The last time Evgeny and Evgenia saw their eight-year-old son Maksim was on May 15. That’s the day that the couple refused to board a commercial flight taking them back to Russia, from which they had fled fearing persecution for their opposition to Valdimir Putin. On August 24, Maksim will turn nine years old in foster care. He has not seen his parents since May 15 and has given up hope for a reunion. Maksim’s family is not unique. The New York Times found a total of nine cases in which parents have been separated from their children after refusing to comply with deportation orders in this new version of the family separation policy that generated such a strong backlash in the first Trump Presidency.
As reported by Hamed Aleaziz in the New York Times and its podcast, The Daily, Evgeny and Evgenia, who prefer not to have their last name revealed, fled Russia because of their political activism. As supporters of Putin’s murdered enemy Alexei Navalny, they felt that they were at risk of losing their freedom, their livelihood or even their lives if they remained in Russia. They fled to Mexico, with the hope of getting an appointment to apply for asylum in the US through a cellphone app created by the Biden Administration to enable asylum-seekers to schedule an appointment from outside the country. But Trump shut down that program when he took office. Seeing no other option, the family went to a port of entry on the southern border and explained that they were there to seek asylum. But asylum applications had been shut down completely at the southern border, and the family was detained in Border Patrol custody. After two weeks, they were taken to JFK airport to be deported.
At the airport, ICE officials told Maksim’s parents that they would be separated from their son if they did not board the flight to Russia. But Evgeny was trying to prevent a longer separation in Russia since he expected to be detained there. With many tears on all sides, Evgeny and Evgenia were taken to detention and Maksim was taken to a shelter for unaccompanied immigrant children. It was May 15, 2025.
In the first Trump administration, thousands of families were separated at the border as a way to deter people from entering the country illegally. Parents were arrested and criminally charged for illegally entering the country and their children were taken away. This policy created a massive outcry worldwide and Trump ended it in 2018. Today, border crossings have slowed to a trickle and the new administration is focused on deporting those who have already crossed. Migrants from many countries can be shackled, cuffed, and loaded onto chartered flights. But for those who came from countries like Russia that do not accept deportation flights from the US, the government must use commercial flights to deport unwanted migrants. And commercial airlines do not accept passengers in restraints or who make a scene. Hence the choice offered to Maksim’s parents.
As Aleaziz puts it for the Times, “the new cases suggest that the administration has decided to use family separation as a tool, at least in some instances, to persuade families to leave and to create a powerful deterrent for those who might come to the United States illegally.” He found nine families who have refused deportation and been separated. But he does not know how many families have faced this choice, including those who have agreed to return to the countries from which they came. A spokeswoman for the Department of Homeland Security told him that there is no family separation policy and that “these families had the right and the ability to depart the country as a family and willfully choose to not comply.”
Evgeny and Evgeniia have not given in–a fact which lends credence to their fear of persecution in Russia. Since Maksim was taken from them, they have passed the rigorous screening for the validity of their asylum claim. Now the government cannot deport them to Russia but can send them to a third country if one can be found. Maksim has been transferred to foster care. His conversations with his parents are heartbreaking; At first he was counting the days that he has been apart from his parents but has now stopped. At this point, he has given up hope that he will see his parents again. Maksim will turn nine on August 24 and it looks like he will not be with his parents on that special day.
My regular readers know that, unlike some people who want to abolish foster care, I support the separation of children from their parents when there is abuse or neglect that is so severe that the child cannot be protected without removal. But perverting these practices in order to deter asylum-seekers is state-committed child abuse. Allowing Maksim to spend his ninth birthday in foster care as a lesson to families with valid asylum claims not to enter the United States is heartless beyond belief. Can a groundswell of opposition be generated and end this family’s ordeal and that of others in a similar situation? I certainly hope so.
Reactive Attachment Disorder (RAD) is a diagnosis that is included in the DSM and often applied to foster and adopted children. While RAD refers to a pattern of inhibited, withdrawn behavior, some controversial therapies (often described as varieties of “Attachment Therapy”) are based on a distorted definition of RAD, or on an unauthorized diagnosis of “attachment disorder” that includes a deep-seated rage that if unaddressed will result in antisocial and even criminal behavior.
Among the practices included these controversial therapies are severe disciplinary methods including the establishment of total parental control over children’s actions, including eating, drinking and using the toilet.
Many of these Attachment Therapy technique include a component that involves forcing the child to express underlying rage through physically coercive methods that may include being held down by several adults for as much as three to five hours. Several child deaths have been attributed to such methods.
In order to prevent more damage to children, it is necessary to adequately vet prospective adoptive parents for their readiness to parent children with challenging behaviors due to early trauma and deprivation. Even for parents who are able to meet the challenge, training and continued support are necessary.
Unbelievably, some adoptive parents have not been charged even when their parenting techniques have led to the deaths of their children. It is absolutely necessary for parents who use abusive parenting techniques to be charged and tried in court. Adequate investigations are necessary in order to ensure that the conditions that lead to such cases are identified and remedied.
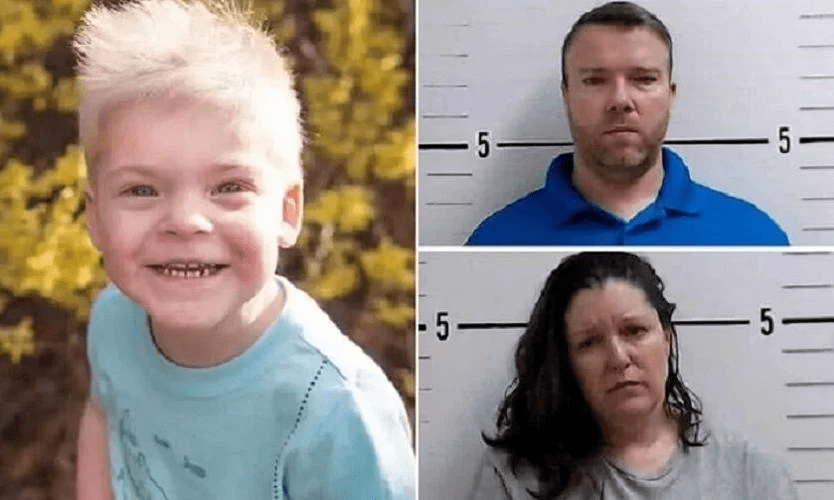
On January 5, 2023, according to a police warrant filed in Surry County, North Carolina, Joseph Wilson received a text from his wife telling him that something was wrong with their four-year-old adopted son Skyler after he was “swaddled.” She attached a picture of Skyler lying face down on the floor, wrapped in a sheet or blanket with duct tape attaching him to the floor. “Swaddling” is a practice used in many cultures to comfort infants, but Wilson told police he was referring to a parenting technique learned from a parenting expert named Nancy Thomas. (Court documents also state that one of the Wilsons’ former employees described recorded Zoom counseling sessions the couple had with Thomas.) Skyler died at Brenner Children’s Hospital in Winston-Salem on Jan. 9 of a “hypoxic, anoxic brain injury,” meaning that oxygen was unable to reach his brain due to the “swaddling.” Skyler’s adoptive parents, Jodi and Joseph Miller, have been charged with murder and felonious child abuse and are awaiting trial, which has recently been postponed–for the second time–from June 2 to December 1, 2025.
After Skyler’s death, police recovered surveillance cameras and arm and ankle restraints that Wilson had told them his wife used on Skyler during “swaddling.” A former foster parent of Skyler and his brother told police that Jodi Wilson had told her about using practices like “food restriction, the gating of Skyler in a room for excessive ‘alone’ time, and the exorcisms of both children.” The former foster parent was concerned enough to call Child Protective Services a month before the incident that killed Skyler.
Nancy Thomas, mentioned as the source of the swaddling technique and as a counselor to Skyler’s parents, is perhaps the most prominent exponent of a group of approaches to that the American Professional Society on the Abuse of Children (APSAC) described in a 2006 report as “controversial attachment therapies.” These therapies are generally directed at children with “attachment disorders.” The only such disorder that is officially recognized by the mental health community is “Reactive Attachment Disorder” (RAD), a diagnosis that is included in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). This diagnosis involves “a consistent pattern of inhibited, emotionally withdrawn behavior toward adult caregivers” as well as a “persistent social and emotional disturbance characterized by behaviors like minimal responsiveness to others, limited positive affect, and “episodes of unexplained irritability, sadness or fearfulness.” To be diagnosed with RAD, the child must have “experienced a pattern of extremes of insufficient care,.” which explains why this diagnosis is often applied to children who were adopted from orphanages abroad or foster care in the US. Some practitioners of these controversial attachment therapies, like Nancy Thomas, prefer to speak of children with “attachment disorder,” which is not included as a diagnosis in the DSM. Others use the term RAD but ascribe to that term a variety of symptoms that are not part of the DSM definition.
Whatever term they use, practitioners of controversial attachment therapies tend to believe that children who experience early adversity become “enraged at a very deep and primitive level.” This suppressed rage is said to prevent the development of attachment to caregivers and others and to lead to severe behavioral problems, such as violent behavior. These children are described as failing to develop a conscience, not trusting others, seeking to manipulate and control others, and at risk of developing criminal and antisocial behaviors. According to Nancy Thomas, some famous people with “Attachment Disorder” who did not get help in time include Adolph Hitler, Saddam Hussein, Jeffrey Dahmer, and Ted Bundy.
As described in the APSAC report, these controversial attachment therapies suggest that “parenting a child with an attachment disorder is a battle, and winning the battle by defeating the child is paramount.” Parents are often counseled to start by establishing total control over all the child’s actions, and requiring immediate obedience to parental commands. Nancy Thomas’s book, When Love Is Not Enough: A Guide to Parenting Children with RAD-Reactive Attachment Disorder, includes advice like “In the beginning, your child should learn to ask for everything. They must ask to go to the bathroom, to get a drink of water, EVERYTHING. When it starts to feel that they must ask to breathe, you are on the right track.” Another quote: When given directions it is unacceptable for the child to ask ‘”‘why?” or ‘what?’ NEVER answer these questions….Remember, have a consequence ready when a rule is challenged.” Thomas also recommends putting an alarm on a child’s bedroom door, and the window if necessary. Other techniques that have been recommended by attachment therapists include keeping the child at home (even counseling home schooling), barring social contact with others, assigning hard labor or repetitive tasks, and requiring prolonged motionless sitting.
