreatment reports and developmental outcomes almost as well as a substantiated report.4
State “victimization rates” range from a low of 1.5 per 1,000 children in New Jersey to a high of 16.2 in Massachusetts. It is unlikely that Massachusetts has more than ten times more child abuse and neglect victims than New Jersey–a not dissimilar Northeastern state. Policy and practice must be at play, including different definitions of abuse or neglect, levels of evidence required to confirm maltreatment, and policies regarding the use of alternative response or “Plans of Safe Care”5 to divert children from investigation, among other factors. Maine reported the second highest “victimization rate.” The Maine Monitor asked experts why this might be so. Among the reasons suggested were the definition of maltreatment; Maine allows abuse or neglect to be substantiated when there is a “threat” of maltreatment, even if there is no finding that it already occurred. In view of the deceptiveness of these terms, I have put the terms “victims” and “victimization rates,” when not preceded by the word “reported,” in quotation marks in this post.
The national “victimization rate” of 7.4 per 1,000 children, is a small decrease from 7.7 in FFY 2022 and the total number of reported “victims” was 19.3 percent less than the total reported in FFY 2019. This “victimization rate” has declined every year since FFY 2018. Of course, this decline is in part a result of the decline in the number of screened-in referrals that was discussed above. Any referral that is screened out is one less reported “victim,” even though some percentage of the screened-out referrals almost certainly reflected actual incidents of maltreatment.6 It is also clear that changes in policy and practice have contributed to the decline in the number of “victims” reported by states, as described below.
Policy and practice changes affecting “victimization” numbers
The change in the number of “victims” between FFY 2019 and FFY 2023 ranged from a 52 percent decrease in North Dakota to a 32 percent increase in Nevada, suggesting that these changes may reflect policy and practice more than actual trends in abuse and neglect. And indeed, two of the largest states made it more difficult to substantiate maltreatment in FFY 2022, and both found a decline in the number of maltreatment victims. In Texas, the legislature narrowed the definition of neglect, requiring the existence of both “blatant disregard” for the consequences of a parent’s action or inaction and either a “resulting harm or immediate danger.” Perhaps this helps account for the drop in the number of reported victims from 65,253 in FFY 2021 to 54,207 in FFY 2022. But the number of victims actually rose very slightly in FFY 2023. Perhaps the new definition had been assimilated into practice and was no longer resulting in a decrease in substantiations. In New York, the level of evidence required to substantiate an allegation of abuse or neglect was changed from “some credible evidence” to “a fair preponderance of the evidence” in FFY 2022. The number of victims found in New York dropped from 56,760 in FFY 2021 in to 50,056 in FFY 2022, which the Office of Child and Family Services attributed in its CM 2022 commentary to that change in evidentiary standards. The number of reported victims fell further to 46,431 in FY2023; perhaps the changed evidentiary standards were continuing to take hold or other state policies affecting other parts of the funnel–such as the attempt to rein in mandatory reporting–were contributing factors. The agency did not address this issue in its 2023 commentary.
A few states did mention in their CM 2023 commentary changes in policy or practice that might have contributed to changes in the number of “victims” in FFY 2023. North Dakota attributes a decrease partly to a change in state statute and policy which allows protective services to be provided when impending danger is identified, even without a substantiation. The agency appears to believe that workers are not substantiating as many reports now that they do not need a substantiation to provide services. Arkansas attributed a decrease in victims to the adoption of a new assessment tool that may have contributed to the routing of more reports to the differential response pathway. Kentucky reported that the adoption of new “Standards of Practice” may have contributed to the increase in the number of “victims” reported in FFY 2023.
Fatalities
Based on reports from 49 states (all but Massachusetts), the District of Columbia, and Puerto Rico, CM2023 estimated a national maltreatment fatality rate of 2.73 per 100,000 children. That rate was then applied to the child population of all 52 jurisdictions and rounded to the nearest 10 to provide a national estimate of 2,000. But experts agree that the annual estimates of child fatalities from NCANDS significantly undercount the true number of deaths that are due to child maltreatment. I discussed this in detail in A Jumble of Standards: How State and Federal Authorities Have Underestimated Child Maltreatment Fatalities.
The annual fatality estimates presented in the report increased by 12.3 percent between FFY 2019 and FFY 2022 and then fell slightly from 2,050 to 2,000 in FFY 2023, a fact that ACF mentioned in its press release. Such a small reduction of less than three percent over the previous year cannot be statistically distinguished from random fluctuation, especially because it is based on much-smaller numbers from the individual states. State commentaries illustrate the randomness of these year-to-year changes. In CM 2022, two individual states explained year-to-year jumps in fatalities by explaining that many children in one family died and that a large group of fatalities that occurred the previous year were reported in the current year. But even aside from statistical fluctuations, there are many reasons one cannot rely on year-to-year changes. These include the timing of reports and changes in policy and practice.
Timing
According to CM 2023 (and previous reports), “The child fatality count in this report reflects the federal fiscal year (FFY) in which the deaths are determined as due to maltreatment. The year in which a determination is made may be different from the year in which the child died.” The authors go on to explain that it may take more than a year to find out about a fatality, gather the evidence (such as autopsy results and police investigations) to determine whether it was due to maltreatment, and then make the determination. Alabama, for example, explained in its commentary that the deaths reported in a given year may have occurred up to five years before.
To add to the uncertainty around timing, the writers of CM 2023 are not exactly correct when they state that all states report on the fatalities determined in the reporting year. In their annual submissions to NCANDS, several states add fatalities for the previous year, implying that their practice is to report on fatalities that occurred in a specific time period, not those determined in the applicable year. Four states revised their number of 2022 fatalities in their submissions to CM2023. This suggests that their 2023 reports are in turn incomplete and will be revised in succeeding years. California, for example, explained that:
Calendar Year (CY) 2022 is the most recent validated annual data and is therefore reported for FFY 2023. It is recognized that counties will continue to determine causes of fatalities to be the result of abuse and/or neglect that occurred in prior years. Therefore, the number reflected in this report is a point in time number for CY 2022 as of December 2023 and may change if additional fatalities that occurred in CY 2022 are later determined to be the result of abuse and/or neglect.
So California is reporting (for CM 2023) a truncated count of child maltreatment deaths for Calendar Year 2022. But it did add 12 fatalities to the count of fatalities that it reported for FFY 2022, raising its total from 164 to 176. California reported 150 fatalities for FY2023; one can assume that additional deaths will be reported in the next report. The four states together added 56 deaths for FFY 2023. Arizona’s total increased from 14 to 39, Maine from three to 10 and Virginia from 39 to 51. .
Policy and Practice: Fatality Definition and Measurement
In addition to timing issues, year-to-year changes in fatality counts can reflect changes in how states screen or define child maltreatment fatalities. In previous issues of CM, states have reported on improvements in their collection of fatality information. Over time, some states have eliminated obsolete practices in screening and information collection. West Virginia reported in its 2016 commentary that it had begun investigating child fatalities in cases where there were no other children in the home. North Carolina ended its restrictive policy of reporting only fatalities determined by a chief medical examiner to be homicide, and it also began efforts to incorporate vital statistics and criminal justice data.
During FY 2023, some states reported changes that may have resulted in a reduced number of child fatalities reported.
Texas did not submit commentary for FFY 2023. But as reported above, it changed its screening policy so that reports involving a child fatality but include no explicit concern for abuse and neglect are not investigated if the reporter and other pertinent sources had no concern for abuse or neglect. DFPS reports that the number of child fatalities it investigated decreased from 997 in FY2022 to 690 in FY2023 (a 31 percent decrease) due to this new screening policy. And the number of child maltreatment fatalities fell from 182 to 164. But with a drastic drop in foster care placements in Texas, there is reason to fear that maltreatment fatalities increased rather than decreased. If that is the case, this change screening policy may have resulted in the failure to investigate and confirm actual maltreatment deaths..
The Illinois Division of Child Protection reported that it added a new administrative review process for sleep-related deaths. A senior administrator reviews the investigation to ensure that death included evidence of “blatant disregard.” DCF links this new policy with a decrease of 24.6% in reported child fatalities in FFY 2023.
Other states reported changes that might result in an increased number of child fatalities reported. Maryland attributed an increase in reported fatalities to a policy change requiring local agencies to screen in sleep-related fatalities as part of its prevention effort. Alaska reported a change that may affect fatality counts in future years: in December 2023 the agency dropped its practice of screening out cases where no surviving children remained in the home; from now on the agency will be making maltreatment findings even when there are no surviving children.
It is regrettable that most state commentaries do not include explanations for the changes in their reported number of referrals, reports, and victims. Worse, several states do not even submit commentaries in time to be included in each year’s report. In CM023, commentaries are missing for Arizona, Hawaii, Kansas, New Hampshire, North Carolina, Oregon, Texas, and West Virginia. Given the importance of the state commentaries for understanding the data they submit, the preparers of the CM reports should reach out to agency personnel in states that have not submitted commentaries by a certain date or have not answered the important questions and ask the questions directly directly. This information is too important to be left out.
It is unfortunate that ACF continues to misuse term “victimization” and “victimization rate” to suggest that child maltreatment (including fatalities) is declining, particularly in its press release and executive summary, which do not provide any explanation of the true meaning of the terms. The deceptive language is not a surprise given the previous Administration’s desire to take credit for ostensible and support the prevailing narrative regarding the need for a reduction in interventions with abusive and neglectful families. One does not have to be a statistician or data scientist to realize that we will never get an accurate measure of child maltreatment because so much of it occurs behind closed doors. Finding fewer victims is one way to reduce CPS intervention in the lives of vulnerable children–and to deny that the reductions are harmful. Sadly, this report will be used as evidence to support policies that continue to roll back protections for our most vulnerable children.
