In a post dated January 10, 2025, I reported that 40 percent of investigations conducted by the District of Columbia’s Child and Family Services Agency (CFSA) in Fiscal Year(FY) 2024, which ended on September 30 2024, were “incomplete.” But by annual rather than quarterly data, that post actually understated the magnitude of the problem, which has worsened in the first half of FY 2025. The percentage of investigations that were terminated with a finding of “incomplete” increased to 65 percent in the second quarter of FY2025. The number of substantiated investigations has increased, while foster care placements and in-home case openings have not kept up with the apparent need for services.
The number of reports to child abuse hotlines varies by season, with reports tending to drop off during the summer when schools are closed and then increase again when schools re-open, along with fluctuations during the school year. Thus, data for part of a year should be compared to the same period of the preceding year. As shown in the table below, the number of reports to the CFSA hotline increased by from 11,945 in the first half of FY 2024 to 12,342 in the first half of FY 2025. The number of reports accepted for investigation actually decreased from 2,197 to 1,973, mostly because the hotline was screening out more of them. Nevertheless, the number of investigations conducted increased from 1,774 to 2,089. Thus, there were more reports, fewer reports accepted, and more reports investigated in the first half of FY 2025 than in the same period of the previous year. The reasons for these changes are unknown.
Table 1: Data for First Half of 2025 Compared to First Half of 2024
An investigation can have several findings. “Substantiated” means that the investigator (with approval from their supervisor) has concluded that the allegation of maltreatment (or risk of maltreatment) is supported by the evidence. “Unfounded” means there is insufficient evidence to support the allegations. “Inconclusive” means there is some evidence that maltreatment occurred but not enough evidence to support it definitively. “Incomplete” is defined as “an investigation finding for referrals in which there were barriers to being able to complete every aspect of the investigation. This could include obtaining confirmation during the investigation that the family was a resident of another state outside D.C., the parent refusing the social worker access to the home to complete a home assessment, or inability to locate the family.” (For the complete definitions, see the Investigations Page on the CFSA Dashboard). It is important to note that “Incomplete” refers to a finding upon closure of an investigation. It is not refer to an investigation that is ongoing.
The total number of investigations increased from 11,945 in the first half of FY 2024 to 12,342 in the first half of Fiscal Year 2025, as Table 1 shows. And there were some big changes in the numbers of investigations that were incomplete, substantiated and inconclusive. The number of incomplete investigations skyrocketed from 456 to 1,305. The number of unfounded investigations dropped from 949 to 327. And the number of substantiated investigations increased from 267 to 377, which is a large increase of 41 percent. This reflects both an increased number of investigations conducted and an increase in the percentage substantiated from 15 percent to 18 percent.
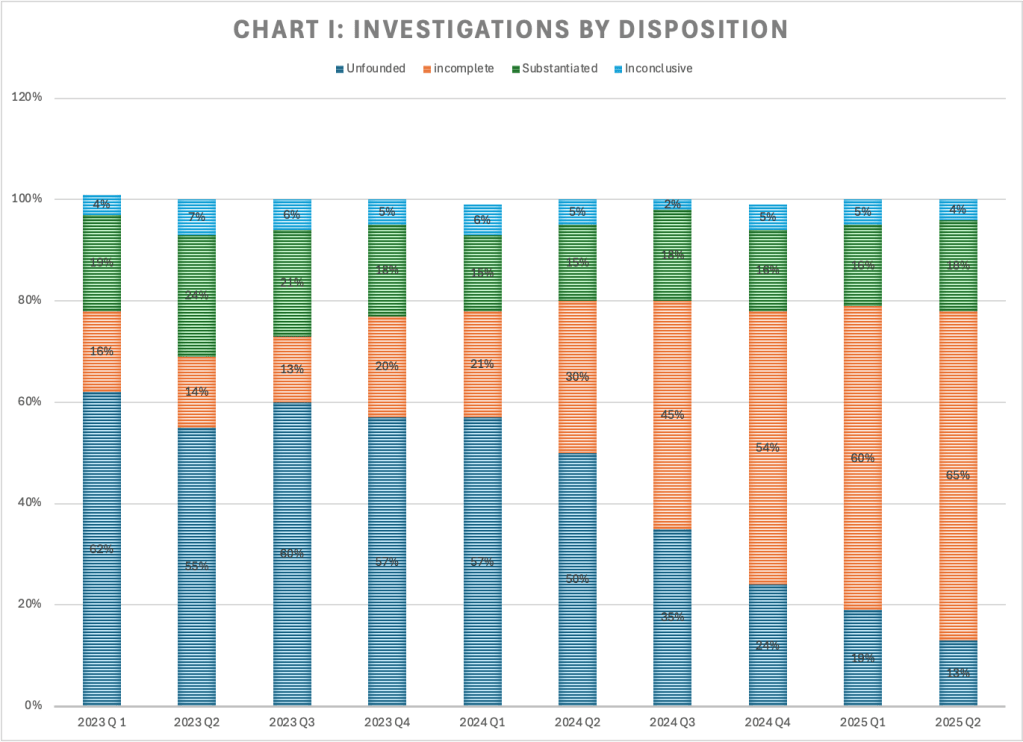
Chart I shows how the percentage of investigations by disposition has changed over the past nine quarters. The percentage of investigations that was incomplete (see the orange segments in the chart below) began to rise in the first quarter of 2024, when it jumped to 20 percent from 13 percent in the previous quarter. It rose to 30 percent in the third quarter of 2024, 45 percent in the third quarter, and 54 percent in the fourth quarter, 60 percent in the first quarter of 2025, and 65 percent in the second quarter of the current fiscal year.
As the percentage of investigations that are incomplete has increased, the percentage that are unfounded (dark blue in the above chart) has decreased–from 57 percent in the first quarter of 2024 to 13 percent in the first quarter of 2025. That drop of 44 percentage points happened at the same time as the percentage of investigations that were incomplete rose from 21 percent to 65 percent–an increase of 43 percentage points. It appears that investigations that would formerly have been closed as unfounded are now being closed as incomplete. CFSA did not respond to a request for the reasons for this change. The percentage of investigations that are substantiated has changed little since the first quarter of FY 2024.
Once an investigation is substantiated, CFSA may open a case for in-home services, or less often for foster care. As shown in Table I above, 169 in-home cases (each involving one or more children) were opened in the first half of FY 2025, compared to 125 in the first half of FY 2024. And 96 children were placed in foster care in the first half of FY 2025 compared with 110 in the first quarter of FY 2024. Unfortunately these two sets of numbers are not comparable as each in-home case can involve more than one child. But with substantiated reports increasing by over 100, in-home cases increasing by only 44, and foster care removals decreasing, it appears that some of the families with substantiated reports in 2025 are not receiving any CFSA services at all, and that is concerning. Perhaps some of these families are being referred to the collaboratives for services, which are less intensive and delivered by staff with lower credentials. And it is possible that some of these investigations may culminate in an informal kinship placement, but that means no services are provided to the parents or the children.
Clearly the staffing crisis with which CFSA (along with other agencies around the country) is struggling is responsible for the increase in incomplete investigations, and perhaps for the reduced percentage of substantiated cases receiving services as well. At the oversight hearing on February 13, 2025, Interim Director Trice pointed out that the number of investigative social workers has dropped from 100 to below 40. It is no surprise that CFSA’s oversight responses documented that most investigative workers had caseloads above 15. the maximum caseload allowed by CFSA’s Four Pillars Performance Framework. Average caseloads for the 38 investigative workers in the first quarter of FY 2025 were 30 or higher for 10 workers and 20 or higher for a total of 20 workers.