Many proponents of controversial attachment terapies also believe that a child’s rage must be “released” before he or she can function normally. This release is often provided through physically coercive methods that may include being held down by several adults for as much as three to five hours. These techniques can be traced to “holding therapy,” a technique developed by a child psychiatrist named Foster Cline, who was ackhowledged as a mentor by Nancy Thomas in her book. Cline was admonished and restricted from using parts of his holding therapy model by the Colorado Board of Medical Examiners after members saw video of an 11-year-old being subjected to physical and verbal abuse while being restrained.
“Holding therapy” and similar methods designed to address “attachment disorder” have been implicated in the deaths of several adopted children, including that of three-year-old Krystal Tibbets, who died in 1997 when her adoptive father “applied the full weight of his body on the girl by lying across her and pressing his fist into her abdomen,” a technique he said he was taught by a therapist; four-year-old Cassandra Killpack, who in 2002 was forced to guzzle two quarts of water while her arms were bound, and 10-year-old Candace Newmaker, who suffocated in 2000 by a “therapist named Connell Watkins during a 70-minute “rebirthing ceremony” that was supposed to treat her attachment disorder. Nancy Thomas was working for Watkins at the time of Candace’s death. The “swaddling” technique that killed Skyler Wilson is an example of such a method.
Advocates of controversial attachment therapies have come to the defense of Skyler Wilson’s parents. The President of the Board of a nonprofit called Attach Families, Inc. shared an article on Facebook about Skyler’s death with the following preface: “These tragedies are always written one sided with no Investigative reporting, sadly…They obviously were using a swaddling technique that some Professionals promote for Attachment. This is a tragedy. But before these parents are “burned at the cross” our Families want more information.” The Page also posted this: “As we have seen hundreds of others making our Families look like monsters. When the truth is we try and will try ANYTHING to help our children. This is what we are trying to help them heal from before they get too big for us to physically handle their rages. Rages in which they inflict self harm. Rages where they slam their heads over and over on purpose. Rages in which we try to protect them from themselves and others around them. If you don’t live it 24 hours a day you have no idea what it is like.” Attached was an article about a Kansas teen who was arrested in the killing of his mother. The article contained no details about the teen or his mother. It is hard to understand how this talk of rage would apply to four-year-old Skyler. His former foster parent told a reporter that Skyler “was so tiny and small but had a heart three times bigger than he was…”
In some cases, the parents themselves, after reading misleading literature about children with RAD may invent their own disciplinary practices or use those inherited from their own upbringings or family traditions. The Denver Post recently wrote about Isaiah Stark, a seven-year-old who died in 2020 from ingesting too much sodium, likely from drinking olive brine. The newspaper learned that Isaiah’s adoptive parents were forcing him to eat olives and drink olive brine as a form of punishment for his behavior. According to a report from the state’s Child Fatality Review Team, the mother blamed all of Isaiah’s difficult behaviors on RAD and both parents attributed his actions to “manipulative behaviors and wilfulness.” At the funeral, she described Isaiah’s death as “God rescuing him.”
Isaiah Stark’s parents were never charged for his death. Since there was no trial, the public never learned whether the parents received any sort of parenting advice from an “expert.” The failure to charge parents who have tortured and killed adoptive children is all too common: witness the case in Florida of Begidu Morris, whose parents were not charged after starving, confining and beating him for years, ostensibly because the person who actually killed him could not be determined. As developmental psychologist Jean Mercer writes, plea bargains and the failure of investigators to follow up on the development of abusive parenting practices mean that we often don’t know whether abusive parents drew on outside influences or their own family histories or imaginations for the practices that led to a child’s injury or death.
Concern about controversial theories and methods of “Attachment Therapy” about twenty years ago prompted the formation of a task force of the American Professional Society on the Abuse of Children, the leading professional society of professionals who deal with child abuse and neglect. Its 2006 report, mentioned above, concluded that “attachment parenting techniques involving physical coercion, psychologically or physically enforced holding, physical restraint, physical domination, provoked catharsis, ventilation of rage, age regression, humiliation, withholding or forcing food or water intake, prolonged social isolation, or assuming exaggerated levels of control and domination over a child are contraindicated because of risk of harm and absence of proven benefit and should not be used.” The report cautioned child welfare systems not to tolerate any such techniques by foster or adoptive parents. It also stated that “[p]rognostications that certain children are destined to become psychopaths or predators should never be made based on early childhood behavior.” It also condemned “intervention models that portray young children in negative ways, including describing certain groups of young children as pervasively manipulative, cunning or deceitful.”
Some adults are simply not suited to raise challenging children. Yet, agencies desperate to get children adopted, especially children with special needs in foster care, have placed children with such parents despite red flags, or even returned them after abuse was uncovered. In an extreme case in 2016, the 12-year-old adopted daughter of Eugenio and Victoria Erquiaga ran away from home. Neighbors found her with her hands zip-tied and her feet bound. She reported that she was locked inside a small playhouse for long periods of time with no bathroom. The story became national news and it became known that the parents had sought help from a mental health counselor who oversaw a program called “Radical Healing,” which no longer exists. The state charged the parents with child abuse. However, they then offered to drop all of the charges and expunge their records if the Erquiagas agreed to take their daughter back into their home, which they did. The girl ended up in a group home after she turned 18.
Twenty years since the APSAC report, children continue to suffer and die because they have been diagnosed by “experts” or parents with RAD or “attachment disorder.” To prevent more damage to children, state governments must adopt policies to ensure that all adoptive parents are adequately vetted. Agencies must be prepared to screen out potential adoptive parents who lack the patience, self-control and emotional intelligence to raise challenging children, and those who might be susceptible to practitioners offering controversial methods involving harsh discipline and physical restraint to cope with behaviors stemming from previous trauma or deprivation. In 2012, a committee led by Washington’s child welfare agency and children’s ombudsman published a Severe Abuse of Adopted Children Committee Report, which made several recommendations for improving assessment of assessing prospective adoptive families. These included strengthening qualifications for individuals conducting adoption home studies and post-placement reports and enhancing minimum requirements for these home studies and reports.
Training and ongoing support must also be provided to those adoptive parents who are deemed capable of accepting the challenge of raising children with histories of trauma and deprivation. These parents must be prepared to understand the needs and possible behaviors of the children they adopt, given their backgrounds. They also must be educated about the existence of parenting practices and therapies which are not supported by research and potentially harmful to children. And finally, they need ongoing support. The need for a greater investment in post-adoption services has been publicized by authorities like the Donaldson Adoption Institute (now closed) in its major report, Keeping the Promise: The Critical Need for Post-Adoption Services to Enable Children and Families to Succeed. Even RAD parent advocacy organizations like Attach Families Inc. are also asking for ongoing support.
Parents caught confining, starving, or otherwise abusing their children through adherence to “attachment therapies” must receive a criminal trial. This is, not only to ensure that justice is done, but also to provide an understanding of the factors that allow such tragedies to occur. The failure to try cases of parents who were obviously responsible for the torture and death of a child is a national stain and must be addressed.
That vulnerable children who have already been traumatized or deprived in early childhood in have met suffering or even death in licensed foster or adoptive homes should be a source of shame to all Americans. It is time to put an end to the suffering of children who have suffered enough. These tragedies can and must be prevented.
Just before this article went to press, the author became aware of media reports about the arrest of the adoptive parents of a 15-year-old boy, who for the past ten years has been locked in his bedroom for most of the day with no access to food, water or a bathroom. The adoptive father is a former employee of the El Paso County, Texas sheriff’s office. So far there has been no information about the genesis of the situation and whether a diagnosis or behavioral problem was involved. But it seems that hardly a week goes by without news of an egregious case of abuse against and adopted child. There is no time to waste in taking action to prevent more such suffering and damage to children.
This post was edited on June 24, 2025 to add a reference to the Washington report on severe abuse of adopted children and its recommendations and again on June 26 and 27 to correct several small errors and typos.
by Emily Putnam-Hornstein (University of North Carolina at Chapel Hill), Sarah Font (Pennsylvania State University), and Brett Drake (Washington University in St. Louis).
I am honored to publish this post by three of the leading academic researchers in child welfare. As often is the case in this blog, they are writing about the flawed use of data to support the user’s claims about a policy or program. In this essay, the authors discuss last year’s testimony by Indiana’s deputy director of child welfare services claiming success for the state’s family preservation program in reducing foster care caseloads without compromising child safety while also reducing racial disparities.
On May 22, 2024, the U.S. Senate Committee on Finance held a hearing titled “The Family First Prevention Services Act (FFPSA): Successes, Roadblocks, and Opportunities for Improvement.” The testimony was striking for its still-aspirational tone 6 years after the law passed and its sanitized depiction of why children enter foster care. As researchers, however, the statistics offered by Indiana’s deputy director of child welfare services, David Reed, caught our attention. Reed’stestimony indicated that FFPSA and associated investments in intensive family preservation services and concrete supports had produced: (1) a 50% decline in the state’s foster care caseload, alongside improved child safety; and (2) a two-thirds decrease in racial disparities among children entering foster care.
These claims are striking and beg the question: How?
On their very face, such dramatic numbers should invite skepticism. Despite continued efforts to move “upstream,” empirical studies of maltreatment prevention programs generally generate null or small effects. But one way for an agency to achieve a rapid reduction in foster care caseloads is to increase the threshold for intervening, leaving children in environments from which they would have been previously removed.
Below, we review data for Indiana and conclude that available evidence does not support the testimony offered.1 This is problematic not only for Senate Committee Members, but also the field at large. Bold causal claims based on flawed interpretations of data too often lead policymakers, and the public, to conclude that there are easy fixes to complex problems.
Reducing Entries to Foster Care and Improving Child Safety
The ideal way to reduce foster care entries is by reducing the community incidence of child abuse and neglect. Other than a brief drop during the COVID-19 pandemic, and despite investments in voluntary programs such as Healthy Families Indiana, referrals to Indiana’s child maltreatmenthotline were largely stable pre- and post-FFPSA implementation (i.e., 168,919 in 2017 vs. 172,077 in 2023). There is no evidence of a decrease in suspected maltreatment identified by community members.
Of note, data indicate that Indiana is now screening in a smaller percentage of referrals (75.0% in 2017 to 57.9% in 2023). Certainly, it is possible that Indiana was responding to allegations of maltreatment that were unwarranted. Indiana issued guidance in 2021 designed to change the state’s response to allegations of “educational neglect.” But if such changes led to the reduction, one would expect that as more “low-risk” referrals were screened out, children who were screened in would have higher risk and a greater share would be identified as victims requiring services.