Notes
Substantated is defined as “supported or founded by state law or policy.” “Indicated” is a less commonly used term meaning a “disposition that concludes maltreatment could not be substantiated understate law or policy, but there is a reason to suspect that at least one child may have been maltreated or is at risk of maltreatment.” ↩︎
An “alternative response” includes an assessment and referral to appropriate services if the parent agrees to participate. There is no determination on whether abuse or neglect occurred and no child removal unless the case is transferred to the investigative track. ↩︎
Theodore Cross and Cecilia Casanueva, “Caseworker Judgments and Substantiation,” Child Maltreatment, 14, 1 (2009): 38-52; Desmond K. Runyan et al, “Describing Maltreatment: Do child protective services reports and research definitions agree?” Child Abuse and Neglect 29 (2005): 461-477; Brett Drake, “Unraveling ‘Unsubstantiated,’” Child Maltreatment, August 1996; and Amy M. Smith Slep and Richard E. Heyman, “Creating and Field-Testing Child Maltreatment Definitions: Improving the Reliability of Substantiation Determinations,” Child Maltreatment, 11, 3 (August 2006): 217-236. ↩︎
Brett Drake, Melissa Jonson-Reid, Ineke Wy and Silke Chung, “Substantiation and Recidivism,” Child Maltreatment 8,4 (2003): 248-260; Jon M. Hussey et al., “Defining maltreatment according to substantiation: Distinction without a difference?” Child Abuse and Neglect 29 (2005): 479-492; Patricia L. Kohl, Melissa Jonson-Reid, and Brett Drake, “Time to Leave Substantiation Behind: Findings from a National Probability Study,” Child Maltreatment, 14 (2009), 17-26; Jeffrey Leiter, Kristen A. Myers, and Matthew T. Zingraff, “Substantiated and unsubstantiated cases of child maltreatment: do their consequences differ?” Social Work Research 18 (1994): 67-82; and Diana J. English et al, “Causes and Consequences of the Substantiation Decision in Washington State Child Protective Services,” Children and Youth Services Review, 24, 11 (2002): 817-851. ↩︎
Plans of Safe Care are voluntary plans offered to the families of substance-exposed infants under the Comprehensive Addiction and Recovery Act (CARA). ↩︎
We. know this from child fatality reviews that many children who die have been the subject of previous referrals, which were not substantiated but later found in fatality investigations to have been correct. See discussions of the deaths of Thomas Valva and Gavin Peterson, for example. ↩︎
“B.B.” was born in 2022 and died of fentanyl poisoning in March 2023. During the ten years before B.B.’s death, DCYF had received 30 reports on B.B.’s family (many before B.B. was born) for issues including use of heroin, marijuana and alcohol in the home; lack of supervision of the children; domestic violence; an unsafe caregiver living with the family; an unsafe and unclean living environment unsecured guns in the home “out-of-control” behaviors by B.B.’s older siblings at school, with the mother described as “out-of-it” and unresponsive to school concerns; concerns about the children’s hygiene; and the mother driving under the influence of marijuana. An in-home services case that had been open since January 2023 was closed days before B.B.’s death.
On August 24, 2024, the Washington Department of Children, Youth and Families (DCYF) proudly announced in a press statement that it had reduced the number of children in out-of-home care by nearly half since 2018. Specifically, the number of children in foster care had fallen from 9,171 in 2018 to 4,971 as of August 14, 2024. “Outcomes like this demonstrate our agency’s commitment to keeping families together and children and youth safe,” DCYF Secretary Ross Hunter said. “Although the number of reports we are receiving remain [sic] consistent, we are seeing fewer children and youth in out-of-home care as families are being referred to support services rather than having children removed from their homes. Indeed, “safely reduce the number of children and youth in out of home care by half” (without a baseline date from which this can be measured) is one of DCYF’s six strategic priorities. But treating the decline in foster care (the direct result of government actions) as a desirable outcome in itself can contribute to a disregard of actual child welfare outcomes like safety and permanency.
How did DCYF reduce foster care by nearly 50 percent?
How did DCYF manage to slash its foster care rolls so radically in such a short time? Without providing specifics, the press release cites DCYF’s implementation of the Family First Prevention Services Act (FFPSA) and its emphasis on “supporting and collaborating with families by providing access to services and programs.” A DCYF spokesperson told the Seattle Timesthat the department was using services to avoid removing children or to reunite families sooner, citing efforts to connect parents to substance use or mental health treatment programs, bring a social worker into the home to “problem solve,” or “offer practical items, like diapers, car seats and beds.”
Apparently not satisfied with the changes implemented by DCYF, the Washington legislature in 2021 passed the Keeping Families Together Act (KFTA, also known as HB 1227), which took effect on July 1, 2023. Among other provisions, KFTA increased the standard for the court to order removal of a child from the home, which previously required the agency to demonstrate that “reasonable grounds that the child’s “health safety or welfare will be seriously endangered if not taken into custody and that at least one of the grounds set forth demonstrates a risk of imminent harm to the child.” As amended by KFTA, the law now requires the agency to demonstrate “that removal is necessary to prevent imminent physical harm to the child due to child abuse or neglect.” The petition for removal is required to contain “a clear and specific statement as to the harm that will occur if the child remains in the care of the parent, guardian or custodian, and the facts that support the conclusion.” Moreover, the court must consider whether participation by the parents or guardians in “any prevention services” would eliminate the need for removal. If so, they must ask the parent whether they are willing to participate in such services and shall place the child with the parent if the parent agrees.
On a page dedicated to KFTA implementation, DCYF explains that it has implemented the law by adopting new policies and procedures to determine whether to remove a child and by training and supporting staff to implement the new procedures and determine whether there is an imminent risk of serious harm to the child. DCYF reports that internal reviews show that staff are “taking additional steps to prevent removal of a child and to support a safety plan for the family.”
Shortly before KFTA took effect, DCYF, along with the Department of Health, the Health Care Authority, and the Washington State Hospital Association issued new guidelines to birthing hospitals and mandatory reporters. These guidelines stated that infants born substance exposed, but for whom there are no other safety concerns, can receive “voluntary wrap-around services from a community organization” without being reported to CPS. These voluntary services are being provided through federally-mandated “Plans of Safe Care (POSC).” Healthcare providers identifying a substance-exposed infant are instructed to access an online portal where they are directed to call DCYF if safety concerns are identified and to complete a POSC referral if not.
DCYF has been issuing quarterly data updates to assess the impacts of the KFTA. According to the most recent (October 2024) update, the law is having the intended impact of further reducing removals to foster care. DCYF reports a 16 percent decrease in the number of children removed in the July through September quarter of 2024 compared to the same quarter of 2022, before passage of KFTA. However, comparing foster entries for all ages in July through September 2024 to those in the same quarter of the previous year, the data indicate that foster care entries actually increased! Will this be the beginning of the end of the foster care reductions? That remains to be seen.
A longer-term view raises questions about the difference KFTA made, compared to the previous and ongoing efforts by DCYF to reduce foster care placements. Entries into foster care in Washington have decreased annually from 2017 to 2024, as shown in the chart below. The rate of decrease remained about the same between 2019 and 2024, while KFTA was not implemented until July 2023. Perhaps more children would have entered care if not for KFTA, but there is no way to assess the impact of KFTA as compared with DCYF’s ongoing effort to reduce removals.
The reduction in foster care placements was supposed to be accompanied (and made possible) by an increase in in-home services (which DCYF calls Family Voluntary Services or FVS), and DCYF reports that the number of cases receiving FVS increased by nine percent from 1,809 in SFY2023 to 1,994 in SFY2024. This increase in FVS cases cannot be compared to the 17-percent decrease in children placed in foster care over the same period, as the unit of analysis is different (families rather than children). But the key question is the nature and intensity of these services and whether they really kept the children safe.
The cost of foster care reductions
The purpose of foster care is to keep children safe when they cannot be protected at home. So the essential question is whether the reduction in foster care placements has occurred without any cost to children. Trends in child fatalities and “near fatalities”1 due to child abuse or neglect can provide a clue. These deaths and serious injuries are the tip of the iceberg of abuse and neglect. For each child who dies or is seriously injured, there are many more that are living in fear, pain, or hunger, and incurring lifelong cognitive, emotional, and physical damage. There are troubling signs of an increase in child fatalities and near fatalities over the past several years. In its most recent quarterly update, DCYF reports on the number of “critical events” or child fatalities and near fatalities that met its criteria for receiving an “executive review.” These include the deaths of any minor that had been in DCYF custody or received services within a year of the death that were suspected to be caused by child abuse or neglect.2 They also include near fatality cases in which the child has been in the care of or received services from DCYF within three months preceding the near fatality or was the subject of an investigation for possible abuse or neglect. DCYF reports that the number critical events it reviewed increased from 23 in 2019 to 51 in 2023 and projects that it will increase to 61 in 2024.3
The increase in critical events reflects, in part, the growing opioid crisis in Washington, as well as decisions Washington has made regarding how it intervenes to protect children. Opioid related emergencies have “dramatically increased for the entire population (adults and children) in Washington,” and children have not been immune. Fentanyl is particularly dangerous to young children because it takes only a tiny amount to kill a baby or toddler, who can mistake the pills for candy or put straws or foil meant for smoking the drug in their mouths. The number of fatalities and near fatalities reviewed by DCYF that involved fentanyl climbed from four in 2019 to a projected 35 in 2024. Since 2018, Washington’s Office of the Family and Children’s Ombuds (has observed an annual increase in child fatalities and near fatalities involving accidental ingestions and overdoses. Fifty-seven (or 85 percent) of the 67 incidents examined in 2023 involved fentanyl. Over half of these incidents involved children under three years old and a shocking 14 out of the 85 infants were 12 months old or less. As Dee Wilson and Toni Sebastian point out, the limited mobility and motor skills of infants suggests that some of these infants may have been given a small amount of fentanyl as a means of sedation.
The Washington Legislature was concerned enough about the possibility that KFTA is contributing to an increase in child fatalities and near fatalities in the context of the fentanyl epidemic that it passed a new law (SB 6109) in 2024. The law provides that a court must give “great weight” to the “lethality of high-potency synthetic opioids.….in determining whether removal is necessary to prevent imminent physical harm to the child due to child abuse or neglect.” However, it appears that there is confusion about exactly what that means.