Director Trice reported that the agency is making do by diverting workers from the In-Home units to Investigations, but that is not a good solution. Families with in-home cases are often deeply troubled, with long histories of chronic neglect. According to CFSA’s 2023 Child Fatality Report, two children died while their families had open in-home cases. We cannot afford to divert these critically needed workers. Moreover, it is possible that the diversion of in-home workers to investigations may be part of the reason that in-home case openings did not increase more given the increase in substantiations. With workers not available to handle these cases, the agency may be more reluctant to open them.
What can be done? Creative solutions are needed. It may be necessary to temporarily reduce licensing or degree requirements through a special waiver due to the staffing crisis. Former Director Robert Matthews spoke of obtaining permission from the Board of Social Work Examiners to use workers with Bachelor of Social Work degrees to help investigators (not carry cases), but this plan was not mentioned in this year’s oversight responses. The agency might consider recruiting federal workers who have lost their jobs for these positions. Recruiting retired police officers and military veterans is another idea that has potential. A partnership with local schools of social work, as Maryland and other states maintain, is long past due. Those who agree to take jobs and remain for a given amount of time should receive loan forgiveness and perhaps housing as well. In a housing-hungry citizen, this could be a game changer. CFSA needs to think outside the box to resolve the staffing crisis.
CFSA’s Dashboard data for the first half of FY 2025 raises more questions than it provides answers. The most striking trend is the continuing explosion in the percentage of investigations that were incomplete–which was 65 percent in the second quarter. Also concerning is the failure of in-home case openings and foster care placements to keep up with increased substantiations. Like many other child welfare agencies, CFSA has been devoting much time and attention to programs outside of its core functions, like the warmline and family success centers. In this time of budget stringency and looming recession, it is time for CFSA to focus on its ability to perform its most basic and important function–child protection.
Recognizing implicit bias in mandated reporting training is a national focus for addressing racial inequity in child welfare. States from New York to Washington have updated their training for mandatory reporters to include implicit bias or highlight the distinction between neglect and poverty in an effort to reduce racial disparities in child welfare involvement. My recent experience taking the updated training in Washington DC made clear that there is a fundamental conflict between preparing mandated reporters for their responsibility to report and advising them to assess their biases before reporting. The basic conflict is this: the core training instructs mandatory reporters to report any suspicion of abuse or neglect, while the implicit bias unit urges mandatory reporters to doubt their instincts and reconsider their duty to report.
In FY 2023, the District of Columbia’s Child and Family Services Agency (CFSA) updated its online mandated reporter training to include a module focused on understanding and addressing implicit bias for mandated reporters. This training is required for all mandated reporters, who include both professionals (doctors, nurses, teachers, social workers, etc.) and volunteers who work with children. I had taken the training several times in the past–first for my work as a social worker with CFSA and later as a mentor to a foster youth. I had my first experience with the updated training last month as part of my preparation to serve as a Court Appointed Special Advocate (CASA) for a child in foster care.
The Implicit Bias Module
The implicit bias module appears to have been shoehorned into the existing DC mandatory reporter training right after a brief introduction to mandatory reporters and their role. The video introducing the section explains that implicit bias harms “families of color” in the child welfare system, without providing any evidence of such harm. It goes on to assert that “the point of this portion of the training is to make sure that reporting is based on observations and not assumptions. Ultimately we want mandated reporters to consider this before responding to a child’s disclosure of suspected abuse or neglect: Do I have any implicit bias in my decision to call or not to call the hotline.” It may sound reasonable, but as the training unfolds, a conflict with the goals of the overall training and mandatory reporting itself becomes clear.
The implicit bias module continues by explaining that nationally and in DC, mandated reporters call the CFSA hotline about Black families disproportionately more than White families; this leads to more “Black and Brown” children having in-home cases or entering foster care because they are assessed more closely. A graph has been provided, with text saying “In this graph, disproportionality is where you see that Black and Brown children make up approximately 64% of hotline calls. However, only 57% of people in the District are a race/ethnicity other than white.” Unfortunately, one does not see this in the graph, which does not include hotline calls at all! It does include children who are the subject of an investigation after a call to the CFSA hotline, and it shows that Black children made up 57 percent of the investigated children, while comprising 53 percent of the population. That is a very small disparity, and in any case could reflect unequal rates of abuse and neglect between Black and White children. The data does show a larger Black-White disparity in confirmed maltreatment (71 percent of the children confirmed as maltreated are Black) and “foster care” (whether this is children in care or entries into care is unclear) at 92 percent. But these increasing disparities come in at the investigation stage (where the substantiation and foster care decisions are made), not at the reporting stage, calling into question the need for training mandatory reporters about implicit bias. To make matters worse, the data on investigations contain a whopping 40 percent without race or ethnicity data; 26 percent of the confirmed maltreatment data, and 23 percent of the in-home case data also lack race and ethnicity information. (Note that the bars of the graph have been shifted by one column to the left of the corresponding columns from the numerical table, as in the original.) So it is impossible to draw meaningful conclusions from these data.
Source: DC Mandated Reporter Training, Lesson 3, page 6, available from
Other than the mention of the hotline call data, which is missing from the graph, the only analysis of the data in the text reads as follows. “Disparity occurs when these children and families have cases open to either in home or foster care support. As you can see that [sic] 85% of in-home cases, and more than 92% of foster care cases in 2020 were opened with Black and brown families, while again the District’s make-up is only 57% Black and brown.” The inclusion of “brown families” is somewhat disingenuous. The graph shows that Hispanics and Asians, the only “brown” children with non-zero populations on the graph, are underrepresented in investigations, confirmed maltreatment, foster care, etc.1 Switching categories, the lecturer goes on to state that “At every stage, Black and Indigenous families face racial discrimination and unequal treatment.” DC is not known to have a large indigenous population; there is no row on the table for Native Americans, and Native Hawaiians and Pacific Islanders are zero percent of every category except that they are listed as making up two percent of children aging out of foster care in 2019.
A central motif of the training is that the confusion of poverty with neglect contributes to the racial and ethnic disparities in child welfare. The video states that “under current law, most children in the US are separated for neglect, a code word that typically represents conditions of poverty, resulting in disproportionate separation and harm to Black families….” But there is a problem with this. We know that neglect is often associated with serious drug abuse and/or mental illness. After all, most poor people don’t neglect their children. Moreover DC Code Section 16.2301 forbids a court to find maltreatment when the deprivation of food, clothing, shelter or medical care is due to the parent’s lack of financial means. The law does not allow removing children because of poverty in DC, and the small number of removals compared to investigations in DC (224 children placed in foster care compared to 3,767 investigations in FY 2024) suggests that CFSA does not remove children for poverty alone.
The training includes practice scenarios to help trainees distinguish between poverty (or “need” according to the training) and neglect. The participant must read the scenarios and decide whether they represent need (and presumably do not call for a hotline report) or neglect. After providing their own answer, trainees learn the “right answer” according to CFSA. One of the three “need” scenarios is particularly troubling and is reproduced here:
The 4-year-old child came into the center smelling of a strong smell and her nails are long and dirty. There is sticky stuff on her chest that is black underneath her shirt on her skin. The child often comes to the center unbathed. She was wearing shoes that were too small, but the dad was made aware, and he got her new shoes. The child comes in with an old pamper not changed, soaked or soiled. Sometimes she comes to school with the same clothes on from the day before or sometimes wears the same clothes for three days.