Yet that is not what the data show. Among children who were screened in, the number of substantiated victims declined by roughly 30% between 2017 and 2023. This decline is particularly notable, given that during this same period, overdose deaths in Indiana were increasing and parental substance abuse is one of the most well-established risk factors for child maltreatment. It would appear that in addition to reducing the number of children who received a response, Indiana also increased its threshold for substantiating maltreatment. Importantly, changes in substantiation thresholds affect not only overall child victim counts, but also the federal measure of repeat maltreatment, which is the indicator of safety cited in Reed’s testimony. The easiest way to document improvements in child safety is to raise the bar for substantiation, thereby reducing both the initial victim count and the likelihood of identifying repeat incidents.
Short of successful efforts to reduce the incidence of maltreatment in the community at large, a second way an agency could theoretically—and safely—reduce the number of children in foster care is by expanding efforts to prevent placement by providing more families with effective services and resources. Yet once again, Indiana’s data show that fewer rather than more children reported for maltreatment have received in-home services. State data suggest a reduced number of children receiving in-home services in absolute numbers (Figures 1 and 2, Table 1) and no change in the proportion (Figure 3). Moreover, as depicted in all three figures and consistent with screening and substantiations, steep declines in in-home services and foster care caseloads began in 2017, before FFPSA was implemented.
A third possibility is that the services provided have become more effective, thus reducing the rate of children entering foster care. Yet the major program touted by Reed in his FFPSA testimony—an intensive family preservation program called Indiana Family Preservation Services—appears to have no effect on removal and a near-zero effect on repeat maltreatment.2 Indeed, the program is described as having “0 favorable effects” by the federal clearinghouse for evidence-based programs. There is simply no way to attribute a 50% foster care reduction to Indiana’s prevention services.
Finally, because the number of children in foster care is a function of the number of children entering care relative to the number of children exiting care, an additional possibility is that Indiana found ways to transition children out of its foster care system faster or in greater numbers. However, foster care entries declined from 12,826 in 2017 to 6,212 in 2023. underscoring that the bulk of the 50% caseload reduction likely stemmed from fewer entries.
Decreasing Racial Disparities
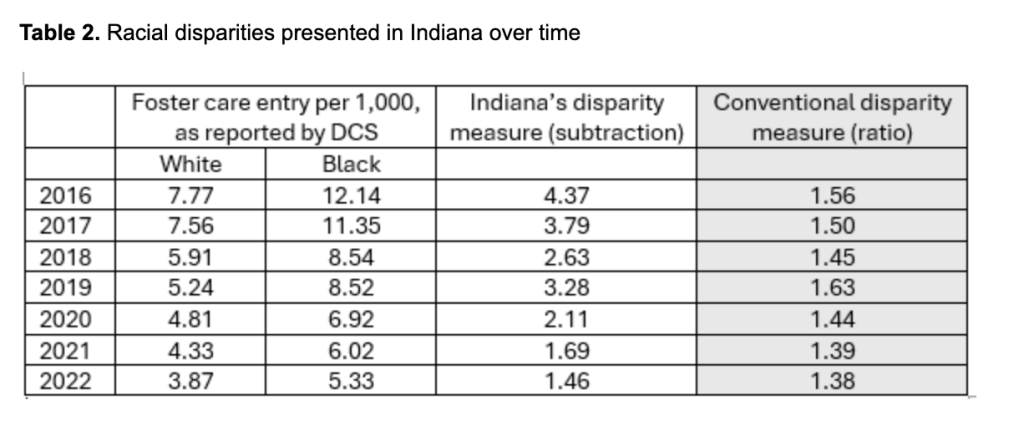
Senate committee members also heard about data suggesting that Indiana’s Black–White disparity in foster care entries declined by two thirds. The statistics presented, however, were quite unusual. The typical approach—both in the health literature and as a longstanding practice in child welfare—is to measure disparities as a ratio of rates (known as relative risk). In the context of the testimony presented, this would have been presented as the Black foster care entry rate divided by the White foster care entry rate.
But this is not what was used.
Rather, Indiana’s numbers were presented as the subtracted difference: the Black foster care entry rate minusthe White foster care entry rate. The problem with this approach is that it is very sensitive to base rates. Imagine that rates of removal were 10 per 1,000 Black children and 1 per 1,000 White children, then those rates decreased to rates of 1 per 1,000 for Black children and 0.1 per 1,000 for White children. In both cases, the relative risk of removal is 10 times higher for Black children than White children (a 0% change in disparity). But using Indiana’s subtraction-based measure, it would appear that the disparity declined from 9 to 0.9: a 90% reduction.
Using the conventional disparity ratio formula, the Black–White removal rate disparity declined only slightly in 2021–2022 compared with 2016–2017—a reduction of roughly 12%, not the “66.9% decrease” indicated in Reed’s testimony (see Table 2).
Summary
Available data do not support testimony that FFPSA implementation and Indiana’s Family Preservation Services program led to a 50% decline in foster care cases. Likewise, any reported improvements in child safety are likely an artifact of changed thresholds for classifying child maltreatment victims. We also believe that this testimony indicating dramatic reductions in racial disparities is quite overstated.
Of course, it is always possible that we have misunderstood the numbers Reed referenced—which is why we contacted him almost a year ago and shared our analysis. We received no response. If there is additional data that supports the testimony provided, we hope it will be made available. Until then, it is only reasonable to conclude that the striking claims made do not hold up to even modest scrutiny.
Note: On June 3, 2025, the IndyStar published an op-ed by Emily Putnam-Hornstein and Sarah Font summarizing the analysis in this post.
Notes
Regarding data published by Indiana’s Department of Child Services, we relied on publicly available information published as of June 2024 to align with what would have been available at the time this testimony was prepared. We also used data submitted by Indiana and found in the annual Child Maltreatment Reports. We focused on trends from 2017 (before FFPSA) through 2023 (the most recent year available). ↩︎
To elaborate, the intervention produced no “direct effect” on children entering foster care (i.e., no statistically significant reduction occurred in placements among families who were served). Published research has indicated that the intervention may have led to a small reduction in repeat maltreatment. To be generous, Indiana officials might argue that despite no direct effect on removals, the reduction in repeat maltreatment led to reduced removals over time. However, the estimated reduction in repeat maltreatment is only 4%, meaning that any indirect effects on removals cannot be more than this 4%. It is also worth noting that the declines in foster care caseloads began long before the program was implemented at any scale in Indiana. ↩︎
In a post dated January 10, 2025, I reported that 40 percent of investigations conducted by the District of Columbia’s Child and Family Services Agency (CFSA) in Fiscal Year(FY) 2024, which ended on September 30 2024, were “incomplete.” But by annual rather than quarterly data, that post actually understated the magnitude of the problem, which has worsened in the first half of FY 2025. The percentage of investigations that were terminated with a finding of “incomplete” increased to 65 percent in the second quarter of FY2025. The number of substantiated investigations has increased, while foster care placements and in-home case openings have not kept up with the apparent need for services.
The number of reports to child abuse hotlines varies by season, with reports tending to drop off during the summer when schools are closed and then increase again when schools re-open, along with fluctuations during the school year. Thus, data for part of a year should be compared to the same period of the preceding year. As shown in the table below, the number of reports to the CFSA hotline increased by from 11,945 in the first half of FY 2024 to 12,342 in the first half of FY 2025. The number of reports accepted for investigation actually decreased from 2,197 to 1,973, mostly because the hotline was screening out more of them. Nevertheless, the number of investigations conducted increased from 1,774 to 2,089. Thus, there were more reports, fewer reports accepted, and more reports investigated in the first half of FY 2025 than in the same period of the previous year. The reasons for these changes are unknown.
Table 1: Data for First Half of 2025 Compared to First Half of 2024
An investigation can have several findings. “Substantiated” means that the investigator (with approval from their supervisor) has concluded that the allegation of maltreatment (or risk of maltreatment) is supported by the evidence. “Unfounded” means there is insufficient evidence to support the allegations. “Inconclusive” means there is some evidence that maltreatment occurred but not enough evidence to support it definitively. “Incomplete” is defined as “an investigation finding for referrals in which there were barriers to being able to complete every aspect of the investigation. This could include obtaining confirmation during the investigation that the family was a resident of another state outside D.C., the parent refusing the social worker access to the home to complete a home assessment, or inability to locate the family.” (For the complete definitions, see the Investigations Page on the CFSA Dashboard). It is important to note that “Incomplete” refers to a finding upon closure of an investigation. It is not refer to an investigation that is ongoing.
The total number of investigations increased from 11,945 in the first half of FY 2024 to 12,342 in the first half of Fiscal Year 2025, as Table 1 shows. And there were some big changes in the numbers of investigations that were incomplete, substantiated and inconclusive. The number of incomplete investigations skyrocketed from 456 to 1,305. The number of unfounded investigations dropped from 949 to 327. And the number of substantiated investigations increased from 267 to 377, which is a large increase of 41 percent. This reflects both an increased number of investigations conducted and an increase in the percentage substantiated from 15 percent to 18 percent.