Has DCYF given up on protecting children?
“We know that supporting and collaborating with families by providing access to services and programs increases their number of protective factors, leading to better outcomes,” said DCYF Assistant Secretary Natalie Green. “Giving families the tools they need to thrive and safely parent means more children and youth remain safely at home.”
But the work of DCYF’s own analysts, in their quarterly KFTA updates, raises doubts about whether DCYF is adequately performing its child protection function. These updates acknowledge that the agency is not removing as many children with a high risk of future encounters with child welfare (in other words, those who have a high risk of being harmed). And they also report that the department has seen “an increasing percentage of moderately high to high risk cases being re-referred to CPS within 90 days of the risk assessment. DCYF also reports that the overlap between KFTA and Plan of Safe Care (POSC) is resulting in fewer screened-in intakes involving substance-exposed newborns because these infants are now being referred to voluntary services under POSC.
There has been a chorus of voices alleging that DCYF is abdicating its child protection responsibilities. One foster parent told the Seattle Times that “she and other foster parents are finding children who now come into their care are in worse shape than they used to be, with more serious mental health conditions or greater exposure to lethal drugs like fentanyl.” She contends they’ve been left too long in unsafe conditions because of the heightened legal standard for removal.In The Erosion of Child Protection in Washington State, Toni Sebastian and Dee Wilson have cited the weakness of the management of Family Voluntary Services, which is often employed as an alternative to foster care.
A survey of executive reviews of 2023 and 2024 child maltreatment child fatalities with DCYF involvement within a year provided examples of problems with screening, investigations, and case management, including the following:
Hotline issues. Reviews documented multiple intakes screened out on the same family even when the family had been the subject of multiple calls. The reviews also suggest that too many cases may be assigned to the Family Assessment Response (FAR) pathway, an alternative to a traditional investigation designed for lower-risk cases. In FAR cases, a social worker assesses the family and refers it to voluntary services. There is no finding about whether maltreatment has occurred and no child removal unless the case is transferred to the investigative track.
Premature closure of FAR cases. Reviewers noted instances in which FAR cases were closed after parents failed to cooperate, without caseworkers considering a transfer to the investigative track or before determining that the parent had followed through with services.
Assessment failures: Reviewers noted multiple failures to adequately assess parents for domestic violence, mental health, and substance abuse; failures to contact collaterals (relatives and friends) and instead relying on parental self-reports; lack of recognition of chronic maltreatment; ignoring evidence of past problems if not included in the current allegation; and failing to anticipate future behavior based on historical patterns.4
Inadequate understanding of substance abuse: Reviewers noted the failure to conduct a full assessment of substance abuse including history, behavioral observations, and collateral contacts; disregarding the unique danger to children posed by fentanyl; downplaying the significance of marijuana use, particularly as an indicator of relapse from harder drugs; and disregarding alcohol abuse because it is legal.
Failure to obtain information from treatment and service providers. The failure to communicate with service providers about clients’ participation in services like drug treatment and relying on clients’ self-reports was noted by more than one review team. Sometimes the providers refused to cooperate. Staff told the team reviewing one case about a substance abuse treatment provider that routinely refuses to cooperate, even when parents sign release forms, and routinely tells clients not to cooperate with DCYF.
Lack of subject matter expertise. Reviewers pointed to the lack of deep knowledge about domestic violence, substance use disorder, and mental health among staff doing investigations, assessments, and case management and the need to provide access to subject matter experts when needed.
Failure to remove a child despite safety threats. The team reviewing the case ofa four-year-old who died after ingesting fentanyl reported that there were at least two different times where an active safety threat was present that would have justified filing a petition in court to place the child in foster care. However, the staff believed, based on past experience, that the court would have denied the petition and therefore did not file.
Delayed Reunifications: “P.L,.” a toddler allegedly beaten to death by his mother, was in foster care for over three years but his mother’s rights were never terminated. He was on a trial return to his mother for just over five months when he was found dead with bruises and burns all over his body.
Staff shortages and high turnover were mentioned as contributing to the observed deficiencies in case practice in almost every fatality review. In B.B.’s case, the reviewers noted that the office had been functioning with a 50 percent vacancy rate for the last several years, stating that such a vacancy rate leads to high turnover, high caseloads, caseworkers with little experience, and supervisors forced to carry cases rather than support their caseworkers. Even caseloads that comply with state standards may be too high. The standard of 20 families per caseworker in FVS was noted to be unmanageable by one review panel, which noted that FVS cases are often discussed as high risk cases and require multiple contacts per month with family members, services providers, and safety plan participants. As Dee Wilson and Toni Sebastian put it, “[b]etting young endangered children’s lives on in-home safety plans developed and implemented by inexperienced and overwhelmed caseworkers is reckless, ill-advised public policy.”
Conclusions and Recommendations
Treating the decline in foster care as a desirable outcome in itself, as Washington and other states have done, is both disingenuous and dangerous. Any government can slash the foster care rolls reducing or ending child removals, as many “child welfare abolitionists” recommend. The central purpose of child welfare services, including foster care, is to protect children from child abuse and neglect. A reduction in foster care placements that results in the failure to protect children is no kind of success.
DCYF told King5 that “the increase in child fatalities and near fatalities in Washington is not being driven by the change in removal standards under House Bill 1227 or the reduction in the number of children in foster care. It is being driven by the increased availability of a highly addictive and hazardous drug and a lack of substance use disorder treatment in our communities.” But whether the agency’s policy or the drug epidemic is more at fault is not the right question. It is DCYF’s job to protect children given the circumstances that exist, including the drug epidemic and the lack of sufficient treatment, keeping in mind that treatment often does not work the first, second, third or subsequent times.
What can be done? DCYF needs to address the workforce crisis, which will probably require increasing pay and improving working conditions, or even possibly relaxing requirements for employment as a caseworker in investigations, assessment, and FVS. DCYF should consider policy and practice changes such as reducing the FVS caseload cap from 20 cases per worker; Instituting a chronic neglect unit, with expert caseworkers and even lower caseloads, for chronic cases; finding a way to limit the use of FAR to cases that are truly low-risk; and promoting the use of dependency petitions for court supervision when children remain in the home, as suggested by two fatality review committees.5 DCYF should request and the legislature should fund a variety of ancillary services for families, starting with therapeutic childcare for all preschool aged children with FVS cases as well as those who have been reunited with their parents. Such childcare would give parents a break and parenting support, keep children safe for a large part of the day, and ensure another set of eyes on the child, among other benefits. Also needed are more residential drug treatment centers where parents can live with their children.
Finally, more transparency is needed so that legislators, advocates and the public have access to the findings of DCYF’s executive review teams. Washington deserves credit for sharing its executive child fatality reviews. But there is no reason that the DCYF should not share its near-fatality reviews as well. We know something about how DCYF failed B.B. and the other children who died. But the public needs access to the reviews of those children who narrowly escaped death as well as those who did not. It is only through such transparency that the public can see the actual impact of all the self-congratulatory proclamations about “safely reducing the number of children in out-of-home care.”
Notes
A “near fatality” is defined by state law as “an act that, as certified by a physician, places the child in serious or critical condition.” ↩︎
DCYF relies on the Office of the Family and Children’s Ombuds (OFCO) to determine whether the fatality appears to have been caused by abuse or neglect, therefore requiring DCYF to conduct a review. ↩︎
Data collected by OFCO are more confusing. OFCO reviews all fatalities and near fatalities in which the child’s family was involved in Washington’s child welfare system within 12 months of the fatality. There number of near-fatalities reviewed by OCFO increased annually from 21 in 2018 to 70 in 2023, according to its most recent annual report on Child Fatalities and Near Fatalities in Washington State. But fatalities reviewed by OFCO did not show the same pattern. They reached a peak of 87 in 2018 and fell sharply in 2019, then rose yearly until they reached 85 in 2022 and then dropped to 79 in 2023. Nevertheless, adding fatalities and near fatalities together shows an alarming increase in critical incidents from 108 in 2018 to 149 in 2023. ↩︎
For example, in the case of “R.W.,” a child who died at age four after ingesting fentanyl, an investigation was closed because the children were staying with relatives, despite the mother’s history of repeatedly removing the children from relatives with whom she had left them. A month later the child was found dead at a motel in the custody of the parents. ↩︎
At least 1,800 children die from abuse and neglect every year, and the total is probably considerably greater. Between a third and a half of these deaths may involve families that were already known to Child Protective Services (CPS) through previous reports of maltreatment. In addition, an unknown number of children are severely injured due to maltreatment every year. Legislators, advocates, and the public need timely information about the circumstances leading to these events so they can identify policy and practice changes necessary to protect children. Decades ago, Congress recognized this need and required states to have a policy allowing for disclosure of information and findings about these tragic events. But due to the weakness of the requirement and the federal government’s lack of enforcement, only a few states make meaningful disclosures in the wake of these horrific events, as documented in a new report.
Federal Law and Policy Regarding Disclosure
In 1996, Congress amended the Child Abuse Prevention and Treatment Act (CAPTA) to ensure that information from child fatalities and near fatalities that are caused by abuse or neglect can be used to correct systemic problems and prevent future occurrences. This provision —42 U.S.C. 5106a(b)(2)(A)(x)—requires that “every state’s plan for spending CAPTA funds contain “an assurance in the form of a certification by the Governor of the State that the State has in effect and is enforcing a State law, or has in effect and is operating a statewide program, relating to child abuse and neglect that includes . . . provisions which allow for public disclosure of the findings or information about the case of child abuse or neglect which has resulted in a child fatality or near fatality.”
This provision has many weaknesses, as described in more detail in a new report called Keeping the Public in the Dark: How Federal and State Laws and Policies Prevent Meaningful Disclosure about Child Maltreatment Fatalities and Near Fatalities, which was prepared for Lives Cut Short, a project to document and direct attention to child maltreatment fatalities. First, the provision requires only that the governor certify the existence of a disclosure requirement, not that it actually exist. Moreover, the language is so vague that it leaves all details to the individual jurisdictions. To make matters worse, the US Department of Health and Human Services (HHS) never wrote regulations to flesh out the vague statutory requirements. Instead, HHS provided guidance in the form of questions and answers in its Child Welfare Policy Manual (CWPM). The CWPM does not have the same force as federal regulations, but some states clearly pay attention to it and have mirrored it in their laws and policies.