The child does not talk or engage with staff or peers. The mother has been observed yelling at the child and all she does is cry. The child covers her eyes but does not ask for anything.
The caller is aware that the family was recently evicted after the mother lost her full-time job and they are being supported on the income made from the father’s part-time employment. The family moves from the homes of family and friends because they refuse to go to a shelter. Caller suspects sometimes the family may sleep in the car.
The characterization of this scenario as “need” rather than neglect is troubling. The combination of factors that are cited suggest something more than poverty. The fact that the child “does not talk or engage with staff and peers,” and that the mother “has been observed yelling at the child and all she does is cry” suggest problems this beyond the realm of need. The refusal to go to a shelter under current conditions, when the District of Columbia guarantees shelter to families with children and has replaced its dilapidated shelter with modern new facilities, increases the likelihood that this is a case of neglect.
In the content that follows, a video tells mandatory reporters that although they are required by law to report suspected abuse or neglect, they should not make reports “solely based on assumptions, schemas, or biases.” It seems rather disrespectful to think that a doctor, nurse, teacher, social worker or volunteer would do this. Trainees are presented with the following questions to ask before making a report.
This is confusing indeed. Is the agency saying that mandatory reporters should not make a report “solely out of legal obligation,” even though they are legally required to report and could receive consequences for not doing so? Providing resources to assist the family is fine, but if there is abuse or neglect, does that exempt the reporter from the duty to report? It seems unlikely and unwise.
“Granted,” the presenter continues, “there are many times when you recognize your legal obligation, have the resources to support a family, and have checked your biases, and a report still needs to be made.” But the speaker goes on to state that “Each of us holds a responsibility to address disproportionality and disparity in the lives of Black and Brown families in the District.” She then invites us to “walk through how we can do this together,” by listening to two videos that are a total of five minutes in length. The first video, on “Mitigating Bias” counsels reporters to follow a three-step process consisting of of “deliberate,” “reflect,” and “educate,” with each step containing mutiple steps or suggestions. Mandatory reporters then learn about “cultural humility” and its three attributes: “lifelong learning and critical self-reflection,” “recognition and challenging of power imbalances,” and “institutional accountability.” And then training participants are told that “[u]ltimately, our goal is to ensure that children who are experiencing neglect in the District receive the support they need to thrive within their families. To do this effectively, we each have to ensure our implicit biases, whether personal or institutional, are not the foundation for calls to the CFSA hotline.” Apparently, no children in the District need to be removed from their families in order to thrive; even though the agency providing the training removed 244 children in the last Fiscal Year, as mentioned above.
To sum up, the implicit bias section of the training teaches child-serving professionals and volunteers that mandatory reporting harms Black children and that to avoid that harm, mandatory reporters must engage in a lengthy deliberative process before making a report. Mandatory reporters learn nothing of the costs of not making a report, which include the possible death of a child. They also learn nothing about the different risks facing Black children, who are three times more likely than White children to die of maltreatment.2 Instead, they are told that “we are delinquent in addressing the institutionalized racism and bias that pervades our family and wellbeing systems. This has been perpetuated by the misconception that we are nobly rescuing children from dangerous situations.” The clear implication is that making a report is much more risky than not making one.
A Case of Mixed Messages
After at least an hour of training on implicit bias, mandatory reporters finally arrive at the original training, which seems mainly unchanged. They learn about how to respond to a child’s disclosure of abuse or neglect. They learn they must report when they have reasonable cause to believe a child has been, or is in immediate danger of, being abused or neglected. They learn what and how to report. They learn that the identity of reporters is confidential and that failure to make a report can be punished by a fine of up to $1,000 or imprisonment for up to 180 days. They learn about different types of abuse and neglect, which children have higher risks of being maltreated, situations in which CFSA does not intervene, what happens when a report is made, and how child welfare services work in the District of Columbia. They are told to “[r]eport any suspicion of child abuse and neglect,” and that “every call matters!” A key instruction is buried in the section on how to distinguish discipline from child abuse. It says: “The good news is, as a mandated reporter, you do not need to know the details or all the facts before making a report. You just need to be suspicious of abuse/neglect and CFSA’s response, if it does respond, will do the rest.” (This should be moved to the top and emphasized, as it may have been in an earlier version of the training). In closing, trainees are told that:
Abuse and neglect place children at great risk of physical and emotional injuries and even death. As a mandated reporter, the District is expecting you to do the following:
Recognize the signs of child abuse and neglect.
When children have the courage to disclose abuse or neglect to you, take them seriously.
When you suspect or know of incidents of child abuse or neglect, call CFSA at (202) 671-SAFE.
Be responsible for calling the CFSA Hotline yourself, even if you have informed your supervisor.
If necessary, be helpful and available during the investigation.
The fundamental conflict between the training’s two messages is clear. According to the original training, abuse and neglect are dangerous to children and it is our responsibility to report. According to the implicit bias section, it is reporting that is dangerous and needs to be inhibited. Neglect is a serious type of maltreatment according to the original training but a “code word”d according to the implicit bias section. It is not really surprising that the implicit bias element of the training seems to be in opposition to the preexisting content. Perhaps those who inserted this content would prefer to eliminate mandatory reporting training entirely and are just trying to minimize it within the requirements of current law. But the half-measure of trying to train the implicit bias out of mandatory reporters creates a training that simply does not make sense.
In addition to this fundamental disconnect, the training exhibits many factual errors and is padded with extraneous content. The factual errors are discussed in an addendum to this post. The extraneous content includes discussions of the racial wealth gap and instructions for “self-reflection, in which trainees are instructed to define their values by a three-step process that is painstakingly described in a three-minute video. Perhaps the most striking extraneous content is a section that describes in detail six types of “mental models related to diversity, equity and inclusion.” One of the six types is “active opposers,” who are typically deeply rooted in their choice to be a strong opponent of DEI. These are the people whose minds cannot be changed and who are committed to disrupting the work of DEI.” One cannot help wondering how the current federal leadership would respond if they knew of this content, and being offended at the disrespect for the time of busy professionals or volunteers.
In summary, there is a fundamental conflict between the original message of CFSA’s mandatory reporter training and the message of the implicit bias unit that has been added to it. Unlike the original message stressing the duty and importance of reporting suspected abuse and neglect, the new message states that reporting damages children and families of color and should be avoided whenever possible. This fundamental conflict is not unique to the District and by necessity affects all mandatory reporter trainings that attempts to temper the duty to report by inserting considerations related to race and ethnicity.
From U.S. Children’s Bureau, Child Maltreatment 2023, page 59. States reported that 6,04 per 100,000 Black children were found to be victims of a child maltreatment fatality compared to 1.94 per 100,000 White children. These are deaths that have been confirmed as due to maltreatment by child protective services, medical examiners, or police, a process that may be affected by bias. ↩︎
Addendum: Factual Errors in CFSA’s Mandatory Reporter Training Implicit Bias Module
The implicit bias module in CFSA’s mandatory reporter training curtains numerous factual errors and omissions. Here are a few.