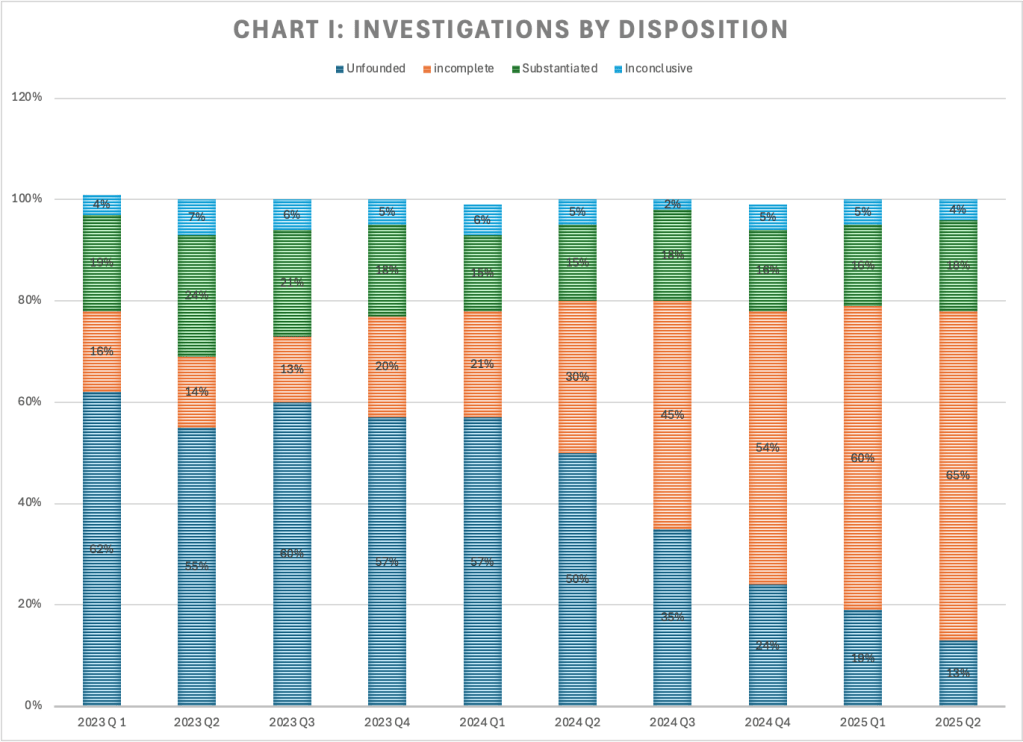
Chart I shows how the percentage of investigations by disposition has changed over the past nine quarters. The percentage of investigations that was incomplete (see the orange segments in the chart below) began to rise in the first quarter of 2024, when it jumped to 20 percent from 13 percent in the previous quarter. It rose to 30 percent in the third quarter of 2024, 45 percent in the third quarter, and 54 percent in the fourth quarter, 60 percent in the first quarter of 2025, and 65 percent in the second quarter of the current fiscal year.
As the percentage of investigations that are incomplete has increased, the percentage that are unfounded (dark blue in the above chart) has decreased–from 57 percent in the first quarter of 2024 to 13 percent in the first quarter of 2025. That drop of 44 percentage points happened at the same time as the percentage of investigations that were incomplete rose from 21 percent to 65 percent–an increase of 43 percentage points. It appears that investigations that would formerly have been closed as unfounded are now being closed as incomplete. CFSA did not respond to a request for the reasons for this change. The percentage of investigations that are substantiated has changed little since the first quarter of FY 2024.
Once an investigation is substantiated, CFSA may open a case for in-home services, or less often for foster care. As shown in Table I above, 169 in-home cases (each involving one or more children) were opened in the first half of FY 2025, compared to 125 in the first half of FY 2024. And 96 children were placed in foster care in the first half of FY 2025 compared with 110 in the first quarter of FY 2024. Unfortunately these two sets of numbers are not comparable as each in-home case can involve more than one child. But with substantiated reports increasing by over 100, in-home cases increasing by only 44, and foster care removals decreasing, it appears that some of the families with substantiated reports in 2025 are not receiving any CFSA services at all, and that is concerning. Perhaps some of these families are being referred to the collaboratives for services, which are less intensive and delivered by staff with lower credentials. And it is possible that some of these investigations may culminate in an informal kinship placement, but that means no services are provided to the parents or the children.
Clearly the staffing crisis with which CFSA (along with other agencies around the country) is struggling is responsible for the increase in incomplete investigations, and perhaps for the reduced percentage of substantiated cases receiving services as well. At the oversight hearing on February 13, 2025, Interim Director Trice pointed out that the number of investigative social workers has dropped from 100 to below 40. It is no surprise that CFSA’s oversight responses documented that most investigative workers had caseloads above 15. the maximum caseload allowed by CFSA’s Four Pillars Performance Framework. Average caseloads for the 38 investigative workers in the first quarter of FY 2025 were 30 or higher for 10 workers and 20 or higher for a total of 20 workers.
Director Trice reported that the agency is making do by diverting workers from the In-Home units to Investigations, but that is not a good solution. Families with in-home cases are often deeply troubled, with long histories of chronic neglect. According to CFSA’s 2023 Child Fatality Report, two children died while their families had open in-home cases. We cannot afford to divert these critically needed workers. Moreover, it is possible that the diversion of in-home workers to investigations may be part of the reason that in-home case openings did not increase more given the increase in substantiations. With workers not available to handle these cases, the agency may be more reluctant to open them.
What can be done? Creative solutions are needed. It may be necessary to temporarily reduce licensing or degree requirements through a special waiver due to the staffing crisis. Former Director Robert Matthews spoke of obtaining permission from the Board of Social Work Examiners to use workers with Bachelor of Social Work degrees to help investigators (not carry cases), but this plan was not mentioned in this year’s oversight responses. The agency might consider recruiting federal workers who have lost their jobs for these positions. Recruiting retired police officers and military veterans is another idea that has potential. A partnership with local schools of social work, as Maryland and other states maintain, is long past due. Those who agree to take jobs and remain for a given amount of time should receive loan forgiveness and perhaps housing as well. In a housing-hungry citizen, this could be a game changer. CFSA needs to think outside the box to resolve the staffing crisis.
CFSA’s Dashboard data for the first half of FY 2025 raises more questions than it provides answers. The most striking trend is the continuing explosion in the percentage of investigations that were incomplete–which was 65 percent in the second quarter. Also concerning is the failure of in-home case openings and foster care placements to keep up with increased substantiations. Like many other child welfare agencies, CFSA has been devoting much time and attention to programs outside of its core functions, like the warmline and family success centers. In this time of budget stringency and looming recession, it is time for CFSA to focus on its ability to perform its most basic and important function–child protection.
Proposed federal budget cuts to child welfare services might hurt New Jersey’s recent progress in child welfare, the Commissioner of New Jersey’s Department of Children and Families told state legislators last month. The anticipated reduction of more than $100 million would force the department to “revert to its most basic role — that of child protection — not prevention, not support or empowerment, just surveillance and foster care,” DCF Commissioner Christine Norbut-Beyer told members of the state Senate’s Budget Appropriations Committee. The relegation of child protection–or “surveillance and foster care”–to the “most basic” version of child welfare is telling. DCF’s Commissioner, like many other progressive child welfare administrators, no longer views child protection as the primary purpose of child welfare services.
For those who regularly read this blog, the devaluation of child protection and foster care by a high-level administrator over child welfare will not be a surprise. There has been a sea-change in child welfare over the past decade. The mainstream view of the purpose of child welfare has shifted from responding to child abuse and neglect to “upstream prevention.” And why not? Why wait until children are abused and neglected if we can prevent the maltreatment altogether?
There is no denying that ideally, it is better to prevent maltreatment than to respond to it. But the services that are discussed as prevention are mainly in the province of other agencies. In seeking to broaden child welfare services through the Family First Act, Congress added mental health, drug treatment, and parenting training. While the latter can be seen as a function of child welfare, drug treatment and mental health are separate systems. There has been increased emphasis on cash and housing and other antipoverty benefits as child maltreatment prevention; we have large programs to address these problems–much larger than the child welfare system. Even some of the “prevention services” that DCF and other state agencies have adopted, like “Family Success Centers,” provide a wide array of place-based services, most of which do not fall into the traditional orbit of child welfare and would be most appropriately funded jointly with other agencies.
If “prevention” could abolish the need for child protection, then there would be no need for child protection agencies. But we know that no amount of “prevention” (at least as envisioned by today’s child welfare establishment) will eliminate child abuse and neglect. We are often talking about patterns of mental illness, drug abuse, family violence, and poverty that have persisted over generations. And then there are families that are not poor or characterized by generations of dysfunction but where a parent’s mental illness or disordered personality makes them incapable of safely raising children. As Jedd Meddefield describes in his brilliant essay called A Watershed Perspective for Child Welfare, “As critical as it is to fully consider upstream factors, it would be wrong not to do all we can to help children who lack safe families today.
But the fact is that many of today’s child welfare leaders like Norbut-Beyer appear not to be interested in child protection and foster care. They often disparage the “reactive” role of child protective services in contrast to the “proactive” nature of prevention. Many agencies have reactive missions–police, firefighters, emergency rooms–and one could argue these are the most important services of all because they save lives. The analogy with the police is revealing. Police react to allegations of crime just as child welfare agencies react to allegations of child abuse and neglect. To prevent crime, we must not rely on the police, who are overburdened already and not trained and equipped to provide the services needed. Instead we must turn to a whole host of agencies dealing with education, public health, mental health, housing, income security and more–the same agencies that we must mobilize if we want to prevent child abuse and neglect. Nobody is saying that the police need to address the underlying causes of crime.
Norbert-Beyer’s use of the word “surveillance” as a synonym for child protection is telling indeed. She clearly doesn’t see CPS investigators as heroes who go out in sometimes dangerous and certainly uncomfortable circumstances to protect children–and maybe even to save them. It’s not surprising because we have all been told that saving children is not what child welfare is about.1 And foster care? Norbert-Beyer boasts that New Jersey has the lowest rate of child removal in the country, and children who are removed more often than not go to relatives. She’s not very interested in the quality of care these vulnerable young people receive or in all the things her agency could do it improve it, like establishing foster care communities (like Together California) to house large sibling groups or investing in cutting-edge models of high-quality residential care.
When the person who is in charge of child protective services in a state that is acknowledged as a leader in the field calls it “surveillance,” and relegates it along with foster care to “basic” functions that hardly deserve mentioning, it’s hard to have faith that the crucial mission of child protection will be implemented with the passion it deserves. Norbert-Beyer’s comments illustrate the prevalent thinking that leads to the diversion of resources from crucially needed child protective services and foster care to “prevention services” that are and should be provided by other agencies.
See for example this statement from Casey Family Programs, which includes the words “We must continue to evolve from an approach that seeks to “rescue” children from their families to one that invests in supporting families before abuse and neglect occur.” One of the first messages I was given as a CPS trainee is that my job was not to save children. ↩︎
Ten-year-old Begidu Morris died more than three years ago of horrific child abuse by his parents, who adopted him from Ethiopia. But there was no avalanche of media coverage of his death, no interviews with shocked neighbors saying they had no idea the child even existed. No pyramid of teddy bears and flowers outside his home. No arrests of those who tortured and murdered Begidu, and no demonstrations demanding justice. No anguished commentaries from experts on how we failed and what could be done to prevent such tragedies in the future. There is not even a picture of Begidu by which we can remember him. If not for a child fatality summary released by the Florida Department of Children and Families (DCF) two years after Begidu’s death, nobody outside the family, a few neighbors, and a small group of medical, social service, and law enforcement professionals would have known that it happened.