Unfortunately the CWPM leaves many questions unanswered and even adds new ones. There are several federal confidentiality requirements embodied in different laws, and the CWPM does not explain the order of preference. Instead, different sections of the CWPM actually contradict each other, with one answer stating that the disclosure requirement trumps previously enacted confidentiality laws and several other answers reminding states to comply with existing confidentiality requirements. To make matters worse, revisions in 2012 introduced new opportunities to avoid disclosure, specifically letting states allow exceptions “in order to ensure the safety and well-being of the child, parents and family or when releasing the information would jeopardize a criminal investigation, interfere with the protection of those who report child abuse or neglect or harm the child or the child’s family.” The exception for “safety and well-being of the child, parents and family” completely undercuts the previous language in the CWPM.
The 2012 revision also included a list of the information and findings to be disclosed, which would have been extremely helpful had it not added a new opportunity to withhold certain information. Specifically, the CWPM (Section 2.1A.4, Question 8) prescribes that states must release:
“information describing any previous reports or child abuse or neglect investigations that are pertinent to the child abuse or neglect that led to the fatality or near fatality; the result of any such investigations; and the services provided by and actions of the State on behalf of the child that are pertinent to the child abuse or neglect that led to the fatality or near fatality.”
This language allows states to withhold information that is actually relevant to the question of whether and how a fatality or near fatality could have been prevented. For example, a state could decide a prior incident of neglect was irrelevant if the cause of death was abuse. But the same parent often perpetrates multiple types of maltreatment, especially chronically maltreating parents who have had multiple encounters with the child welfare system. A state’s decisive intervention in response to prior maltreatment may save a child from death or near-death by another form of maltreatment.
State Laws and Policies Regarding Disclosure
The report reviews state laws and policies governing disclosure of information and findings in cases where child maltreatment resulted in a child fatality or near fatality. The review shows that many state laws and policies fall far short of what is needed to ensure adequate public information about how child protections may have failed. The major findings include:
Despite the federal requirement, not every state has a policy for publicly disclosing findings or information about child fatalities and near fatalities. Out of the 50 states and the District of Columbia, four states appear to have no such policies. Another four states have a policy for fatalities but not near fatalities.
Among the 47 jurisdictions that do have laws or policies for disclosing maltreatment fatality and near-fatality information, only 35 require the release of findings and information about child maltreatment fatalities, and all but four of those require that of near fatalities as well. Twelve allow but do not require the release of findings and information about these incidents.
Many state laws and policies are vague, and many contain restrictions that violate the Congressional intent to make information about child maltreatment and agency operations publicly available.
Seventeen states have laws or policies that require releasing some information without request. These releases vary from a few basic facts on each incident to a comprehensive review of the victim’s family’s history with child welfare. Only nine issue notifications of fatalities or near fatalities that are suspected to be due to maltreatment.1 Without such notifications, the public may not even know an incident has occurred, so they certainly will not ask for information about it.
Recommendations
CAPTA should be amended to clarify the language regarding child fatalities and near fatalities due to maltreatment and establish parameters for states in interpreting the law. The new language should make clear that states must release findings and information about fatalities and near fatalities, and disclosure must be required rather than simply allowed. The law should prescribe the types of information that can be withheld and when disclosure can be postponed, and it should deny states the option of withholding other information or refusing to release information altogether. It should spell out the findings and information that must be released. It should clarify that the CAPTA language overrides other confidentiality provisions in federal law. It should also require that states notify the public of child fatalities and near fatalities that are reported to child abuse hotlines and accepted for investigation.
But recent attempts to reauthorize CAPTA have failed, and these changes seem unlikely in today’s ideological climate, where child safety often takes a back seat to other concerns. It is probably more realistic to focus on changes to state legislation. A good state disclosure policy, in compliance with CAPTA, should cover fatalities and near fatalities. It should be mandatory and contain no vague terms, conditions, or exceptions. Permitted redactions should be limited to the names of living children in the family and reporters of maltreatment and (temporarily) any information that would cause specific material harm to a criminal investigation. There should be no prohibition on sharing information deemed to be against the best interests of or harmful to the injured child or any other child in the household.
At a minimum, a disclosure policy should require prompt public notification of all fatalities and near fatalities reported to the hotline and accepted for investigation, along with a documented rationale for not investigating others. The notifications should include whether the family had past involvement with CPS and a brief summary of prior reports and responses by the agency. There should be no requirement that the historical information be “pertinent to the abuse or neglect that caused the fatality,” as suggested by the CWPM. Upon completion of the investigation, if it is determined that the fatality resulted from abuse or neglect, the department should be required to release a detailed summary of prior reports involving the family or household and of agency responses, including investigations, in-home cases, child removals, and family reunifications, The agency’s complete files on the perpetrators and their children, with certain identifying information redacted, should be available to any person upon request.
A study of the policies of 50 states and the District of Columbia toward disclosing information regarding child maltreatment fatalities and near fatalities shows that many fall drastically short of embodying Congress’s intent in adding Section 106(b)(2)(B)(x) to CAPTA. Most of these difficulties stem from the deficiencies of the language itself and the guidance provided in HHS’s CWPM. While changing CAPTA’s language would be the most efficient way to enable improvement around the country, it is more likely that legislators and child advocates at the state level will collaborate on legislation requiring full transparency around these deaths. We cannot make progress in preventing severe and life-threatening child maltreatment unless legislators, advocates, and the public can access comprehensive information about what led to these tragic events.
Rhode Island provides notifications of suspected maltreatment only for fatalities and near fatalities only if the child was the subject of an open case; other notifications occur only after maltreatment is confirmed. ↩︎
This essay was originally published on the website of Lives Cut Short, a project to document child maltreatment deaths in the United States since 2022, for which I serve as Senior Project Associate
Jahmeik Modlin was found in a skeletal condition in a Harlem apartment stocked with food. He died the next day, and his three older siblings were hospitalized with severe malnutrition. The family had been on the radar of the Administration for Children’s Services (ACS) since 2019, before Jahmeik was born. But the agency closed its last case with the family in 2022 after determining that the children were safe, a source told the New York Times. A spokeswoman for ACS declined to offer further information, citing state law designed to protect siblings of fatal abuse victims.
According to data states submit to the federal government, about 1800 children die of abuse and neglect every year, but this figure is widely recognized to be an undercount. Among those deaths, studies suggest that between a third and a half involve families who were already known to the child protection system (CPS) through previous reports. Even in other cases where the family had no prior contact with CPS, other systems may have interacted with the child and perhaps could have intervened. Legislators, advocates and the public must have access to timely information about the circumstances leading up to child maltreatment fatalities so they can identify missed opportunities and policy and practice changes necessary to protect children. For that reason, Congress in 1996 added a provision in federal law that requires all states to provide assurances to the federal Department of Health and Human Services that they have provisions for disclosing findings and information regarding child fatalities and near fatalities from maltreatment.
Lives Cut Short surveyed state laws and policies governing access to information about child maltreatment fatalities and near fatalities. The resulting report, Keeping the Public in the Dark: How Federal and State Laws and Policies Prevent Meaningful Disclosure about Child Maltreatment Fatalities and Near Fatalities, shows that most states have such laws and practices but many of them are vague, and many have provisions that conflict with the purpose of ensuring public access to critical information. Among such provisions are those that prohibit releasing information that might harm surviving children in the families where a child was killed or seriously injured by maltreatment.
New York, at first glance, appears to be more transparent than most states in making information and findings about child maltreatment fatalities available to the public. The New York State Office of Children and Family Services (OCFS), which supervises local agencies such as ACS, is required to review all local investigations of child fatalities reported to the State Central Register and to publish a summary report within six months of the investigation. Disclosure of this information, however, occurs only if the state or local commissioner determines that it is not “contrary to the best interests of the child, the child’s siblings or other children in the household.” While the law does not provide a comprehensive definition of “contrary to the best interests,” the OCFS website does explain that OCFS conducts what it calls a “best interests determination,” sometimes assisted by “experts” from the agency’s Statewide Child Fatality Review Team. The process considers “whether publishing a fatality report is contrary to the best interests of a child’s siblings or other children in the household, what effects publication may have on the privacy of children and family, and any potentially detrimental effects publication may have on reuniting and providing services to a family.”
To understand the impact of the “best interests” determination, one needs to know the proportion of child fatalities for which New York withholds reports. The identifying numbers that the state assigns to its child fatality reports provide a useful clue. All these numbers start with a two-letter abbreviation for the region (AL for Albany, BU for Buffalo, etc.), continue with the last two digits of the year, and end with a three-digit number, starting from 001. For example, the first Albany report for 2022 would be identified as AL-22-001. Assuming that all missing numbers represent reports withheld under the “best interests determination,” about one-quarter of reports on 2022 fatalities in New York State were withheld.
The Child Abuse and Neglect Deaths Integrated Database (CANDID), maintained by Lives Cut Short, allows us to determine which child deaths reported in the media had a corresponding fatality report released by New York OCFS. CANDID combines information on child maltreatment fatalities from media reports, official fatality reviews or reports, and other available sources. New York State’s fatality reports do not include names, but they do include the dates of death as well as details about the circumstances. Therefore, one can attempt to match media coverage with the OCFS review of the same fatality. But very few maltreatment deaths occurring in 2022 and covered by the media had an OCFS review released to the public. It appears that the reviews of high-profile deaths that received media coverage were withheld based on “best interest determinations.”