“National studies by the US Department of Health and Human Services reported that minority children and in particular black children are more likely to be in foster care than receive in-home services even when they have the same problems and characteristics as White children.” I asked the CFSA’s Communications Director for a citation and I found the exact language in one of the three references that were provided–a 2019 ABA brief entitled Race and Poverty Bias in the Child Welfare System: Strategies for Child Welfare Practitioners. A footnote referred readers to an essay by Dorothy Roberts for PBS’ Frontline program. That essay in turn attributes the same quote to “a national study of child protective services by the U.S. Department of Health and Human Services” with no citation. When consulted, ChatGPT references the outdated 1996 National Incidence Survey of Child Abuse and Neglect, which has been superseded and contradicted by the more sophisticated study published in 2010.
“Rates of child abuse are not higher for children of color than white children. People of color do not treat their children worse than White families do. Racial disproportionality in CW is due to systemic racism, cultural misunderstandings, stereotypes, and biases that influence the decision to report alleged child report or neglect to CPS.” This is simply not true. First, we don’t have definitive evidence of child abuse rates as it occurs in secret, may not be reported, and investigations may not come up with the right results. But all the evidence we have indicates that Black families do abuse and neglect their children more than White families. This is likely due to the history of slavery and racism, which led to higher poverty and concentration in impoverished neighborhoods characterized by crime, substance abuse, unemployment, and limited community services, as well as a legacy of intergenerational trauma associated with these factors as well.
“Although African American families tend to be assessed with lower risk than White families, they are more likely to have substantiated cases, have their children separated, or be provided family based safety services.” I could not find any resource on the internet that indicates that Black families tend to be assessed with lower risk than White families It is true that Black children tend to have more substantiated cases, have their children removed, or receive in-home services. But that is before controlling for family characteristics that affect risk. The only research article cited by CFSA actually reported that when they controlled for family risk factors, agency and geographic contexts, and caseworker characteristics, Black children were not at significantly higher risk of substantiation or removal.
Complete Fiscal Year 2024 data now on the Dashboard of the District of Columbia’s Child and Family Services Agency (CFSA) reveal significant changes over the previous fiscal year. Most striking is a large jump in the number of incomplete investigations and a concomitant decline in “substantiated” and “unfounded” reports. The number of children entering foster care increased for the first time in over ten years. There was a drop in in-home case openings but a similar increase in foster care placements during the year. The agency did not respond to this writer’s questions about the meaning of these trends.
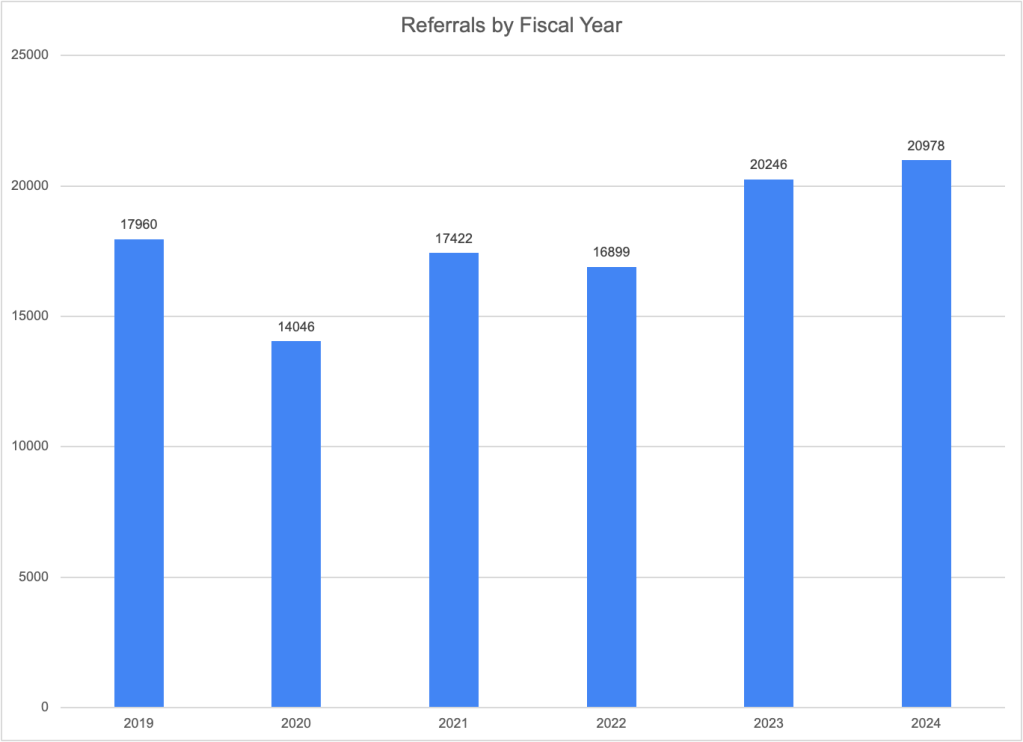
Referrals
Total referrals (or calls to the CFSA hotline) have increased for the second year in a row. After falling in 2020 and remaining below 2019 levels in 2021 and 2022, the number of referrals jumped from 16,899 in FY2022 to 20,246 in FY2023 and then rose more modestly to 20,978 in 2024–an increase of 3.6 percent. Prominent child welfare scholars like Emily Putnam-Hornstein have concluded that referrals are the best available indicator of actual maltreatment due to the strong correlation between referrals and future reports (regardless of the outcome of any associated investigation) and also evidence of the difficulty of correctly determining whether maltreatment has occurred. Thus, the increase in referrals may well be a sign of increasing maltreatment. Contributing factors might be the end of COVID-19 assistance programs and the growing mental health, substance abuse, and housing crises in the District.
Childcare and school personnel continued to make more than half of the referrals to CFSA, with another 13 percent coming from law enforcement and 11 percent from friends and neighbors. All three of these groups made more referrals in FY2023 than FY2024, while counselors, therapists, social workers and medical professionals made fewer, suggesting that children may be seeing fewer of these professionals with the disappearance of virtual options spawned by the pandemic.
Looking at CFSA’s response to the referrals, the largest portion, or 73 percent, were screened out. That compares to only 19 percent that were accepted for investigation. The remaining referrals were either linked to an existing investigation (three percent) or classified as an information and referral that does not involve an allegation of abuse or neglect. These percentages are quite similar to those of the previous year.