According to the DCF child fatality summary, Begidu Morris collapsed at home in Lee County, Florida, on March 17, 2022 and was transported to Golisano Children’s Hospital. He was diagnosed with subdural hematoma, hypothermia, cardiac arrest, acute respiratory failure, retinal hemorrhages, and metabolic acidosis.Begidu was placed on life support and died on March 22, 2022. Examination showed bruising to Begidu’s head and significant scarring to his buttocks. Begidu weighed 44 pounds, which was in the 0.1 percentile for his age. An autopsy determined that the cause of death was “complications of hypoxic ischemic encephalopathy due to craniocerebral trauma” and the manner of death was homicide.
The CPS investigation
Begidu lived with his adoptive parents, Jack and Consuela Morris, and their biological son. Their two other biological children were in college and returned home for vacations. Begidu and his biological sister were adopted from Ethiopia by the Morrises, when he was about two years old. His sister’s adoption with the Morris family disrupted and she was re-adopted by another family in 2019. After Begidu’s death, the family quickly obtained a lawyer and was “minimally cooperative” with the CPS and police investigations.
The family’s three-bedroom home was described by the investigator as “pristine.” In addition to the master bedroom and the teenage sibling’s room, the third bedroom served as a guest room for the two adult siblings when they returned home from college. Begidu slept in a small closet, where investigators discovered a pile of urine-soaked clothing on a rollaway bed. The door to the closet was locked from the outside and was monitored by a camera. The closet had no ventilation and there were no toys or personal possessions indicating that a child lived there. Begidu’s adoptive parents claimed that he engaged in behaviors such as temper tantrums and fecal smearing.
The CPS investigation concluded that “[a]lthough it was not able to be determined with certainty who inflicted the injury/injuries that led to this child’s death, it can be concluded that the parents either participated in the abuse that led to the child’s injuries and subsequent death, or they participated in concealing the horrific abuse and neglect that he suffered.” It found the parents Jack and Consuelo Morris responsible for Begidu’s death and for “bizarre punishments,” internal injuries, physical injuries, medical neglect, “failure to thrive/malnutrition/dehydration,” failure to protect, and inadequate supervision.
Deaths due to child abuse or neglect are the tip of the huge iceberg of child maltreatment, most of which remains unseen by the public. All of these deaths should be examined, not only to determine whether maltreatment occurred and who was responsible, but also to identify systemic issues that might suggest policy changes to protect other children. Yet, the investigation summary I received showed a complete lack of curiosity and interest by DCF in drawing lessons from this terrible case and making them available to the public.
Isolation is a common element of severe and chronic child abuse cases. Begidu was clearly isolated. He had not visited a medical provider in three years. Most neighbors were unaware that the child even existed. And perhaps most important, he was not attending school–at least not in person. The Investigation Summary contains three different statements about Begidu’s and his adoptive brother’s schooling, stating in one place that the brother was enrolled in Lee County Schools and Begidu was not, in another place that both were homeschooled, and in two different places that each was enrolled in “virtual school.” DCF did not respond to my request to know which statement was correct. Yet this is crucial information.
If Begidu was enrolled in school virtually, it would have been incumbent on the investigator to contact the school and ask about his attendance and any interactions with Begidu and his family. This would be important in establishing if there was any negligence on the part of school staff or any need for policy changes. If Begidu was not in school at all, the question would be whether the state was aware he was being homeschooled. Homeschooling parents in Florida must provide one-time notice to the local superintendent, maintain a portfolio of their children’s work, and turn in an annual assessment by standardized test or portfolio evaluation. We need to know if Begidu’s parents complied with these requirements, and how he fell through the cracks if they did not.
With the lack of protective educators to respond to Begidu’s plight, DCF should have wanted to know if there were any opportunities for his situation to be brought to the attention of other protective adults. While the Morris family had no history with CPS in Florida or in Michigan, where they adopted Begidu, there may have been an occasion when the abuse in this home could have come to light. Begidu’s sister was re-adopted by another family in Florida in 2019. One cannot help wondering if the sister was the previous target of abuse in the home, thus leading to her adoption by another family. In his medical chart from a primary care visit in 2018 or 2019, there was a note that Begidu said he was “going to be just like his sister.” (These may be the only words of Begidu’s to be recorded).
Fully 19 lines of text about Begidu’s sister are redacted from the Investigation Summary, which says only that she lives in another state and had no contact with Begidu or the Morris family. It is likely that the redacted information concerned the circumstances behind the disruption of the sister’s adoption. Did the sister report any concerning treatment to her new adoptive parents? Did anyone involved in the second adoption have information that should have been reported and investigated? Was a coverup part of the new adoption arrangement? Unfortunately, DCF denied my request for this information. DCF appears to have no interest in learning from Begidu’s death and sharing the implications of what they have learned with the wider community in the interests of protecting children in the future.
Whatever the flaws of the investigation were in terms of uncovering systemic issues, DCF ultimately found Begidu’s parents to be responsible for Begidu’s death and the horrific abuse and neglect that preceded it. But shockingly, the agency decided not to remove Begidu’s adoptive brother from the home. According to the case summary, the teenager reported feeling safe in the home, and “sources familiar with the child” reported no concerns for his safety. (One wonders who these sources were and what they knew about Begidu’s abuse.) The investigator also noted that the teen “appeared physically healthy, was enrolled in virtual school, and was visible in the community, including attending a Mixed Martial Arts program several times weekly. He had his own fully furnished bedroom, and he was allowed to have relationships with others outside the home, including his adult siblings who were away at college.” It is clear that this decision did not come easily. According to the investigation summary, “[W]hile it is concerning that [Begidu’s sibling] remains in the home, it should be noted that he does not share the same vulnerabilities that were present with his younger sibling.” This is quite a statement. Apparently, this child was considered “safe” in the home of where his brother suffered unspeakable abuse and died, because he himself was not ill-treated. There was not even a services case opened to make sure that he received therapy for the trauma he has endured.
The criminal investigation
Three years after Begidu’s death, the police have made no arrests in the case. The DCF Investigation Summary states that CPS was involved in multiple meetings, including with the State Attorney’s Office (SAO) and that
“[u]ltimately no action was taken by the SAO as the perpetrator of abuse could not be determined based on the information that was available at the time of their staffing. There were two individuals (the mother and [the brother]) in the home capable of causing the head trauma to the child; the individual responsible for the abuse could not be determined.
The lack of charges is almost incredible. If they could not have charged anyone with the actual homicide, it is hard not to understand how the parents could not have been charged with multiple counts of child abuse, charges that surely exist in Florida as they do in other states. It is hard not to ask the question, as one child advocate put it, could this happen if Begidu were White? The State’s Attorney denied my request for the investigation records on the grounds that “there is still an active investigation.” But it is hard to believe that the police are still seriously working on this case.
Adoptions and Severe Abuse
Begidu’s story has similarities with the stories of other children adopted from overseas or from foster care. Few readers could have forgotten the six Hart children, adopted from foster care in Texas, who were starved, beaten, and eventually killed in a 2018 murder-suicide by one of their adoptive mothers. In 2013, a Washington State couple were convicted and sentenced to decades in prison in the death of their Ethiopian adopted daughter, Hanna Williams, who died of hypothermia in 2011 after being forced to sleep outside in the rain. Her malnourished body was covered with bruises and scratches and her brother testified that their adoptive parents beat them and deprived them of food. A Pittsburgh couple was sentenced in 2014 for endangering the welfare of two children they adopted from Ethiopia through withholding food from their six-year-old son and causing abusive head trauma to their 18-month-old daughter. In a dispiriting echo of Begidu’s case, the adoptive mother was sentenced to six to 12 months in jail with daily work release to enable her to go home and care for her biological children. The mother who re-adopted these children saw this sentence as “an indication that the court viewed adopted children as different, since it decided that a woman who abused her adopted kids could be trusted with her biological children.” In 2021, a woman in Washington was charged with second-degree criminal maltreatment for beating and starving a 12-year-old boy that she and her husband adopted from Ethiopia. The prosecution decided to drop the case, as reported by KUOW, stating that the boy had “suffered mental health challenges which will prevent him from testifying.” The child had been re-adopted by one of his schoolteachers, who saw his abuse and came to an agreement with his parents–a possible hint to what may have happened with Begidu’s sister.
The vast majority of adoptive families provide loving homes, and a study from the Netherlands suggests that adoptive families are less likely to maltreat their children than birth families. Nevertheless, observers have noted clusters of cases of severe abuse of adopted children. Such a cluster was noted in the State of Washington at the time of Hanna Williams’ death. A committee led by Washington’s child welfare agency and children’s ombudsman in 2012 published a Severe Abuse of Adopted Children Committee Report, which discussed 15 cases of adopted children who had suffered abuse at the hands of their adoptive families. There was a common pattern of concerning parenting practices in these cases, including physical confinement, withholding food, isolation (including withdrawal from school), forcing the child to remain outside the home; and disparaging remarks about the child. The committee observed that these cases tend to occur “when an adoptive family is ill-prepared or ill matched with a child that suffers from unidentified and/or untreated trauma, abuse, and/or neglect.” The analysis suggests that families may respond to their adopted children’s difficult behaviors caused by past trauma by using punishments like sending a child to bed without dinner, which in turn triggers further behaviors, leading to a vicious cycle of behaviors and punishments culminating in egregious abuse.
The Washington committee made multiple recommendations for avoiding such tragedies in the future, including better oversight of child-placing agencies, strengthening the assessment of prospective adoptive families, and improved training for parents and adoption professionals, and post-adoption support services for families. Some of these recommendations required legislation and other required agency action, and it is not clear whether any of them were implemented.
The trial of Larry and Carri Williams for the death of their adopted daughter, Hannah, was a major event in Washington, with Seattle-area Ethiopians attending proceedings every day, “almost as a vigil” as the Seattle Times described it. But with no arrests in Begidu’s case and no media coverage until two years later, Florida’s Ethiopian community may not even be aware of it. Holding Begidu’s adoptive parents accountable won’t bring him back, but the lack of any meaningful response to his death is an offense to all child victims of abuse and neglect and those who care about them. The only thing that can be done now is to hold his torturers and murderers responsible and learn from his suffering to prevent other children from sharing it.
The original version of this post was published on April 4, 2022.I decided to update and re-publish it after reading a press release from Prevent Child Abuse America stating that “PCAA’s signature home visiting program, Healthy Families America, has been proven to reduce child abuse and intimate partner violence while improving long-term health and educational outcomes.”While I cannot evaluate the claim about domestic violence, the post below show that Healthy Families America has not been “proven” to reduce child abuse.