These cases included:
The death of Bryleigh Klino, a profoundly disabled 17-year-old whose parents have been charged with endangering her welfare. Hospital employees observed numerous signs of abuse and neglect on Bryleigh’s body;
The drowning of six-month-old Dalilah Crespo, whose death was ruled a homicide;
The death from abusive head trauma of four-month-old Cairo Dixon-Sanchez, for which his father pleaded guilty;
The fentanyl poisoning death of 11-month-old Liam Sauve, who ingested 23 times the amount of fentanyl that could kill an adult and whose mother pleaded guilty for his death;
The death of three-month old Genevieve Comager, whose father was charged with shaking her to death;
The beating death of nine-year-old Shalom Guifarro, whose mother has been sentenced to 16 years for her killing;
The death of two-year-old Ermias Taylor-Santiago of a fentanyl overdose, which was ruled a homicide;
The death of blunt force trauma of Xavier Johnson, whose mother’s boyfriend was charged with beating him to death;
The fatal heroin overdose death of six-month-old Denny Robinson, found with a heroin bag in his mouth in a house that was connected with a major drug trafficking operation;
The drug and alcohol poisoning of 14-year-old Hailey Hasbrouck, allegedly by her father and his girlfriend, who allegedly gave her the “toxic cocktail;”
The “suspicious” death of seven-year-old Hunter DeGroat, found unresponsive in his home;
The death of two-year-old Aniyah Wyatt-Wright, allegedly punched to death by her father;
The murder of three-year-old Shaquan Butler, beaten to death in a Queens homeless shelter after being reunified with his parents after being removed from them by ACS.
It is probably not a coincidence that OCFS has elected not to release information on most of the egregious fatalities that were covered in the media. Many of the published state fatality reviews concern deaths due to unsafe sleep factors, accidental drownings, and other fatalities that do not result in criminal charges and are therefore never known to the public. It is possible that OCFS is trying to shield the surviving children in the cases listed above because readers may be able to identify them by putting together the reports and the media coverage—as we did. But these are the very cases for which the information is most urgently needed. The nature of these cases suggests the existence of serious and chronic conditions that might have resulted in previous reports and involvement with CPS. Any harm that public release of the report would cause when the incident has already been covered in the media is dubious. It’s hard to avoid wondering if the exclusion of these cases from disclosure protects the agency more than the children. And to avoid guessing that Jahmeik’s death will join the list of those cases for which reports are never published.
We cannot make progress in the prevention of severe and life-threatening child maltreatment unless legislators, advocates and the public have access to comprehensive information about what led up to these tragic events. Congress tried to provide this access through a provision in federal legislation, but states have couched this requirement in vague language or hedged it with qualifications that prevent the release of critical information—or any information at all in some cases—as in New York. Only Congress can fix the gaps in the federal law, but state legislatures can act in the meantime to ensure their disclosure laws serve the purpose of improving child welfare in their states.
The annual Child Maltreatment reports, produced by the Children’s Bureau of the U.S. Administration for Children and Families, are based on data that states submit to the National Child Abuse and Neglect (NCANDS) data system. These reports are eagerly anticipated in the child welfare policy community because they provide much of the data commonly used to quantify child maltreatment and the operations of child protective services around the country. The latest report, Child Maltreatment 2022 (CM2022), provides data for Federal Fiscal Year (FFY) 2022, which ended on September 30, 2022. This post discusses the findings on child maltreatment fatalities specifically. A more general discussion of the report is provided in a previous post. In general, this analysis shows the extent to which child maltreatment fatality numbers and rates reported by states reflect how they define and determine child maltreatment fatalities. This diversity makes it impossible to use these data to estimate the total number of fatalities, differences between state maltreatment fatality rates, and differences over time. More specifically, several key points emerge from the analysis.
States reported a total of approximately 1,990 fatalities to the federal government for Federal Fiscal Year 2022. Yet it is widely recognized that states’ reports to the federal government greatly underestimate the number of child fatalities due to maltreatment by most common definitions. States may use restrictive definitions, fail to consult all available sources, or decide not to investigate or substantiate some maltreatment related deaths. Information from the states’ commentaries to Child Maltreatment 2022 reveals great diversity in how they determine child maltreatment fatalities. In states where child death review (CDR) teams estimate the number of maltreatment deaths, their estimates are always higher than the NCANDS estimates, with some CDR estimates as much as twice, three times, or even ten times higher.
CM2022 shows child fatalities increasing every year between FFY 2018 and FFY2022. But year-to-year changes should be approached with caution. Most states report for each fiscal year the number of maltreatment fatalities identified during that year, not the number that occurred during that year. However, at least two states, including the state with the largest number of children (California), report fatalities based on the year of occurrence and report additional deaths in subsequent years as they are identified. For this reason, even five-year trends shown in CM2022 may change over time. Adjusting for the changes in reports for these two states, reported child maltreatment fatalities have indeed been increasing since 2013. Several states report improvements over time in their ability to capture child maltreatment fatalities for NCANDS reporting. Thus, we do not know the extent to which this increase reflects improved reporting as opposed to increasing deaths from abuse or neglect.
The data reported in CM2022 show that child maltreatment fatalities are concentrated in the youngest children and become less frequent as age increases. Boys are somewhat more likely to die of maltreatment than girls. Black children are much more likely to die of maltreatment than White or Hispanic children—two to three times as likely as White children, depending on the year. The broad category of “neglect,” defined as defined as “neglect or deprivation of necessities” was involved in 76 percent of child maltreatment fatalities while abuse was Involved in 42 percent. Another 8.3 percent of child maltreatment fatalities involved medical neglect.
The Number of Child Fatalities
There is no standard mandated reporting system for child abuse or neglect deaths in this country. Definitions, investigative procedures, and reporting requirements vary from state to state. Attributing a child’s death to abuse rather than to an accident or natural cause is often extremely difficult. The death of a toddler who drowns in a bathtub, for example, may be classified as an accident in one jurisdiction or as a child neglect death in another.
Child Maltreatment 2022 (CM2022) reports an estimated total of 1,990 child maltreatment fatalities for FFY2022.1 But there is widespread agreement among experts that the annual estimates of child fatalities from NCANDS undercount the true number of deaths that are due to child maltreatment by a factor of two to three.2 The National Center on Child Fatality Review and Prevention lists several reasons why this occurs in a given jurisdiction. Jurisdictions may count only deaths substantiated as abuse or neglect using definitions from child welfare civil or criminal law, which may not be comprehensive. Some jurisdictions count only deaths for which the death certificate lists homicide or child maltreatment. Multiple data sources may not be used to identify possible maltreatment deaths. Accidental deaths that were made possible by egregious neglect are often not included,
To get states to use more data sources, the Child and Family Services Improvement and Innovation Act (P.L. 112-34) requires states to describe in their state plans all the sources used to compile information on child maltreatment deaths. To the extent that information from state vital statistics departments, child death review teams, law enforcement agencies and medical examiners or coroners is not included, states must explain the reason for the exclusion and how they plan to include this information in the future. However, this law is clearly not being enforced, and most states do not report using data from all these sources.
In the commentaries that almost all states provided with their NCANDS submissions (included at the end of CM2022), most report drawing on at least some sources external to the child welfare agency, but usually this information is accepted only as a report to the child protection hotline with an allegation of maltreatment. Only if investigated and substantiated by child protective services (CPS) are these deaths included in the counts provided to NCANDS. A few states report taking special measures to ensure that suspected child fatalities are reported to child welfare agencies. In Missouri, coroners and medical examiners are required by law to report all child fatalities to the child abuse hotline. In its commentary, Missouri suggests that it may appear to have a higher child fatality rate than other states because of this law, and indeed its child fatality rate is higher than that of most states. Indiana requires county coroners to report any “suspicious, unexpected, or unexplained” deaths to the Department of Child Services (DCS). Idaho’s Division of Vital Statistics refers to CPS all child death cases for which the cause of death is homicide. (Except when a link or reference Is provided, information in this post is drawn from CM2022.)
Some state child welfare agencies have an internal fatality review unit that may add maltreatment fatalities to the state’s counts. Minnesota’s child welfare agency has a Critical Incident Review Team that reviews death certificates and directs local agencies to add fatalities that they find were due to abuse and neglect to the cases that they already substantiated. New Jersey’s Department of Children and Families’ Office of Quality maintains a critical incident review process that may add to NCANDS some deaths that were not substantiated as maltreatment by CPS.
A few states explain that they report to NCANDS fatalities that are determined to be maltreatment-related by agencies other than child welfare:3
California reports fatalities determined by medical examiners or coroners, and by law enforcement agencies, in addition to county child welfare agencies, to NCANDS.
Washingtonand New Mexico report to NCANDS child fatalities that were determined to be the result of abuse or neglect by a medical examiner that were not already known to CPS.
Alabama, Nebraska, and North Dakota add cases from child fatality review teams that were not already in their databases to their NCANDS reports.
South Carolina incorporates into its NCANDS submission additional cases received from the State Law Enforcement Division (SLED), which receives reports of all child deaths that were not the result of natural causes. SLED investigates all “preventable” cases and refers its findings to the Department of Social Services.
Since most states’ child welfare agencies report only fatalities substantiated as maltreatment by CPS to NCANDS, the number that are reported will depend in part on the state’s definition of a child maltreatment fatality. NCANDS defines a child maltreatment death as “the death of a child as a result of abuse or neglect, because either: (a) an injury resulting from the abuse or neglect was the cause of death; or (b) abuse and/or neglect were contributing factors to the cause of death.”4 But not all states use this definition. At least one state, Arizona, includes only fatalities where abuse or neglect was the sole cause of death, as described in more detail below. (Iowa indicated that it did not include fatalities where child maltreatment was only a contributing factor until FFY2015 and there may be other states that do the same.)
A state’s maltreatment fatality numbers will also depend on its tendency to accept child fatality referrals for investigation and to substantiate them. Hotline screening methods and tools differ by state, and states report little about their screening practices around child maltreatment fatalities. Ohio, which has a county-run system, reports that some county agencies will not investigate child fatality reports if there are no other children in the home or the other children are not deemed to be at risk of maltreatment. The likelihood of substantiation of a report once accepted for investigation will depend on a state’s standard of proof and other investigation policies, messages transmitted by agency leadership, and staffing issues. My commentary about CM 2022 shows how much screening and substantiation rates for maltreatment reports differ by state, and there is no reason to think that fatality reports would be any different from other maltreatment reports. Variations in these rates, as well as the sources states draw from and the definitions they use, ensure that states’ child maltreatment fatality counts reflect much more than the actual number of maltreatment fatalities according to a given definition.