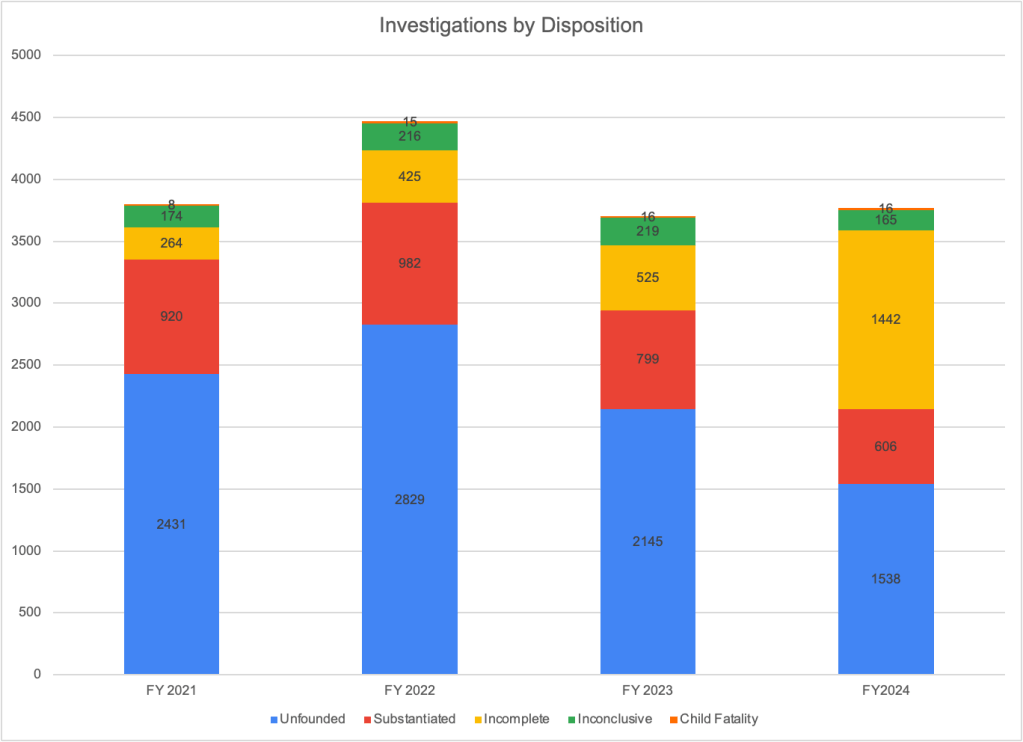
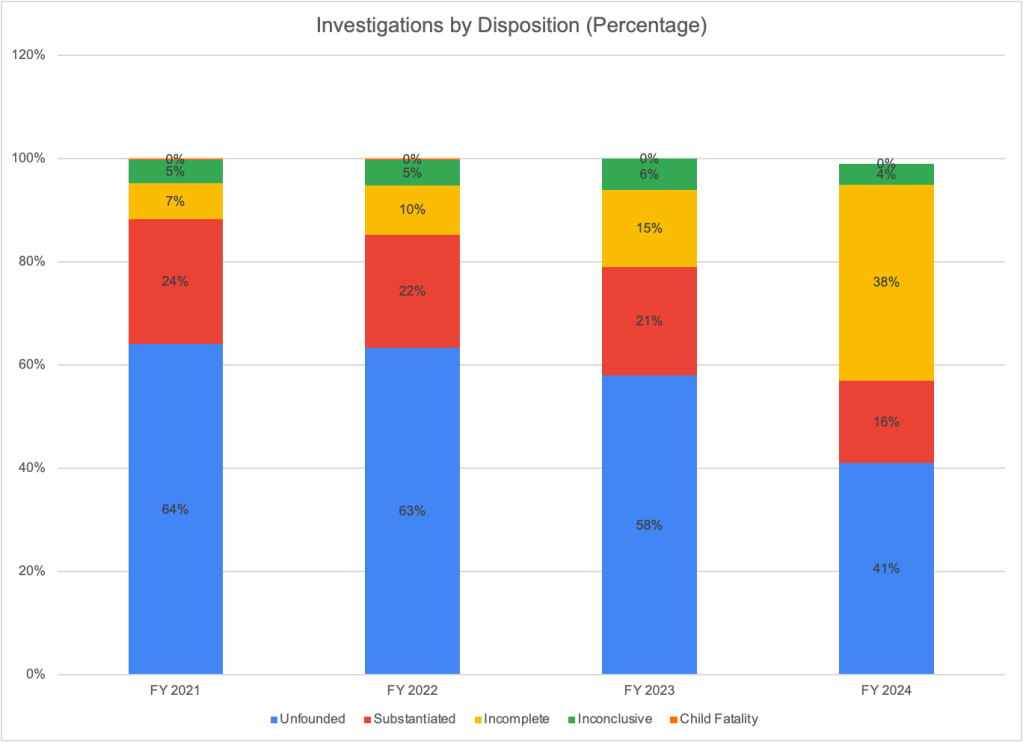
An investigation can have five different dispositions. According to the definitions provided in the Dashboard, unfounded means that there is not enough evidence to conclude that the child has been maltreated or at risk of being maltreated. “Substantiated” means that there is enough evidence to conclude that the child has been maltreated or is at risk of maltreatment. “Inconclusive,” means that “there is insufficient evidence to substantiate the report but there still exists some conflicting information that indicate the abuse or neglect may have occurred.” “Incomplete” means that the investigation could not be completed due to barriers like inability to locate the family, a family’s refusal of access to the home, or finding out that the family lived out of state.
There was a big jump in the number of investigations categorized as incomplete, from 525 in FY2023 to 1,442 in FY2024. That was an increase from 15% of all investigations to 38% of all investigations. As a consequence of the increase in incomplete investigations, the number and percentage of investigations that were unfounded and substantiated dropped drastically. The number of investigations that were substantiated fell from 799 (21 percent of investigations) in FY2023 to 606 (or 16 percent of investigations) in FY2024. Unfounded remained the most common disposition in FY2024, but the proportion of cases that were unfounded dropped from 58 percent to 41 percent.
CFSA’s communications director did not respond to several emails asking for an explanation of the the jump in incomplete investigations. But it seems likely that this trend stems from the workforce crisis that is affecting CFSA and other child welfare and human services agencies around the country. A spreadsheet that the agency provided to the DC Kincare Alliance shows 27 out of the 36 social workers performing investigations as of August 2024 were carrying more than the 12 to 15 cases that CFSA uses as an indicator of satisfactory performance. This included 19 social workers carrying 20 or more cases and five social workers carrying more than 30 cases. Even more concerning is that the number of social workers doing investigations fell from 42 in January 2024 to 36 in August 2024, according to the spreadsheet.
If social workers are not able to complete the required interviews and collect needed information timely, endangered children may suffer further harm. It is possible that most of the incomplete investigations have been essentially concluded with a determination of findings, leaving only the completion of needed documentation and forms undone as workers hurried to start new investigations. Such a scenario might be somewhat less alarming but would still raise concerns that overburdened social workers are not able to thoroughly investigate allegations, thereby endangering vulnerable children.