I have written before about the power of wishful thinking and how it causes people to disregard research and real-life results. A program called Healthy Families America (HFA) offers a good example of the power of wishful thinking. The nation’s oldest and largest charity (now called Prevent Child Abuse America or PCAA) dedicated to the prevention of child abuse launched HFA based on weak evidence that a program in Hawaii could prevent child maltreatment. The first experimental study of the Hawaii program found no impact on child maltreatment but did nothing to derail the launch of HFA, which grew into the centerpiece of PCAA. Studies of HFA programs around the country have found little evidence of reductions in child maltreatment, but the program has continued to grow. The story of HFA is a lesson in the power of wishful thinking and the failure of evidence (or lack thereof) to counteract it.
As told in a helpful history of home visiting, all modern programs can trace their origins to Henry Kempe, whose book, The Battered Child, brought about the recognition of child maltreatment as a national problem. To address child abuse, Kempe called for universal prevention through a network of home health visitors. Inspired by Kempe, modern home visiting began with Hawaii’s implementation of the Healthy Start Project (HSP) in 1975. HSP was developed on the island of Oahu. It had two components: early identification (at the birthing hospital) of families with newborns at risk of child abuse and neglect and home visiting by trained paraprofessionals for those families classified as at-risk who agreed to participate. This initial program was never evaluated, but anecdotal information suggested it was successful in promoting effective parenting, and six similar programs were established on neighboring islands.
The Hawaii Legislature authorized a three-year pilot program focusing on one neighborhood in Oahu, which began in 1985. There was no control group in the pilot study, and the researchers used CPS reports and changes in family stress in participating families to measure program effectiveness. During the three-year pilot, there were few reports of physical abuse, neglect or imminent harm for program participants. Because evaluations of other home visiting programs had found much higher rates of reported maltreatment in comparison group families, these results were viewed as evidence that the program had a positive impact. According to the authors of the first rigorous evaluation of HSP, “The pilot study results might have been given too much weight, given the lack of a control group and the short period of follow-up for most families.” Nevertheless, the results of this unpublished study were enough evidence for the Legislature to expand HSP throughout Hawaii starting in 1989.
Home visiting in general was gathering steam in the 1980s and early 1990’s. In 1990, the U.S. General Accounting Office (GAO) issued a report promoting home visitation as a “promising early intervention strategy for at-risk families.” In its summary of research evidence, GAO focused mostly on health and developmental benefits for children, rather than maltreatment prevention. In 1991, the U.S. Advisory Board on Child Abuse and Neglect issued a report recommending a pilot of universal voluntary neonatal home visitation, stating that the efficacy of home visiting as a preventive measure was “already well-established.” The Board cited the results of a federally-funded demonstration begun 17 years earlier as well as the the nurse home visitation program started by David Olds in 1977. But HSP was not mentioned.
Despite the lack of a rigorous evaluation, the National Committee to Prevent Child Abuse (NCPCA, now called Prevent Child Abuse America), which bills itself as the nation’s “oldest and largest organization committed to preventing child abuse and neglect before it happens,” had become interested in using HSP as the nucleus of a national home visiting program. But first, NCPCA conducted a one-year randomized trial of HSP. The trial suffered from severe methodological limitations, including “less than ideal followup,” differential dropout rates in the program and control groups, the failure to blind interviewers to experimental or control status, and reliance on program staff rather than researchers to measure some outcomes. Nevertheless, the trial concluded that HSP reduced child maltreatment, and this apparently gave NCPCA the assurance it needed to invest in the model.
NCPCA launched Healthy Families America in 1992, with financial support from Ronald MacDonald House Charities. Rather than impose a single service model, HFA was based on a set of principles or critical elements, which included initiation of services prenatally or at birth, assessment of the needs of all new parents in the target area, voluntary nature of services, at least weekly services for families with the highest needs, availability of services for three to five years, comprehensive nature of services, and cultural competence, among others. The typical HFA program included an assessment of all new or first-time parents in a given community at the time their babies are born or prenatally.”
In the meantime, the Hawaii Department of Health recognized the limitations of both the pilot study and the NCPCA study and initiated a more rigorous evaluation of HSP in 1994. This was a randomized controlled trial, with at-risk families identified at the hospital and randomly assigned to the experimental and control groups. In 1999 the results of the Evaluation of Hawaii’s Healthy Start Program were released as part of an issue of the Future of Children journal containing evaluations of six different home visiting models. No overall positive program impact emerged after two years of service in terms of child maltreatment (according to maternal reports and child protective services reports). Early HFA evaluation results, published in the same issue, also failed to find effects on abuse and neglect in three randomized trials, which included the HSP evaluation discussed above and another Hawaii HSP study.
David Olds had had begun testing his Nurse Home Visiting Program in 1977 and already had long-term results on the program in Elmira, NY, as well as shorter-term results for a replication in Memphis, Tenn. That program, now known as Nurse Family Partnership, was very different from HFA. It was restricted to first-time teenage mothers and the home visitors were nurses rather than paraprofessionals. The nurses followed detailed protocols for each visit. The researchers found that among low-income unmarried women (but not other participants), the program reduced the rate of childhood injuries and ingestions of hazardous substances that could be associated with child abuse or neglect. Follow-up of the Elmira group when the children were 15 found that the nurse-visited mothers were significantly less likely to have at least one substantiated report of maltreatment. These results are particularly impressive because they overrode a tendency for nurse-visited families to be reported for maltreatment by their nurse visitors. The researchers concluded that the use of nurses, rather than paraprofessionals, was key to the success of the program.
In their analysis of all six studies published in the Future of Children volume on home visiting, Deanna Gomby et al. concluded that while the HFA and HSP evaluations showed some change in maternal attitudes and self-reported behaviors related to abuse and neglect, only the Nurse Home Visiting Program showed impacts on abuse and neglect other than from self-reports. Gomby and her co-authors also concluded that the results of all six home visiting evaluations were discouraging for those who had high hopes for home visiting for solving an array of problems. All the programs “struggled to enroll, engage and retain families.” Program benefits generally accrued to only a subset of enrolled families and were often quite modest. The authors explained the disappointing results by concluding that human behavior is hard to change, particularly when problems are community-wide. They recommended that “any new expansion of home visiting programs be reassessed in light of the findings presented in this journal issue” and stated that home visiting services are “best funded as part of a broad set of services for families and children.”
But the home visiting juggernaut was already in motion nationwide. And NCPCA, renamed Prevent Child Abuse America in 1999, had already made HFA its centerpiece program. Home visiting grew, and HFA grew with it. In 2010, Congress created the Maternal, Infant and Early Childhood Home Visiting Program (MIECHV), which was re-authorized in 2018 with funding of $400 million per year through FY 2022. HFA is one of the models that are most frequently implemented with MIECHV dollars. Home visiting programs can also receive funding through Medicaid, Title IV-B and IV-E of the Social Security Act, and many other funding sources. HFA now serves over 70,000 families per year at an average cost of over $3,000 for a family in its first year of home visiting.
The infusion of funding for HFA research resulted in a multitude of research projects (both randomized trials and less rigorous studies) and resulting publications. Nevertheless, research has yet to find solid evidence that these programs have an impact on child maltreatment: The California Evidence-Based Clearinghouse for Child Welfare (CEBC), the pre-eminent child welfare program clearinghouse, reviewed 19 research reports on HFA. Its website as of April 2022 gave the program a rating of “4” on a scale of 1 to 5 for prevention of child abuse and neglect, meaning the evidence fails to demonstrate that HFA has an effect on abuse and neglect. Interestingly, that rating no longer appears on the CEBC website, but the earlier version is preserved by the Wayback Machine. As of April 2025, HFA is no longer listed at all in the CEBC’s document titled Home Visiting Programs for Prevention of Child Abuse and Neglect. When I emailed the CEBC to ask about the missing rating, I received an email stating that Healthy Families America “is still currently under review in the Prevention of Child Abuse and Neglect topic area. The rating for this topic area was pulled from the website during the rereview process. Some programs take longer to review due to the amount of research and other factors.”
HFA was not designed to work with families that have already been found to abuse or neglect their children but that did not stop child welfare agencies from spending federal and state funds delivering HFSA to families under the Family First Prevention Services Act (FFPSA). Despite the lack of evidence of its impact on maltreatment, HFA received a rating of “Well Supported” from the clearinghouse established by FFPSA to determine whether a program can receive federal funding under Title IV-E of the Social Security Act. To get such a rating, the program must show improved outcomes based on at least two randomized trials or rigorous quasi-experimental studies. But these outcomes could be any sort of “important child and parent outcome,” (not just reduction of child abuse or neglect) and there is no standard for how to measure each outcome. Based on its review of all HFA studies that met their criteria for inclusion, the Clearinghouse found 23 favorable effects, 212 findings of no effect, and four unfavorable effects across 16 outcomes. This included five favorable effects on child safety based on parents’ self-reports of maltreatment, with no favorable effects on other measures of child safety. Self-report is generally frowned upon as a measure of child maltreatment, for obvious reasons. A positive impact of HFA might reflect that participants in HFA were more eager than control group members to provide the “right answer” to questions about maltreatment.
The “well-supported” rating from the Title IV-E clearinghouse allowed states to spend Title IV-E funds on services to families with a child welfare in-home case. To take advantage of this new market, HFA announced in September 2018 that families referred by the child welfare system were now able to enroll as long as the child in question was 24 months of age or younger, as opposed to the original requirement that services start at or before birth. To serve these families, HFA introduced special child welfare protocols. HFA advertises these protocols on its website, stating that “HFA’s evidence and the flexibility of enrollment make HFA a great prevention choice for states and child welfare organizations seeking to strengthen families and reduce the number of children placed in foster care.” (Note that there is no mention of reducing abuse and neglect!)
Today, the diversity of HFA programs makes evaluation of the program as a whole impossible. According to the website, “HFA puts communities in the driver’s seat. Local HFA programs are able to choose their eligibility criteria, parenting materials, and hire the staff they deem best to do the job. With the amount of flexibility offered, HFA has been able to be successfully implemented in a wide variety of communities.” It is hard to imagine what the evaluation of one HFA program means about the effectiveness of other programs under the same name.