It is instructive to compare states’ maltreatment fatality rates displayed in CM2022 with their rankings on an index of child well-being such as the one used in the Annie E. Casey Foundation’s latest Kids Count Data Book. The 12 states with the highest rates of reported child maltreatment fatalities in CM2022 are Mississippi, South Dakota, Arkansas, Maryland, Alaska, Ohio, Missouri, New Mexico, North Carolina, Illinois, Indiana and South Carolina. Only four of these states are among the 12 states with the lowest rankings for overall child well-being, according to Kids Count. The 12 states with the lowest rankings on child maltreatment fatalities in CM2022 are Vermont, Montana, Nebraska, New Hampshire, Arizona, New Jersey, Rhode Island, Kansas, Kentucky, Utah, Maine, Utah and Hawaii. Five of these states are also among the 12 states with the best child well-being outcomes, and another seven are not. Clearly a state’s rank on child well-being is not an accurate predictor of its rank in reported child maltreatment fatalities. This suggests that the fatality data may reflect more than actual child maltreatment deaths that meet the state’s definition. Particularly striking are the two states—Arizona and Kentucky—that are among those with the lowest reported child maltreatment rates and worst child outcomes. But it is worth noting that there are no states with top-tier child well-being outcomes that have bottom-tier reported child maltreatment fatality rates. Therefore, this exercise suggests that the state fatality rates may reflect in part the “true” incidence of maltreatment fatalities as defined by the states and in part how maltreatment fatalities are identified.
Arizona is one of the states with the lowest reported maltreatment fatality rates despite its low child well-being ranking. Serendipitously, it turns out that Arizona has another estimate of child maltreatment fatalities, thanks to its exceptional Child Maltreatment Fatality Team (CFRT), which is housed in the state’s health department. Arizona’s CFRT analyzes every child death, classifies it by cause and manner, and determines whether the death was caused by abuse or neglect. All child death certificates issued in the state are reviewed, first by the local team in the area where the child lived, and then by the statewide team. For Calendar Year 2022, the team calculated that there were 146 neglect or abuse deaths, or 17 percent of all child fatalities that year. Yet, the Arizona Department of Child Safety (DCS) reported only 14 fatalities to NCANDS for FFY 2022, resulting in its low reported maltreatment fatality rate of 0.88 per 100,000 children.
In its current Child and Family Services Plan, DCS reported that it receives information on all unreported child fatalities from local CFRT’s. But the agency explained that CFRT identifies many more fatalities than it does because CFRT includes deaths where maltreatment was believed to have “contributed” to the death rather than “caused it,” a distinction discussed above, But, as we have seen, the NCANDS Codebook defines a maltreatment death to include cases where abuse and/or neglect were contributing factors to the cause of death.” By not reporting such deaths, DCFS is failing to report all maltreatment fatalities as defined by NCANDS.5
Arizona’s CFRT clearly has an expansive definition of maltreatment fatalities and probably errs on the side of finding maltreatment. Forty-four of the 146 maltreatment deaths it found (30 percent) were due to suffocation—apparently mainly unsafe sleep deaths. Another 15 (10 percent) were due to drowning. Most of these suffocation and drowning deaths were likely accidental. And as the quote at the top of this post indicates, one jurisdiction (or agency within a jurisdiction) may classify such a death as neglect and another may not. Another ten percent of the CFRT-identified maltreatment deaths were due to prematurity caused by the mother’s substance abuse or other factors. Fifteen states (including Arizona) and the District of Columbia defined prenatal exposure to harm due to the mother’s abuse of an illegal drug or other substance as neglect as of May 2022. But DCS may not in practice investigate or substantiate such cases.6
The comparison with CFRT provides some insight on why Arizona reports such a low rate of maltreatment fatalities. Leaving out fatalities where maltreatment was a contributing factor and being less likely to find that accidents or premature births involve maltreatment, may help explain the difference between the two estimates. It is also worth noting that Arizona reported a steep drop in maltreatment fatalities from 48 in FFY 2018 to 33 in FFY2019 to 18 in FFY 2020 (followed by no fatalities reported in FFY2021 and 14 in FFY2022). Arizona provided no explanation for these reductions in its commentaries for FFY’s 2019, 2020, and 2022 and did not provide commentary for FFY2021. One cannot help but wonder whether DCS changed its methods or criteria or simply stopped investigating some allegations of child maltreatment fatalities.
In its publication mentioned above, the National Center for Child Fatality Review and Prevention notes that child death review (CDR) teams often identify more maltreatment deaths than states report to NCANDS. Among the reasons are the records from multiple disciplines and agencies are shared, additional information comes to light in the review process, CDR leads to improved investigations, and teams often use broader definitions for maltreatment, as we have seen for Arizona. CDR teams in most states do not review all child fatalities for a given year or identify those that were due to maltreatment, as Arizona does. But a review of the most recent state CDR reports in all states that published statewide reports yielded eight state CDR teams (including Arizona’s) that do such an analysis. Table 1 shows the differences between the number of maltreatment fatalities identified and reported to NCANDS by child welfare agencies and the number identified by the CDR teams in these eight states in their most recent reports. All the CDR estimates are higher than the NCANDS reports, ranging from 50 percent higher in North Dakota to almost ten times as high in Arizona.
Table 1: Number of Child Maltreatment Fatalities Reported by NCANDS and by CDR
In contrast to Arizona, Mississippi’s position in the ranking of child maltreatment fatalities is not a surprise. Being 48th in child well-being, the state also has the highest child maltreatment fatality rate—by far—at 10.62 per 100,000 children. But there is an anomaly. Mississippi’s maltreatment fatality rate is almost twice that of the state with the next highest rate. And it almost doubled between 2020 and 2022. Even assuming that Mississippi’s “real” maltreatment fatality rate is closer to the 5.48 per 100,000 it reported in FFY2020 still puts it second from the top of all states. It seems unlikely that Mississippi’s child maltreatment deaths doubled in two years; it is more plausible that something about the way the deaths were defined, identified, or reported changed.
This discussion has illustrated the impossibility of knowing the extent to which state maltreatment fatality numbers reflect real differences in child maltreatment fatalities versus differences in definition or measurement. But if states were consistent over time in their definitions and measures, the difference in fatality numbers over time could still be meaningful. Whether that is the case is discussed below.
Have child fatalities increased?
As mentioned above, CM2022 provides a national estimate of 1,990 children who died of abuse or neglect in FFY 2022 at a rate of 2.73 per 100,000 children in the population. Exhibit 4A from CM2022 shows an increase in reported child maltreatment every year between FFY2018 and FFY2022.7
There are many reasons to be cautious about year-to-year comparisons of child fatalities. Those deaths reported in the 2022 report did not mainly occur in 2022. As CM2022 puts it, the “child fatality count in this report reflects the federal fiscal year (FFY) in which the deaths are determined as due to maltreatment,” rather than the year of death.8 It may take more than a year to find out about a fatality, gather the evidence (such as autopsy results and police investigations) to determine whether it was due to maltreatment, and then make the determination. States explain in their commentaries that the deaths they reported may have occurred as long as seven years before 2022. Because child fatalities are rare, a year-to-year increase, even in a larger state, may reflect a large fatality event that occurred in one year or a delay in determining several fatalities. For example, Illinois reported that an increase from 70 fatalities in FFY2018 to 106 in FFY 2019 resulted from the delayed completion of 15 death investigations and an incident that claimed the lives of ten children.
However, not all states report fatalities in the way described by CM2022. California, as it describes in its annual commentaries, reports for each federal fiscal year the deaths that occurred in the prior calendar year and were known to the state by December of the calendar year following the death. Because counties will continue to investigate fatalities that occurred in previous years, the state submits revised counts if additional fatalities from that calendar year are later determined to be caused by abuse or neglect. For example, California originally reported 135 fatalities in FFY2021, but that number had increased to 159 by FFY2022. Second-year changes were not as large for fatalities first reported in FFY2020 and FFY2021.
Knowing that at least one state changes its fatality data in the next year’s submission raises an intriguing question. Even accepting that each state’s fatality count has its own meaning, can we even rely on Exhibit 4A in any given year to at least illustrate the trend in reported fatalities? It does not take long to answer that question. Exhibit 4A of CM2021 does not show maltreatment fatality rates increasing each year between FFY2018 and FFY2022, as does the same table in FFY2022. Instead, it shows a decrease in FFY2020 followed by an increase in FFY2021 to just slightly below the level of FFY2019.
Since each CM report shows five years of data, each year’s figures will eventually be shown in five different reports, starting as the most recent year displayed and ending as the earliest year. Table 2 shows the numbers of fatalities reported for FFY 2018 to FFY2022 in the CM report for each year. The figures for FFY2018 and FFY2019 changed two or three times in the succeeding years, but never by more than 10 deaths. Oddly, the number of deaths reported sometimes decreased from year to year. But the original numbers for FFY2020 and FFY2021 increased considerably in succeeding years. The total number of deaths reported for FFY2020 increased from 1,750 in that year to 1770 in FFY2021 and 1,850 in FFY2022. The total for FFY2021 increased from 1820 in that year to 1930 in FFY2022. Clearly, the 24 fatalities that California added in FFY2022 for the previous year are part of that increase, and presumably one or more other states did the same. Inserting the new numbers into the table from CM 2021 now shows an increase every year between FFY2018 and FFY2021.
Table 2: Deaths Reported by Year Reported
Deaths in:
Reported In:
2018
2019
2020
2021
2022
2018
1770
1780
1770
1765
1765
2019
1840
1830
1825
1825
2020
1750
1770
1850
2021
1820
1930
2022
1990
Source: Author’s compilation from Children’s Bureau child maltreatment reports. US Department of Health and Human Services, Administration for Children and Families, Children’s Bureau, “Child Maltreatment,” June 27, 2023, https://www.acf.hhs.gov/cb/data-research/ child-maltreatment.