In-Home Case Openings and Foster Care Placements
The table below shows the number of in-home case openings and children entering foster care by year. These two numbers cannot be added together because because in-home entries are reported at the case level (with multiple children in many cases) and foster care entries are reported at the child level. However the trends over time can be compared, showing that the number of in-home cases opened dropped between FY2023 and FY2024 while the number of children entering foster care increased. This was the first time the number of children entering foster care increased since FY2021, after the drop in foster care placement due to COVID-19.\
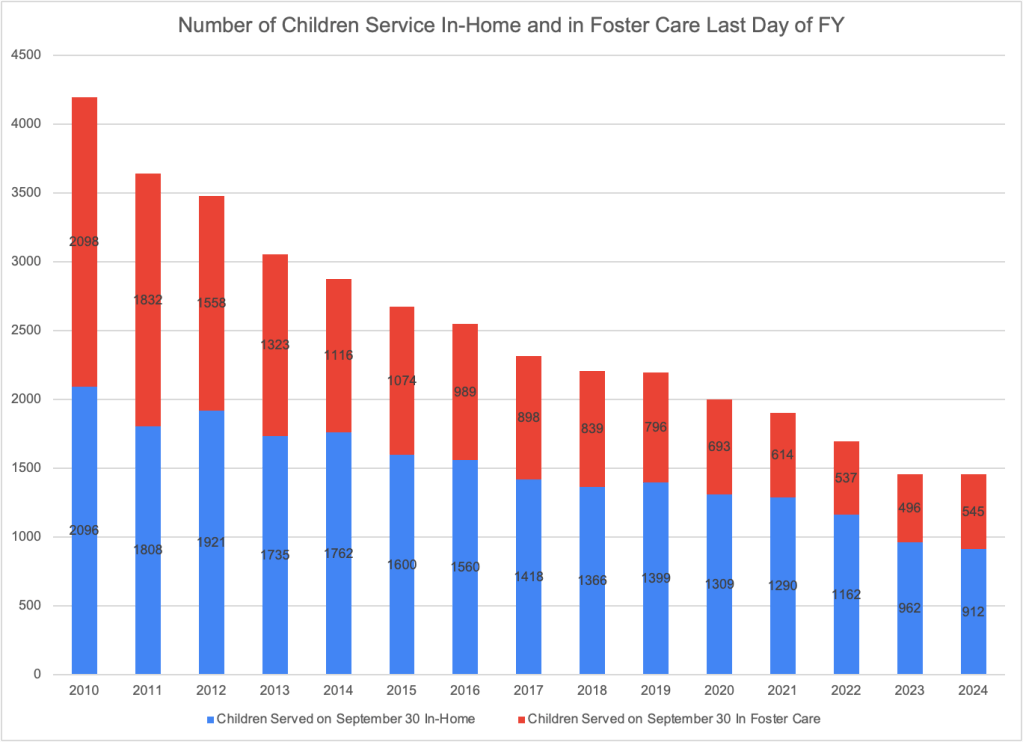
The total number of children served in home and in foster care on the last day of every quarter are available on the CFSA Dashboard and can be added to yield the total number of children served on that date. The chart below shows that the total number of children served on the last day of the fiscal year (September 30) stayed basically the same between FY2023 and FY2024. But the number of children being served in their homes decreased by 50 while the number in foster care increased by 49. FY2024 reverses a trend of annual decreases in the number of children in foster care going back at least as far as 2011.
The increase in the number of children in foster care between September 30, 2023 to September 30, 2024 reflects an excess of entries to foster care over exits from care during FY2024. Specifically, the number of children in foster care at the end of the fiscal year should reflect the number of children in foster care at the end of FY2023, plus the number of entries to foster care during the year, minus the number of exits from foster care. While there is a discrepancy of two between the results of this calculation and the foster care caseload reported by CFSA, the numbers confirm that there were about 50 more entries than exits, so the caseload increased. A similar calculation cannot be performed for children served in their homes, as the entry data are based on cases, not children.
It may be reassuring that the number of children served by CFSA changed so little in FY2023. One can hope that despite the high percentage of incomplete investigations, CPS workers are doing what is necessary to find the children that need help and simply leaving some of the paperwork for later. However, such a situation is not sustainable without endangering children. And the 3.6 percent increase in the number of referrals between FY2023 and FY2024 was not met with an increase in the number of children served, which may be a result of the incomplete cases.
It is not possible to understand the FY2024 data without further information from CFSA. How alarming the increase in incomplete investigations may be depends on whether these investigations are truly incomplete or basically finished except for forms and documentation. More concerning still, CFSA caseload data indicates that there are fewer than half the number of social workers doing this work now than in previous years. It is good that the total number of children being served has not dropped precipitously along with the drop in completed investigations. But the public needs to know more about how CFSA is functioning and what it is doing to alleviate the workforce crisis.
To my readers: This blog summarizes a report that is the culmination of nine months of work. It is part of my advocacy for children in the District of Columbia, which I share in my blog, Child Welfare Monitor DC. But I think this post and the underlying report will be of interest to child advocates, policymakers and researchers around the country because the findings and issues discussedare widely applicable.
“We are not here to save children.” That is what I was told on the first day of my training as a child protective services worker at the District of Columbia’s Child and Family Services Agency (CFSA). And indeed, the District is on the cutting edge of the current movement in child welfare around the country that considers child protective services as a “family policing system” that unnecessarily harasses and separates families, especially families of color. The problem with this perspective is that some families do not provide a safe environment for children to grow and develop. In some of these families, children die. That is what happened to the 16 children whose cases are discussed in a new report, which is summarized in this post. And indeed, analysis of the limited information provided suggests that CFSA did not take advantage of the opportunities it had to protect children even after long histories of CFSA involvement in their families. As a result, three children were beaten to death, three more were poisoned by opioids, and others died of burns, a car accident, and unknown causes when the deaths might have been preventable if the agency had been more protective.
When a child dies of abuse or neglect after that child’s family has been on the radar of the agency designed to protect children, it is important for the public to know whether and how this death could have been avoided. The essential question is whether the agency could have prevented the death by doing something differently. Did staff miss any red flags, and therefore fail to take action when necessary? If the death was preventable, what factors must be remedied in order to prevent such failures in the future? It is not enough for the agency itself to have access to this information, or to have an internal team review it. Agencies can fail to learn from their mistakes when they are blinded by ideology, self-interest or just inertia.
For those reasons, federal law requires every state to have a law or program that includes “provisions which allow for public disclosure of the findings or information about the case of child abuse or neglect which has resulted in a child fatality or near fatality.” In compliance with this requirement, DC Code requires the Mayor or the Director of CFSA, upon written request or on their own initiative, to provide findings and information related to “[t]he death of a child where the Chief Medical Examiner cannot rule out child abuse, neglect, or maltreatment as contributing to the cause of death.” In March 2023, we requested such findings and information for all the fatalities that met the criteria and were reviewed by CFSA’s internal fatality review team between 2019 and 2021. It took more than six months of meetings and emails to receive the information that is presented in this report. We agreed to restrict our request to cases reviewed in 2019, 2020 and 2021 and to withdraw our request for information on near-fatalities, which CFSA only began tracking in October, 2022.
Not surprisingly, CFSA interpreted the disclosure requirements in a way that restricted the information provided as much as possible. If a medical examiner did not rule the manner of death to be an abuse or neglect homicide or “undetermined,” no information was provided. Therefore, the agency did not release any information on cases where the manner of death was labeled as accidental, even if it found a parent responsible for the death or removed the children. The “accidental” deaths for which information was not provided included one child who died after he was left in a baby swing for two hours, which most ordinary people would consider to be neglect. The death of seven-week-old Kyon Jones, whose mother told police that she threw his body in a dumpster after she rolled over him while high on PCP, was not included because his body was never found and therefore it did not meet the criteria for release of the information–even though CFSA removed the surviving children from their mother.*
In addition to omitting some cases in which neglect or abuse played a role, CFSA heavily redacted the information it did provide, with many pages and large portions of others blacked out. CFSA refused to provide the names of the children, parents and caregivers, providing a rather convoluted interpretation of DC Code, which clearly requires the release of this information. (See the full report for more information about their reasoning). In three cases, the child’s identity was clear from media coverage of the case, and we used the child’s name. A major source of redactions was the exclusion of “personal or private information unrelated to the child fatality.” It appears that CFSA’s legal team interpreted this term much more broadly than a social worker or researcher would, because they redacted almost all information about parents’ history of criminal activity, substance abuse, mental illness, and domestic violence–which are obviously relevant to many of the fatalities we are discussing.
On investigations, it is unfortunate that DC Code requires that the agency release only ”a description of the conduct of the most recent investigation or assessment” rather than all investigations regarding the family in question. It appears that the agency interpreted “the most recent investigation” as the fatality investigation itself rather than the most recent investigation before the fatality, but the law ought to require a description of all previous investigations. The agency also disregarded language that requires it to provide “the basis for any finding of either abuse or neglect.”