Critical examination of the HFA website shows that the organization skews its portrayal of available research to present it in the most favorable light and avoids direct statements that the program prevents child abuse and neglect. On its Evidence page, HFA claims the “highest rating possible from CEBC in the category “Home Visiting Programs for Child Well-Being,” without mentioning that in the category “Home Visiting Programs for the Prevention of Child Abuse and Neglect,” HFA is currently unrated after the statement that it was unable to demonstrate an effect was removed. The page goes on to group the effects of HFA into three categories, stating that participants “build nurturing relationships with their children,” “champion their children’s health and development,” and “cultivate a flourishing future for their family.” Reductions in abuse and neglect are not mentioned in the description of how parents “build nurturing relationships with their children.”
It is disappointing that an organization that defines its mission as child abuse prevention, decided to fund HFA before it was proven to prevent child maltreatment and continued with this commitment even after the disappointing evaluations of 1999 might have led them to diversify their investment. That PCAA continues to use charitable contributions made for the prevention of child abuse and neglect to fund a program that has not been proven to accomplish this goal, raises serious ethical questions. Twenty-three members of the 45-person staff (which has grown by five staff in three years !) listed on the Prevent Child Abuse website have duties linked to Healthy Families America.
The story of HFA is not an unusual one. I have written about the similar disregard for evidence in the promotion of models such as Homebuilders and blind foster care removals. Such stories are all too frequent. They show us how wishful thinking can drive leaders to disregard research, especially after they have made a premature decision to commit to one program or course of action.
The Texas Department of Family and Protective Services has reported a dramatic decline in child maltreatment fatalities from 199 in FY 2021 to 99 in FY in 2024. Perhaps most surprising about the purported decline in fatalities is that it occurred alongside a massive drop in the number of children placed in foster care from 16,028 in Fiscal Year 2021 to 9,623 in Fiscal Year 2022, with similar numbers of children placed in 2023 and 2024.
Supporters of recent changes in Texas law regarding child maltreatment were quick to highlight these findings as evidence that foster care can be greatly reduced or eliminated with no adverse effects on child safety.
But these claims do not stand up under careful scrutiny. Changes to policy and practice can result in dramatic year-to-year changes in official counts of child maltreatment fatalities, and Texas has implemented at least three significant policy or practice changes during this period.
First, a Texas law that took effect September 21, 2021 tightened the definition of neglect to require the presence of “blatant disregard” for the consequences of an act or failure to act that results in harm to the child or that creates an immediate danger to the child’s physical health or safety. This new requirement means that deaths that would have been attributed to maltreatment prior to the law change are now not investigated at all or not confirmed as maltreatment. Indeed, DCF cites this changed definition as one cause of the decline in reported fatalities between FY 2021 and FY 2024.
Child fatality numbers were also affected by a practice change implemented by DCF that involves the way the agency handles reports of child fatalities. Previously, DCFS assigned all child death reports it received for a full investigation. But starting in September 2022, reports to the Texas Child Abuse Hotline that involve a child fatality but include no explicit concern for abuse and neglect are treated as “Case Related Special Requests,” requiring field staff to confirm that the reporter or first responders had no concern for abuse or neglect. If there are any concerns for abuse or neglect, the child fatality is then sent for a full investigation, but otherwise there is no further action. DFPS reports that the number of child fatalities it investigated decreased from 997 in FY2022 to 690 in FY2023 and 587 in FY 2024. DFPS attributes this decline in investigations to both this practice change and to the legislature’s change in the definition of neglect.
There is one newer policy change that DFPS announced in its recent report. Investigations that are closed “with a disposition of reason to believe for neglect with a fatal severity code” receive a further level of review. It seems possible that this level of review may be reducing the number of reported cases even further.
Given all these policy and practice changes affecting the count of child maltreatment fatalities, It seems highly likely that Texas did not see an actual reduction in these deaths, but rather reclassified them as not due to child maltreatment. Perhaps it is not surprising that neither DFPS nor the supporters of weaker child protection are interested in exploring what is really happening to vulnerable children in the aftermath of the drastic decline in the use of foster care.
This post was originally published as a guest commentary in the Baltimore Sun.
Last month, the Baltimore Banner reported on an alarming rise in the number of child fatalities due to maltreatment in Maryland, as shown by a federal report. The number of child abuse and neglect deaths reported by Maryland to the federal Children’s Bureau was 83 for Fiscal Year 2023, up from 27 a decade before, a rate higher than any state but Mississippi.
After initially responding with confusion, the Maryland Department of Human Services (DHS) explained that the numbers it reported to the feds were erroneous. Actually, the state was aware of 47 children who died of abuse or neglect in 2023, which was still a 75% increase from 2013. “We continue to discover where data was routinely released without any validation or reconciliation,” a deputy DHS secretary told the Banner.
But members of the legislature were already alarmed and began talking about withholding funds until the agency was able to report accurate data about child fatalities as well as the conditions of children in foster care. Eager to demonstrate its desire for transparency, DHS announced that it was pivoting to support a bill requiring the agency to promptly release information about children in foster care who die from suspected maltreatment.
But this legislation would not apply to children who died while in the custody of their parents or guardians. It would not apply, for instance, to five-year-old Zona Byrd, who starved to death last year after being returned to her parents’ custody; four-year-old Amir James, who arrived at the hospital covered in cuts and bruises and died from skull fractures that caused his brain to bleed, while his twin brother survived similar injuries; 16-month-old Zavier Giron, who had several broken ribs, a dislocated femur and a perforated intestine when he died; and two-year-old Charlee Gamble, who was shot in the head by an unsecured gun that her father purchased illegally and left on a TV stand. The bill would apply only to cases of abuse or neglect in foster care — even though they are a rare occurrence. Indeed, less than 1% of perpetrators of child maltreatment fatalities reported nationwide for Fiscal Year 2023 were foster parents or staff of a group home or residential treatment facility.
The chair of the Maryland House Judiciary Committee conducting a hearing on the bill wondered if the bill was too narrow, but one of the sponsors, Del. Susan McComas, responded, “Whether it’s a little step or a big step, I don’t really care. I think we need to do something. And I think we could start with just this.”
The sentiment to do something is admirable, but in this case it will likely not even make a dent in the lack of public accountability and transparency when children die of maltreatment.
To prevent such tragedies, we need improved data collection, timely notification and greater transparency by agencies that investigate such fatalities and are responsible for protecting children. Maryland should pass a bill that requires prompt notification of any child fatality that has been reported to child protective services. Eleven other states already do this. Without such notifications, legislators and the public may never know about some child abuse deaths, especially those that did not result in criminal charges. In addition, DHS should be required to respond promptly to requests for further information about all suspected child maltreatment fatalities, not just those where the child was in foster care or state custody. It is only by achieving such transparency that DHS can work with the legislature, researchers and child advocates to prevent these tragic events in the future.
Recognizing implicit bias in mandated reporting training is a national focus for addressing racial inequity in child welfare. States from New York to Washington have updated their training for mandatory reporters to include implicit bias or highlight the distinction between neglect and poverty in an effort to reduce racial disparities in child welfare involvement. My recent experience taking the updated training in Washington DC made clear that there is a fundamental conflict between preparing mandated reporters for their responsibility to report and advising them to assess their biases before reporting. The basic conflict is this: the core training instructs mandatory reporters to report any suspicion of abuse or neglect, while the implicit bias unit urges mandatory reporters to doubt their instincts and reconsider their duty to report.
In FY 2023, the District of Columbia’s Child and Family Services Agency (CFSA) updated its online mandated reporter training to include a module focused on understanding and addressing implicit bias for mandated reporters. This training is required for all mandated reporters, who include both professionals (doctors, nurses, teachers, social workers, etc.) and volunteers who work with children. I had taken the training several times in the past–first for my work as a social worker with CFSA and later as a mentor to a foster youth. I had my first experience with the updated training last month as part of my preparation to serve as a Court Appointed Special Advocate (CASA) for a child in foster care.
The Implicit Bias Module
The implicit bias module appears to have been shoehorned into the existing DC mandatory reporter training right after a brief introduction to mandatory reporters and their role. The video introducing the section explains that implicit bias harms “families of color” in the child welfare system, without providing any evidence of such harm. It goes on to assert that “the point of this portion of the training is to make sure that reporting is based on observations and not assumptions. Ultimately we want mandated reporters to consider this before responding to a child’s disclosure of suspected abuse or neglect: Do I have any implicit bias in my decision to call or not to call the hotline.” It may sound reasonable, but as the training unfolds, a conflict with the goals of the overall training and mandatory reporting itself becomes clear.
The implicit bias module continues by explaining that nationally and in DC, mandated reporters call the CFSA hotline about Black families disproportionately more than White families; this leads to more “Black and Brown” children having in-home cases or entering foster care because they are assessed more closely. A graph has been provided, with text saying “In this graph, disproportionality is where you see that Black and Brown children make up approximately 64% of hotline calls. However, only 57% of people in the District are a race/ethnicity other than white.” Unfortunately, one does not see this in the graph, which does not include hotline calls at all! It does include children who are the subject of an investigation after a call to the CFSA hotline, and it shows that Black children made up 57 percent of the investigated children, while comprising 53 percent of the population. That is a very small disparity, and in any case could reflect unequal rates of abuse and neglect between Black and White children. The data does show a larger Black-White disparity in confirmed maltreatment (71 percent of the children confirmed as maltreated are Black) and “foster care” (whether this is children in care or entries into care is unclear) at 92 percent. But these increasing disparities come in at the investigation stage (where the substantiation and foster care decisions are made), not at the reporting stage, calling into question the need for training mandatory reporters about implicit bias. To make matters worse, the data on investigations contain a whopping 40 percent without race or ethnicity data; 26 percent of the confirmed maltreatment data, and 23 percent of the in-home case data also lack race and ethnicity information. (Note that the bars of the graph have been shifted by one column to the left of the corresponding columns from the numerical table, as in the original.) So it is impossible to draw meaningful conclusions from these data.
Source: DC Mandated Reporter Training, Lesson 3, page 6, available from
Other than the mention of the hotline call data, which is missing from the graph, the only analysis of the data in the text reads as follows. “Disparity occurs when these children and families have cases open to either in home or foster care support. As you can see that [sic] 85% of in-home cases, and more than 92% of foster care cases in 2020 were opened with Black and brown families, while again the District’s make-up is only 57% Black and brown.” The inclusion of “brown families” is somewhat disingenuous. The graph shows that Hispanics and Asians, the only “brown” children with non-zero populations on the graph, are underrepresented in investigations, confirmed maltreatment, foster care, etc.1 Switching categories, the lecturer goes on to state that “At every stage, Black and Indigenous families face racial discrimination and unequal treatment.” DC is not known to have a large indigenous population; there is no row on the table for Native Americans, and Native Hawaiians and Pacific Islanders are zero percent of every category except that they are listed as making up two percent of children aging out of foster care in 2019.