A plot of the number of child fatalities reported between FFY2013 and FFY2022, using the most recent versions of each number, is shown below as Figure 1. Assuming the numbers for years before FFY2021 will change little if at all, we can see that reported child maltreatment fatalities have increased annually since FFY2013, aside from a slight decrease in FFY2017. And if the numbers from FFY2021 and FFY2022 will increase, as seems likely, the rise in fatalities in FFY2021 and FFY2022 will get steeper.
Source: Source: Author’s calculations using US Department of Health and Human Services, Administration for Children and Families, Children’s Bureau, “Child Maltreatment,” June 27, 2023, https://www.acf.hhs.gov/cb/data-research/child-maltreatment
The critical question is whether this increase in reported child maltreatment fatalities reflects increasing maltreatment deaths, better measurement, or even changing definitions. Some states attribute increases in reported fatalities to improvements in the accuracy of their reporting.9
Through 2018, North Carolina reported only child fatalities determined by the Chief Medical Examiner as homicide by a parent or caregiver. According to a Senior Media Relations Manager at the North Carolina Department of Health and Human Services, “Since 2018, Child Welfare has: developed closer working relationships with counterparts at OCME, utilized vital statistics data, and enhanced processes to include more law enforcement information. This work has increased our ability to identify maltreatment deaths, as defined in statute…[W]e have also continued to enhance our ability to track the information – resulting in more robust reporting and accounts for the change in numbers.” The Children’s Bureau noted in CM2022 that North Carolina “resubmitted data from multiple prior years to include additional fatalities.” North Carolina’s reported child fatalities increased from 64 in FFY2018 to 111 in FFY2019, 99 in FFY 2020, 121 in FFY2021, and 93 in FFY2022.10
Mississippi reported that the creation of a special investigation unit for child fatalities in FFY 2014 resulted in an increase in reported child maltreatment fatalities in FFY2013, FFY2014, and FFY2015. The state also reported that public awareness campaigns about deaths caused by unsafe sleep and deaths from heat stroke of children left in hot cars led to more reporting of such deaths as possible maltreatment starting in 2014.
West Virginia reported 20 fatalities in FFY 2016 compared to 9 in FFY2015 and attributed the increase to the fact that the state had begun investigating child fatalities in cases where there were no other children in the home.
Virginia attributed its increase from 37 maltreatment fatalities in FFY2014 to 54 in FFY 2015 to a change in the law regarding the timing of investigations. The time spent waiting to obtain documents from outside agencies, like autopsies, would no longer count toward the 45-day deadline for completing an investigation. (It is not clear whether child death investigations previously were terminated before these documents arrived, and therefore the deaths were not reported.)
Ohio reported in FFY2022 that it required mandated reporters participating on child fatality review boards to report suspected maltreatment fatalities to the local child welfare agency. Reported child maltreatment fatalities increased from 98 in FFY2021 to 115 in FFY 2022. But the state also attributed the fatality increase to the fact that the overall death rate from violence had been on the rise for the past several years, showing the difficulty of disentangling causes for any increase in maltreatment fatalities.
Iowa began reporting child fatalities where maltreatment was a contributing factor rather than the sole cause of the fatality in FFY 2015. Reported fatalities increased from 8 to 12 but those are small numbers, and Iowa attributes the increase to the growing under-18 population.
The increase in reported maltreatment fatalities clearly reflects at least in part improved reporting, as documented by some states. But it may also reflect an underlying increase in actual maltreatment fatalities as defined by the states. Such an increase could be due to several factors. Washington’s commentary in the FFY2022 report suggests that the opioid crisis has contributed to its increase in fatalities from 19 in FFY 2021 to 31 in FFY 2022.11 West Virginia also reported an increase in illegal drug use in its commentary to CM2016, probably referring to opioid abuse as well.12 Ohio mentioned increasing violence in recent years as a possible reason for the increase in reported child maltreatment fatalities.
Demographics, type of maltreatment, and perpetrators
We have already discussed the reasons that the child maltreatment fatality numbers may not be accurate, even given different definitions in different states. These problems affect our ability to draw conclusions about demographics and child maltreatment fatalities. If some of the definition and measurement issues affect different groups differently, it is possible that findings on demographics would be less meaningful.
The data presented in CM2022 shows that Infants under a year old are more than three times more likely to die of maltreatment than one-year-olds, and the fatality rate generally decreases with age. Younger children are more fragile, and there are many reasons to believe that the relationship between age and maltreatment fatality rates is correct, despite problems with the data. The age graph has a similar shape every year, with the percentage of child fatalities dropping as age increases.13 The percentage of victims who are under one year old varied between 22.8 percent and 25.3 percent between FFY2018 and FFY2022. There are bigger differences by year in the older age groups, where smaller numbers make the data less reliable.
Boys were between 57 percent and 60 percent of the fatalities in every year between FFY2018 and FFY2022. In contrast, victims of child maltreatment in general, are slightly more likely to be girls. It is hard to imagine a reason why data problems would affect boys and girls differently, so it is likely that boys are more likely than girls to die from maltreatment.
Reported child maltreatment fatality rates varied greatly by race and ethnicity, and the differences among the larger groups were fairly stable over the five years since FFY2018. Black children had by far the highest maltreatment fatality rate of all the groups for whom information was available. The fatality maltreatment rate for Black children ranged from 5.06 to 6.37 per 100,000 children over the five-year period. Reported maltreatment fatality rates ranged from 3.27 to 4.40 for children of two or more races. White children reportedly died from maltreatment at a rate between 1.90 and 2.18 per 100,000 children, Hispanic children at a rate from 1.44 to 1.89. (The numbers of Native American, Native Hawaiian, and Asian children were too small to be reliable). The reported maltreatment fatality rate for Black children was two to three times as high as the rate for White children, which was always somewhat higher than the rate for Hispanic children. The rates from CM2022 are shown in Exhibit 4-D, reproduced below.
The question of bias must be addressed in evaluating racial and ethnic differences in reported child fatality rates. We have seen that fatality numbers reported by states generally reflect the results of a CPS investigation or a determination by a coroner, medical examiner, or fatality review team. It is possible that racial bias could play a role in whether a fatality is substantiated as due to maltreatment. But Drake et al. found that indicators of risk and harm for Black children were usually between two and three times greater than those for White children in 2019, while the Black-White homicide disparity was four times as great as that for White children.14 While we cannot rule out any role for bias, it is unlikely to be the main cause of the Black-White disparities in child maltreatment fatalities. As Drake et al suggest, they are more likely to stem from the legacy of slavery, Jim Crow, and segregation, which includes intergenerational poverty and the relegation of poor Black families to disadvantaged and often dangerous neighborhoods.
For each fatality, NCANDS collects the types of maltreatment that were substantiated. The authors note that “while these maltreatment types likely contributed to the cause of death, NCANDS does not have a field for collecting the official cause of death.” One child can be found to have suffered more than one type of maltreatment. Over three quarters (76.4 percent) of the children who died were found to have suffered from “neglect” (defined as “neglect or deprivation of necessities” in the Codebook), 42.1 percent were found to have endured physical abuse, 8.3 percent were found to have suffered from medical neglect, and 2.4 percent from sexual abuse.
Most of the perpetrators of reported child maltreatment fatalities were parents, according to NCANDS data submitted by 43 states. A total of 81.8 percent of the maltreatment fatalities involved “one or more parents acting alone, together, or with other individuals. That includes mothers alone in 13.2 percent of the death, fathers alone in 14.5 percent, “two parents of known sex” in 23.2 percent of the fatalities, and mothers with nonparents (such as boyfriends) in 10.3 percent of the cases. Another 13.2 percent of the fatalities involved nonparents only, including relatives (4.7 percent), “child daycare providers” (1.3 percent), unmarried partners of the parent (1.1 percent), and “other” (3.4 percent). A final 4.9 percent of the fatalities involved unknown perpetrators only. (See Table 4-4 of CM 2022 for all the categories, numbers and percentages).
CM 2022 was originally published on the Children’s Bureau website early in January 2024 without a press release; it then disappeared from the website for about three weeks. It is hard to avoid speculating about the reasons for its removal and the gap before it was finally replaced. One might wonder if officials were trying to figure out how to spin the five years of increase in reported fatalities. Strangely, the press release, when it did come out, reported the increase in child maltreatment fatalities without raising the possibility that changes in how fatalities were defined and measured could have contributed to this increase, which might have supported their optimistic narrative.
In summary, this analysis shows how difficult it is to make any conclusions based on the child maltreatment fatality data contained in the Children’s Bureau’s annual Child Maltreatment reports. Single-year numbers cannot be fairly compared between states because they reflect different ways of defining child maltreatment fatalities, learning of fatalities that may involve maltreatment, and determining whether maltreatment was a contributing factor. Trends over time are difficult to assess because states often change these definitions and practices, and because new data from previous years may be entered after each year’s report is published. There is evidence that improved reporting has contributed significantly to the increase in reported fatalities. But until the federal government imposes a uniform set of standards for counting child abuse and neglect fatalities as recommended by the Committee to Eliminate Child Abuse and Neglect Fatalities, it will be impossible to get a handle on actual levels and trends.
Notes
This estimate is based on the reports of 51 jurisdictions including the District of Columbia, Puerto Rico, and all states but Massachusetts. The maltreatment fatality rate for the reporting jurisdictions was multiplied by the population of all 50 states, the District of Columbia, and Puerto Rico, to obtain the estimate of 1,990.