For most cases, we received very little information aside from a list of the previous referrals (reports to the CPS hotline) including only the date of the report, the allegation category and the disposition; an account of in-home and foster care case activities for the families that had such cases; and an account of the investigation of the fatality itself. The information about the parents was heavily redacted, and almost the entire history of agency involvement was blacked out in most cases. Despite the limited information provided, the redacted summaries included some new information, some of which was startling and disturbing. The report is based on the 16 case summaries provided by CFSA, occasionally supplemented with information from the agency’s annual fatality reports, which are available to the public. These cases affected 15 families, as one family had two fatalities in one year. Unless otherwise noted, the information is based on the case summaries. The full report, from which this blog is excerpted, contains summaries of each case.
Cause and Manner of Death
CFSA classifies child deaths by cause and manner. “Cause of death” is the specific disease or injury that led to the death. Manner of death refers to the circumstances that caused the death, and falls into five categories: natural, accidental, suicide, homicide, and undetermined. Of the 16 cases for which information was provided by CFSA, three (19 percent) were abuse homicides, six (37 percent) were neglect homicides, and seven (44 percent) were undetermined in manner. The latter were the cases for which CFSA provided information because the Medical Examiner was unable to rule out child abuse or neglect homicide as the manner of death.
The most common causes of death were blunt-force trauma and opioid poisoning, each claiming the lives of three children, as shown in figure below. The remaining children died from a variety of causes, including drowning, asphyxia, thermal and scald injuries, injuries from a car accident, and unknown causes.
Abuse deaths: Blunt Force Trauma
Three of the children died of blunt force trauma–one of the two most common causes of death in the sample. The murders of two of these children – Makenzie Anderson and Gabriel Eason – – became known to the horrified public through press coverage of their deaths in February and April of 2020. Each of them died from head trauma inflicted by a parent or stepparent. Makenzie suffered from multiple contusions to the face and head, skull fractures, and other injuries, and her mother pleaded guilty to manslaughter, receiving a ten-year prison term with seven years suspended on the condition that she obtain mental health treatment and have no unsupervised contact with children. Gabriel’s autopsy found abrasions and contusions to the head, face and torso; contusions to the heart and thymus gland; liver and kidney laceration; new and healing fractured ribs; and a brain hematoma. His stepfather was sentenced to 12 years and eight months in prison and his mother, who did not seek medical help for Gabriel or his critically-injured three-year-old brother, was sentenced to four years of probation and three years of supervised release.
But there was a third homicide by blunt force trauma. A three-year-old girl died of trauma to the abdomen in the home of an aunt where she was placed by CFSA after being removed from her drug-addicted mother. Her injuries included contusions to the forehead and abdomen, a lacerated liver, and blood in the abdominal cavity. No charges were filed against either the aunt or her boyfriend, and the case received almost no public attention.
Neglect deaths: Opioid Poisoning and other causes
Three children (a three-year-old girl, a three-year-old boy, and a three-month-old girl) died of synthetic opioid toxicity, with fentanyl implicated in all three deaths. (One of the children had also ingested a controlled substance called eutylone.) There is no information about how the children might have ingested the drugs, but all lived with parents who were known or alleged to abuse substances. These deaths never became known to the public, which is not surprising since it appears that none of the parents were arrested or charged.
A 17-month-old boy died of “complications of thermal and scald injuries,” and his mother told the investigator that she had no idea how it happened or how he ended up face-down in the bathtub several hours later. A seven-year-old died of injuries from a car accident. His mother was a long-time substance abuser and was arrested for Driving Under the Influence (DUI) in the accident. She was driving from Florida to Washington and her children were not sitting in car seats or belted in. A five-month-old boy died of asphyxia by drowning after being left alone in the bathtub with a one-year-old sibling while their mother searched for her car keys.
Deaths for Which the Manner was Undetermined
Two deaths has known causes but the manner – whether abuse or neglect or something else – was not determined. A twelve-year-old girl with asthma died of an untreated bacterial infection and pneumonia but also had enough bruising from two separate beatings in the previous two days to support a CFSA substantiation of the mother for physical abuse. It is unclear why this was not considered a medical neglect homicide. A ten-month-old girl died of asphyxia but the manner of death was undetermined. Her mother had left her in the care of her father and returned to find her unresponsive.
The cause as well as the manner of death was unknown or undetermined in five cases. These included an 18-month-old boy with a subdural hematoma, which could have been caused by abuse or a fall, an 11-month-old girl whose mother reported leaving her unsupervised on her stomach with a bottle in her mouth for about 40 minutes, a nine-month-old boy put to bed with a bottle and found face-down on a pillow; a two-month-old girl who died while sleeping with her mother, and a three-month-old girl found unresponsive by her parents one morning. Unsafe sleep practices may have contributed to some of these deaths, but other unsafe sleep fatalities were categorized as accidents, for which case summaries were not provided.
Demographics
A quarter of the children who died were younger than six months old and half of them were one-year-old or younger. Another quarter were two or three. This is not surprising as young children are more vulnerable and similar results are found nationally. But older children were not invulnerable to abuse or neglect, including the seven-year-old who died in a car accident and the 12-year-old who died of an untreated bacterial infection and pneumonia.
Fifteen of the decedents were African American and one was classified as “African-biracial.” According to the latest data from Kids Count, 54 percent of children in the District of Columbia are Black. So Black children were overrepresented among the children who died of maltreatment or possible maltreatment. The overrepresentation of Black children among children who died points to Black children’s particular need for protection. And it suggests that current emphasis in the District and around the country on reducing the involvement of Black families in child welfare may cause more suffering and more deaths among Black children.
The prevalence of large families among those that lost a child due to abuse or neglect is striking. More than two thirds of the mothers of children who died by maltreatment had four or more children. The average mother in the group had 4.6 children, often with more than one father.
Histories of System Involvement
All the families had been the subject of at least one report to the CFSA hotline before the fatality, or else they would not be included in this report. But many of the families that lost a child had experienced a large number of reports prior to the fatality. Among the 16 fatalities included in this report, only six occurred in families that were the subject of five reports or fewer in the last five years. Five occurred in families that had between six and 10 reports, three occurred in families with 10 to 15 reports, and one family had 24 reports. Three of the families had actually experienced a previous child fatality–a shocking statistic considering the rarity of child fatalities overall.
The families of the two children – Makenzie Anderson and Gabriel Eason – whose abuse homicides shocked the District of Columbia in February and April 2020 were both known to CFSA before the deaths, and the last report to the hotline came five months before the fatalities of both children. Makenzie Anderson’s family was reported to the hotline eight times within five years of her death. The last report alleged exposure to unsafe living conditions, inadequate supervision, and substance abuse by a parent, caregiver, or guardian. All those allegations were unfounded (not confirmed) by CFSA. Gabriel Eason’s family was the subject of 17 prior calls to the hotline since 2012, including 12 in the five years preceding Gabriel’s death. The most recent report was for unexplained physical injury in October 2019 and was also unfounded by CFSA.
Substance abuse by the parent or caregiver was the most frequent allegation CFSA received regarding the families in the five years before the deaths, with 30 substance abuse allegations collectively accumulated by the families of the 16 dead children during that period. Another eight reports concerned positive toxicity of a newborn, a reflection of parental substance abuse. Substance abuse by the parents was observed or alleged in the families of all but four of the victims included in this report. Inadequate supervision was the second most common allegation, with 25 allegations concerning the 15 families. Almost as common was educational neglect, referring to children with excessive school absences, with 24 allegations received in the five years preceding the fatality. Ten of the 15 families had at least one report for educational neglect before the child’s death. Another major theme was exposure to domestic violence, with 17 allegations received by the families. Domestic violence was mentioned in nine of the 16 case histories as the subject of an allegation or in notes from social workers or police.