A central motif of the training is that the confusion of poverty with neglect contributes to the racial and ethnic disparities in child welfare. The video states that “under current law, most children in the US are separated for neglect, a code word that typically represents conditions of poverty, resulting in disproportionate separation and harm to Black families….” But there is a problem with this. We know that neglect is often associated with serious drug abuse and/or mental illness. After all, most poor people don’t neglect their children. Moreover DC Code Section 16.2301 forbids a court to find maltreatment when the deprivation of food, clothing, shelter or medical care is due to the parent’s lack of financial means. The law does not allow removing children because of poverty in DC, and the small number of removals compared to investigations in DC (224 children placed in foster care compared to 3,767 investigations in FY 2024) suggests that CFSA does not remove children for poverty alone.
The training includes practice scenarios to help trainees distinguish between poverty (or “need” according to the training) and neglect. The participant must read the scenarios and decide whether they represent need (and presumably do not call for a hotline report) or neglect. After providing their own answer, trainees learn the “right answer” according to CFSA. One of the three “need” scenarios is particularly troubling and is reproduced here:
The 4-year-old child came into the center smelling of a strong smell and her nails are long and dirty. There is sticky stuff on her chest that is black underneath her shirt on her skin. The child often comes to the center unbathed. She was wearing shoes that were too small, but the dad was made aware, and he got her new shoes. The child comes in with an old pamper not changed, soaked or soiled. Sometimes she comes to school with the same clothes on from the day before or sometimes wears the same clothes for three days.
The child does not talk or engage with staff or peers. The mother has been observed yelling at the child and all she does is cry. The child covers her eyes but does not ask for anything.
The caller is aware that the family was recently evicted after the mother lost her full-time job and they are being supported on the income made from the father’s part-time employment. The family moves from the homes of family and friends because they refuse to go to a shelter. Caller suspects sometimes the family may sleep in the car.
The characterization of this scenario as “need” rather than neglect is troubling. The combination of factors that are cited suggest something more than poverty. The fact that the child “does not talk or engage with staff and peers,” and that the mother “has been observed yelling at the child and all she does is cry” suggest problems this beyond the realm of need. The refusal to go to a shelter under current conditions, when the District of Columbia guarantees shelter to families with children and has replaced its dilapidated shelter with modern new facilities, increases the likelihood that this is a case of neglect.
In the content that follows, a video tells mandatory reporters that although they are required by law to report suspected abuse or neglect, they should not make reports “solely based on assumptions, schemas, or biases.” It seems rather disrespectful to think that a doctor, nurse, teacher, social worker or volunteer would do this. Trainees are presented with the following questions to ask before making a report.
This is confusing indeed. Is the agency saying that mandatory reporters should not make a report “solely out of legal obligation,” even though they are legally required to report and could receive consequences for not doing so? Providing resources to assist the family is fine, but if there is abuse or neglect, does that exempt the reporter from the duty to report? It seems unlikely and unwise.
“Granted,” the presenter continues, “there are many times when you recognize your legal obligation, have the resources to support a family, and have checked your biases, and a report still needs to be made.” But the speaker goes on to state that “Each of us holds a responsibility to address disproportionality and disparity in the lives of Black and Brown families in the District.” She then invites us to “walk through how we can do this together,” by listening to two videos that are a total of five minutes in length. The first video, on “Mitigating Bias” counsels reporters to follow a three-step process consisting of of “deliberate,” “reflect,” and “educate,” with each step containing mutiple steps or suggestions. Mandatory reporters then learn about “cultural humility” and its three attributes: “lifelong learning and critical self-reflection,” “recognition and challenging of power imbalances,” and “institutional accountability.” And then training participants are told that “[u]ltimately, our goal is to ensure that children who are experiencing neglect in the District receive the support they need to thrive within their families. To do this effectively, we each have to ensure our implicit biases, whether personal or institutional, are not the foundation for calls to the CFSA hotline.” Apparently, no children in the District need to be removed from their families in order to thrive; even though the agency providing the training removed 244 children in the last Fiscal Year, as mentioned above.
To sum up, the implicit bias section of the training teaches child-serving professionals and volunteers that mandatory reporting harms Black children and that to avoid that harm, mandatory reporters must engage in a lengthy deliberative process before making a report. Mandatory reporters learn nothing of the costs of not making a report, which include the possible death of a child. They also learn nothing about the different risks facing Black children, who are three times more likely than White children to die of maltreatment.2 Instead, they are told that “we are delinquent in addressing the institutionalized racism and bias that pervades our family and wellbeing systems. This has been perpetuated by the misconception that we are nobly rescuing children from dangerous situations.” The clear implication is that making a report is much more risky than not making one.
A Case of Mixed Messages
After at least an hour of training on implicit bias, mandatory reporters finally arrive at the original training, which seems mainly unchanged. They learn about how to respond to a child’s disclosure of abuse or neglect. They learn they must report when they have reasonable cause to believe a child has been, or is in immediate danger of, being abused or neglected. They learn what and how to report. They learn that the identity of reporters is confidential and that failure to make a report can be punished by a fine of up to $1,000 or imprisonment for up to 180 days. They learn about different types of abuse and neglect, which children have higher risks of being maltreated, situations in which CFSA does not intervene, what happens when a report is made, and how child welfare services work in the District of Columbia. They are told to “[r]eport any suspicion of child abuse and neglect,” and that “every call matters!” A key instruction is buried in the section on how to distinguish discipline from child abuse. It says: “The good news is, as a mandated reporter, you do not need to know the details or all the facts before making a report. You just need to be suspicious of abuse/neglect and CFSA’s response, if it does respond, will do the rest.” (This should be moved to the top and emphasized, as it may have been in an earlier version of the training). In closing, trainees are told that:
Abuse and neglect place children at great risk of physical and emotional injuries and even death. As a mandated reporter, the District is expecting you to do the following:
Recognize the signs of child abuse and neglect.
When children have the courage to disclose abuse or neglect to you, take them seriously.
When you suspect or know of incidents of child abuse or neglect, call CFSA at (202) 671-SAFE.
Be responsible for calling the CFSA Hotline yourself, even if you have informed your supervisor.
If necessary, be helpful and available during the investigation.
The fundamental conflict between the training’s two messages is clear. According to the original training, abuse and neglect are dangerous to children and it is our responsibility to report. According to the implicit bias section, it is reporting that is dangerous and needs to be inhibited. Neglect is a serious type of maltreatment according to the original training but a “code word”d according to the implicit bias section. It is not really surprising that the implicit bias element of the training seems to be in opposition to the preexisting content. Perhaps those who inserted this content would prefer to eliminate mandatory reporting training entirely and are just trying to minimize it within the requirements of current law. But the half-measure of trying to train the implicit bias out of mandatory reporters creates a training that simply does not make sense.
In addition to this fundamental disconnect, the training exhibits many factual errors and is padded with extraneous content. The factual errors are discussed in an addendum to this post. The extraneous content includes discussions of the racial wealth gap and instructions for “self-reflection, in which trainees are instructed to define their values by a three-step process that is painstakingly described in a three-minute video. Perhaps the most striking extraneous content is a section that describes in detail six types of “mental models related to diversity, equity and inclusion.” One of the six types is “active opposers,” who are typically deeply rooted in their choice to be a strong opponent of DEI. These are the people whose minds cannot be changed and who are committed to disrupting the work of DEI.” One cannot help wondering how the current federal leadership would respond if they knew of this content, and being offended at the disrespect for the time of busy professionals or volunteers.
In summary, there is a fundamental conflict between the original message of CFSA’s mandatory reporter training and the message of the implicit bias unit that has been added to it. Unlike the original message stressing the duty and importance of reporting suspected abuse and neglect, the new message states that reporting damages children and families of color and should be avoided whenever possible. This fundamental conflict is not unique to the District and by necessity affects all mandatory reporter trainings that attempts to temper the duty to report by inserting considerations related to race and ethnicity.
From U.S. Children’s Bureau, Child Maltreatment 2023, page 59. States reported that 6,04 per 100,000 Black children were found to be victims of a child maltreatment fatality compared to 1.94 per 100,000 White children. These are deaths that have been confirmed as due to maltreatment by child protective services, medical examiners, or police, a process that may be affected by bias. ↩︎
Addendum: Factual Errors in CFSA’s Mandatory Reporter Training Implicit Bias Module
The implicit bias module in CFSA’s mandatory reporter training curtains numerous factual errors and omissions. Here are a few.
“National studies by the US Department of Health and Human Services reported that minority children and in particular black children are more likely to be in foster care than receive in-home services even when they have the same problems and characteristics as White children.” I asked the CFSA’s Communications Director for a citation and I found the exact language in one of the three references that were provided–a 2019 ABA brief entitled Race and Poverty Bias in the Child Welfare System: Strategies for Child Welfare Practitioners. A footnote referred readers to an essay by Dorothy Roberts for PBS’ Frontline program. That essay in turn attributes the same quote to “a national study of child protective services by the U.S. Department of Health and Human Services” with no citation. When consulted, ChatGPT references the outdated 1996 National Incidence Survey of Child Abuse and Neglect, which has been superseded and contradicted by the more sophisticated study published in 2010.
“Rates of child abuse are not higher for children of color than white children. People of color do not treat their children worse than White families do. Racial disproportionality in CW is due to systemic racism, cultural misunderstandings, stereotypes, and biases that influence the decision to report alleged child report or neglect to CPS.” This is simply not true. First, we don’t have definitive evidence of child abuse rates as it occurs in secret, may not be reported, and investigations may not come up with the right results. But all the evidence we have indicates that Black families do abuse and neglect their children more than White families. This is likely due to the history of slavery and racism, which led to higher poverty and concentration in impoverished neighborhoods characterized by crime, substance abuse, unemployment, and limited community services, as well as a legacy of intergenerational trauma associated with these factors as well.
“Although African American families tend to be assessed with lower risk than White families, they are more likely to have substantiated cases, have their children separated, or be provided family based safety services.” I could not find any resource on the internet that indicates that Black families tend to be assessed with lower risk than White families It is true that Black children tend to have more substantiated cases, have their children removed, or receive in-home services. But that is before controlling for family characteristics that affect risk. The only research article cited by CFSA actually reported that when they controlled for family risk factors, agency and geographic contexts, and caseworker characteristics, Black children were not at significantly higher risk of substantiation or removal.