US Government Accounting Office (2011). Child Maltreatment: Strengthening National Data on Child Fatalities Could Aid in Prevention. Washington, DC; Schnitzer P, Covington T, Wirtz J, Verhoek-Oftedahl W, Palusci V. (2007). Public Health Surveillance of Fatal Child Maltreatment: Analysis of 3 State Programs. American Journal of Public Health. 97:7; Herman-Giddens ME, Brown G, Verbiest S, et al. (199() Underascertainment of child abuse mortality in the United States. JAMA. 282:463–467; Crume TL, DiGuiseppi C, Byers T, Sirotnak AP, Garrett CJ. (2002). Underascertainment of child maltreatment fatalities by death certificates, 1990–1998. Pediatrics. 110(2 pt 1):18.
In contrast to those states that augment their own data with that of other agencies, Alaska delegates the entire process of determining whether a fatality involves maltreatment to medical examiners or coroners.
CAPTA defines maltreatment in part as “an act or failure to act on the part of a parent or caretaker,” but it does not define “caretaker.” There may be some differences among states on who they define as a caretaker, but these are unlikely to affect many cases and cause big differences between states.
DCS also says that CFRT’s fatality count is higher because it counts fatalities caused by a person other than the parent, caregiver, or custodian (which would not normally be counted). Based on CFRT’s tabulations regarding caregivers, this does not seem to be a large issue. DCS also state that the CFRT counts deaths that occur outside the state’s jurisdiction, such as on an Indian reservations. It is true that CFRT includes any death that occurs in Arizona, even if the child is not a state resident. However out-of-state residents were only three percent of the total number of fatalities in 2022, according to its most recent report, Ten percent of the children who died of all causes were American Indians but they do not report on how many lived on reservations.
The remaining deaths that CFRT identified were due to motor vehicle and other transport (14), poisoning (13), other medical causes (12), blunt force injury (10), undetermined (9) causes, firearm injury (8), and other injury (6). Many of these deaths could also be due to accidents that DCS was reluctant to investigate or find neglectful.
Exhibit 4A counts the District of Columbia and Puerto Rico as states, resulting in up to 52 “reporting states” per year.
Child Maltreatment 2022, p. 52.
Other states report improvements in their data collection, but their data do not suggest that they had a long-term beyond one year on fatality numbers. In FFY 2020, New York reported that it began reporting all fatalities, regardless of date of death, as long as the investigation ended during the reporting period and the fatality had not been reported during a prior year. Before that time, New York reported only those deaths that occurred and were reported in the applicable FFY. New York attributed the increase in the number of fatalities from 69 in FFY 2019 to 105 in FFY 2020 to this change. Perhaps the increase came from reporting an extra “batch” of fatalities in FFY2020. However, the state had reported 118 fatalities in 2018. And it then reported 126 in FFY2021 and 105 in FFY2022, so it is hard to understand how the change resulted in an increase in fatalities reported, except as compared to a year with abnormally few of them. When fatalities rose sharply in Mississippi from 49 in FFY2021 to 72 in FFY2022; the state again used the creation of the special unit in FFY 2014 to explain the increase, but that seems unlikely. I have asked West Virginia to speculate about reasons for the increase but have not yet heard from the state. In FYF2019 or perhaps FFY2018 (when the state did not submit commentary), South Carolina created a special unit to receive and investigate reports of child fatalities. The number of fatalities reported jumped from 39 in FFY2018 to 60 in FFY2019. But it then fell to 36 in FFY 2020, 41 in FFY2021, and 38 in FFY2022. So it is does not appear that the creation of the special unit had a long term effect on maltreatment fatality counts.
North Carolina provided revised numbers for FFY2018 and FFY2019 to NCANDS and provided them to me through their press office
Washington reports that between FFY 2021 and FFY 2022 the percentage of child fatalities in the state that were due to opioid ingestion or overdose rose from less than one percent to 23 percent of child fatalities. Of the deaths and near-fatalities that qualified for a review because they occurred in families touched by the system in the previous year, that percentage jumped from 28 to 44 percent.
In its Commentary, West Virginia stated that only one of the 13 fatalities reviewed by its critical incident team did not involve substance abuse as a factor either in the death or the family’s history.
However, it must be reported Exhibit 4-B, Child Fatalities by Age, appears to be inaccurate. It looks very different from every other year, with much higher rates for older children. There is no way that the fatality rate per 100,000 17 year olds would increase from 0.42 to 3.3, from 0.57 to 5.0, for example. It looks almost, but not exactly, like Exhibit 3-D, which shows child maltreatment victims (not deaths) by age. The Children’s Bureau referred my inquiry of March 21 to the “appropriate team,” which has not yet responded.
Brett Drake et al., “Racial/Ethnic Differences in Child Protective Services Reporting, Substantiation, and Placement, With Comparison to Non-CPS Risks and Outcomes: 2005-2019. Child Maltreatment 2023, Vol 0(0) 1-17.
ABC News: Joanna, Terri and Sierra Denton-Carrillo
On May 2, 2024, an extraordinary gathering was held in Washington, DC. It brought together scholars, advocates, and family members of children who lost their lives to abuse and neglect to mark the inauguration of a new project, Lives Cut Short. This project, under the auspices of the American Enterprise Institute and University of North Carolina Chapel Hill, will shed a light on the lives and deaths of abused and neglected children, many of which would never otherwise be known to the public. I am proud to be a part of this project, along with Naomi Schaefer-Riley AEI’s point person on child welfare, and eminent child welfare scholars, Emily Putnam-Hornstein of UNC-Chapel Hill and Sarah Font of Penn State. If you missed the event, you can watch it here.
We are grateful that family members of two children who died of abuse were able to join us for our launch. One of these special guests was the aunt of Joanna (age three), Terry (age two) and Sierra (age six months) Denton-Carrillo, who were drowned by their mother despite desperate efforts by their father to warn the Los Angeles Department of Child and Family Services (DCFS) and LAPD about her deteriorating mental state. Also in attendance was the aunt of Sophia Mason, who was physically and sexually abused and forced to live in a metal shed by her mother and mother’s boyfriend in the months before she died. Alameda County (California) DCFS social workers ignored repeated warnings from school staff and medical professionals and family members about Sophia’s injuries and the danger she was in.
About 1,900 children died of maltreatment in the United States in 2022, according to national statistics that are known to be greatly underestimated. All of these children of them were likely known to a family member who could have reported or intervened. At one time, the fact that a large number of children died of abuse or neglect was a big national issue. A national coalition worked to mobilize support for the funding of the Protect Our Kids Act of 2012, which authorized the Commission to Eliminate Child Abuse and Neglect Fatalities (CECANF) and charged it with developing a national strategy to reduce fatalities from child abuse and neglect. CECANF began work in 2014, holding public hearings around the country. In March 2016, after two years of work, it published Within Our Reach: A National Strategy to Eliminate Child Abuse and Negect Fatalities, a 167-page report with 110 recommendations. Eight years later, the report is forgotten, the recommendations disregarded, and mentioning the issue is considered gauche in ruling circles. An office founded to monitor the progress of this state and local efforts to monitor the CECANF recommendations produced a “First Progress Report” and appears to have been disbanded.
Child welfare leaders, legislators and advocates appear to have lost interest in child maltreatment fatalities. As Naomi Schaefer Riley put it at the project launch, she often hears that talking about child maltreatment deaths is “letting the tail wag the dog.” We can’t make policy based on rare events and small numbers, she is often told. Yet, as she stated, these numbers are not small at all. They far surpass the number of people killed in mass shootings, that get a lot more attention. Perhaps more importantly, if child maltreatment is an iceberg, the fatalities represent the part we cannot see. How many more children are suffering in silence?
The Lives Cut Short project has multiple goals. We seek to draw attention to this issue, knowing that public attention is necessary to build up support for reform. We hope to provide a context for media outlets, who often cover an incident in their area without any knowledge of the context. We will draw attention how differently states are defining, identifying, and reporting child maltreatment fatalities, and how this results in a final tally that is like adding apples to oranges, grapes and other fruit, but in any case is underestimated. Already posted on our website is a report that illustrates this diversity in great detail, showing how the numbers that states report to the federal government reflect their definitions and reporting practices as much or more than they reflect the actual rates of child maltreatment. Entitled A Jumble of Standards: How State and Federal Authorities Have Underestimated Child Maltreatment Fatalities, the report may be the only available resource that describes this diversity in state reporting in such detail. And as several speakers explained on May 2, this diversity creates a paradoxical situation in which states that are more transparent and conscientious about reporting child fatalities end up looking like they have higher fatality rates.
The core of Lives Cut Short is a database called CANDID, which consists of records of children who died of abuse or neglect since 2022 whose deaths that fit the federal definition of maltreatment fatalities–those that are caused by maltreatment or for which maltreatment was a contributing factor. All of the data come from publicly available sources, including media reports and official case summaries or reports from states. Right now, the website enables the user to sort the children by state and age. Clicking on each child’s name will allow the reader to access media and non-media sources of information about the circumstances under which the child died. A detailed state-by-state page provides links to each state’s statute governing disclosure of child fatality information as well as links to any child fatality notifications, case summaries, and case reviews, that each state provides.
We will continue both to add child fatalities and to broaden the information on each death. As our searches yield new media reports and state notifications and reviews, which often appear as much as two years after a child’s death, we will add them to our census of child deaths. We plan to seek out other sources, such as Medical Examiner reports, to learn about cases of which we are still unaware. To broaden the information on each case, we have already begun to enter detailed data about these deaths in a detailed database that will record demographic characteristics of the children and families, causes of death, perpetrator characteristics and risk factors, past involvement with CPS and other services, and systemic factors that may have prevented the discover of these children’s plight before it was too late. By bringing together media reports, official case summaries, and other sources such as wrongful death suits, we will be able to provide a richer description than any one source can provide. This information can then be analyzed to provide valuable information to help prevent such fatalities in the future.
We hope that Lives Cut Short will restart the conversation about how to prevent child maltreatment fatalities, and more broadly, redirect the conversation about how to prevent child maltreatment fatalities, which must start with an honest consideration of what serious child abuse or neglect means. Even more broadly, perhaps it will even change the conversation around child welfare services, bringing child safety and well-being back into focus, but also bringing in other systems and their responsibility to vulnerable children. These goals may be ambitious, but we cannot afford to fail.