Most of these families could be described as “chronically neglectful.” According to the Child Welfare Information Gateway, “Chronic child neglect occurs when a caregiver repeatedly fails to meet a child’s basic physical, developmental, and/or emotional needs. Chronic neglect can have long-term, negative consequences for child health and well-being.” Working with chronically neglectful families is especially difficult and requires special training and skills, which many CFSA social workers may lack. Perhaps that is one reason why they struggled so hard to engage some of these families. Four of the children died while an in-home case was open. Three out of four of the in-home case narratives from CFSA portray caregivers who evaded offers of help from CFSA and other providers and refused to cooperate with efforts to monitor conditions in their homes.
System Failures
The information received suggests several areas where failures in policy and practice by CFSA and other agencies may have allowed these deaths to happen. These areas include:
Screened out and unsubstantiated reports: Research points to the difficulty of determining correctly whether a child has been maltreated, as well as the absence of significant differences in subsequent outcomes between children with a substantiated allegation of maltreatment and those with an unfounded allegation. Without information on how hotline and investigation decisions were made, we cannot assess the agency’s performance in these areas. But the fact that most previous reports for families with a subsequent death were screened out or unfounded is concerning.
Flawed management of in-home cases: Four of the deaths reviewed here happened while an in-home case was open for the family. In three of these cases, workers struggled to complete face-to-face visits with the families because parents evaded these visits. Social workers and supervisors could have filed a petition to involve the court, an option known as “community papering.” But they did not exercise this option–or they started too late, as in the case of the child who died after a meeting was finally scheduled to discuss community papering the case. The meeting was cancelled after the agency received word of the child’s death.
Too many chances: The mother of the seven-year-old killed in the 2020 car accident had been given numerous chances to recover from drug addiction and had relapsed many times over 18 years of involvement with CSFA. The family of the 17-month-old who died of complications of thermal and scald injuries had 24 referrals to CFSA between 2016 and 2021. Three in-home cases were opened and closed, but the children were not removed until the little boy died.
A fragmented health care system: In its findings on Gabriel Eason’s death, CFSA pointed out that Gabriel was taken to different medical providers for his various injuries. Because they use different information systems, the providers could not see records of the earlier injuries.
The reaction of CFSA and the criminal justice system after the fatalities obviously did not contribute to the fatalities themselves but may illustrate a pattern that contributes to future deaths. Specifically, CFSA’s tendency to place siblings informally after fatalities and the police and US District Attorney’s failure to charge parents raise concerns.
Informal placements after fatalities: CFSA, and child welfare agencies around the country, have been criticized for relying on informal placements with family members, rather than formally removing the children, placing them with the relatives, and opening a case to monitor their safety and well-being. In at least four of the 16 cases reviewed here, CFSA did not officially remove the siblings of the children who died but instead relied on informal placements with fathers or other relatives to keep them safe. Nothing was done to assure that the children were not returned to the home from which they had been removed as soon as the investigations closed, or to verify that the parents or caregivers had rectified the conditions leading to the child deaths.
Failures by the criminal justice system: The failure to bring charges against some of the parents and caregivers described here is quite concerning, particularly in the case of the three-year-old who died of blunt-force trauma and the infant and two three-year-olds who died of opioid poisoning. There has been considerable criticism of the US Attorney’s office in the District (which handles adult criminal prosecutions) for its low rate of opting to charge people for crimes. We do not know if the problem is the Metropolitan Police Department’s failure to bring the cases to the US Attorney or the latter’s failure to pursue them.
Recommendations
Without seeing the full case studies that were available to CFSA’s internal review committee, we cannot make detailed recommendations about how to avoid child maltreatment fatalities for children known to CFSA. The minimal recommendations that CFSA’s internal review team made show the need for the City Council, advocates and the public to have access to these complete case studies: in its 2021 report the agency made no recommendations other than those dealing with the fatality review process! Therefore, our first recommendation is to the City Council, urging it to require that CFSA release comprehensive case histories on all proven or suspected child maltreatment fatalities. Our next blog post will discuss the legislative changes that are needed.
The lack of information on how screening and investigation decisions in particular were made precludes specific recommendations. Perhaps a new audit of the hotline is in order. Some changes to hotline screening policy might be advisable, especially around educational neglect. School absences should be investigated regardless of the age of the child (requiring a change in the law) and their academic performance. And perhaps investigative workers could benefit from better training in forensic interviewing techniques that might help them better evaluate parents’ and childrens’ statements for veracity and perceive more subtle signs of abuse or neglect.
The case narratives make clear that in-home social workers struggled to complete home visits to the families of the children who later died. The agency must change its policy to encourage “community papering,” making court involvement routine after a certain number of missed visits or other instances of noncooperation. CFSA might also want to consider strengthening its in-home practice, perhaps by reinstating the Chronic Neglect Units, which were eliminated barely a year after they were implemented. These units would employ specially-trained social workers with lower caseloads and longer time periods to work with families.
Despite the current ideology favoring family preservation and reunification at all costs, the agency must also recognize that sometimes it must give up on a parent and find a safe, permanent alternative for the children. Giving parents multiple chances with successive children over many years belies the true purpose of child welfare services – to protect children.
Not all needed changes fall in CFSA’s bailiwick. Reforms in the criminal justice system are also necessary to ensure that parents who killed one child cannot harm more children. Couples who refuse to cooperate with prosecutors, and parents who expose children to opioids due to their own abuse or drug dealing must also be charged. Other jurisdictions do it, and the District must do it as well.
DC Health and medical providers also have a crucial role to play in making children safer. Encouraging the adoption of a comprehensive medical information platform across the region to prevent families from using different doctors to hide abuse and neglect would be a welcome step. A campaign by DC Health to educate young women on how an early pregnancy, especially when followed quickly by others, compromises their future and that of their children, is a crucial necessity. It must be accompanied by improved access to long-acting reversible contraceptive methods.
In summary, even with the very minimal information we received, some conclusions emerge. CFSA’s extreme deference to parents and guardians emerges clearly through the redactions in these narratives. This is in direct contrast to the picture that is being painted by the foundations, advocacy groups and public agencies dominating the child welfare conversation. Their accounts portray interventionist child welfare agencies that remove children rather than giving their families the help they need and want. We are seeing the opposite here: families who evade offers of help from the agency and providers and refuse to cooperate with efforts to monitor conditions in the home. The goal of such parents often appears to be to avoid surveillance by outsiders rather than to improve their ability to care for their children. And CFSA workers often seem unwilling or unable to intervene in a way that will protect these children.
‘The tragic deaths of children whose families are known to CFSA are the tip of a much larger iceberg. For every child who dies of abuse or neglect, an unknown number of others are living in fear or pain from abuse, suffering chronic neglect that will cause lifelong intellectual an emotional damage, or lacking the loving attention necessary for optimal mental, emotional and physical development. Sadly, it is only the children who die whose cases can be used to learn lessons to prevent similar tragedies in the future. This information must be public, so that the public can push for a system that protects all children who are not receiving the parental care they need to survive and thrive.
*The case, which received media coverage, was included and easily identifiable in